

Introduction
Despite its reputation for technical precision and operative control, surgery consistently exposes professionals to both physical and psychological occupational risks, many of which remain insufficiently recognized. International research indicates that these risks are not isolated events but recurrent features of daily practice: intense physical strain, prolonged maintenance of static postures, and the repetitive execution of identical surgical gestures are frequently associated with musculoskeletal pain, particularly in the cervical and lumbar regions [1, 2]. Bibliometric studies published over the past decade reveal growing scientific interest in this issue, with a marked increase since 2016 [3]. Research conducted in Spain reported a prevalence exceeding 90% for musculoskeletal pain among surgeons, with some cases requiring medical treatment that led to temporary absenteeism or presenteeism. Identified contributing factors include excessive duration of surgical procedures, elevated body mass index, and inappropriate positioning of laparoscopic screens [4].
In addition to physical discomfort, surgical practice involves other categories of occupational risks with a significant impact on health. Biological and chemical hazards, exposure to radiation, and surgical smoke, which may contain toxic compounds such as phosgene, combine with chronic stress and psychological pressure, requiring a more sophisticated assessment than simple direct observation [5].
In daily practice, surgeons face a set of complex risks, often masked by professional pressure. The application of a well-designed questionnaire, tailored to the specifics of their practice, enables the transformation of subjective perceptions into quantifiable data, with both clinical and preventive value.
Over the past decade, the questionnaire has emerged as a refined tool capable of capturing subtle aspects of surgeons’ professional activity [6]. One line of research employs predictive algorithmic models to estimate the individual risk of developing injuries, integrating objectively measured ergonomic parameters and providing personalized physiotherapeutic recommendations [4]. Recent literature also describes initiatives to design questionnaires tailored to operating theatre staff, psychometrically validated and rigorously tested for reliability and internal consistency [7, 8].
In the Republic of Moldova, occupational health remains largely focused on workplaces in the real sector, while the healthcare sector is insufficiently explored. The absence of specialized institutions, the lack of dedicated indicators, and the inexistence of a coherent monitoring system significantly reduce prevention capacity [9]. In this context, the initiative to develop a rigorous questionnaire for surgeons is not merely a research exercise but a strategic step towards strengthening occupational health at the national level.
Data published in recent years indicate worrying trends: both occupational mortality and morbidity among healthcare workers are on the rise, resulting from exposure to physical, chemical, biological, and psychosocial factors [10-13]. For surgeons, daily exposure to surgical smoke and intense stress constitutes a distinct risk profile; under such conditions, the use of well-calibrated assessment tools enables the objective quantification of exposures and early intervention [14].
At the national level, the creation and validation of such a questionnaire would open concrete prospects: it could become the first tool tailored to the specifics of surgical practice in the Republic of Moldova, with immediate applicability in hospital settings; it could serve as the basis for a standardized register of occupational risks, useful both for epidemiological surveillance and for informing public policies; and it could be integrated into the training of occupational medicine specialists, providing a practical approach to real rather than purely theoretical risks.
The aim of the research is to develop and validate a tool tailored to assess occupational risk factors among surgeons.
Material and methods
A sequential mixed-methods design was used, comprising a qualitative phase to explore the dimensions of the work environment and occupational risk factors present in surgeons’ workplaces. The data obtained were thematically analyzed to identify relevant domains and indicators, which formed the basis for drafting the questionnaire items.
Subsequently, a quantitative phase was conducted with the aim of psychometrically testing the pilot version of the questionnaire. This involved administering the instrument to a sample of active surgeons selected through convenience sampling. Sociodemographic data were collected, along with responses to items addressing working conditions, exposure to occupational factors, general health status, and psycho-emotional state.
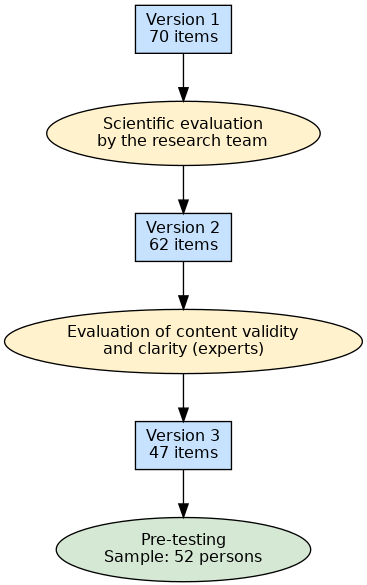
The first version of the questionnaire, developed by the working group, comprised 70 items. This version underwent scientific review by the research team, resulting in a second version containing 62 items. The latter was then submitted to experts for content validity and clarity assessment. Consequently, the third version of the questionnaire consisted of 47 items and was pre-tested on a sample of 52 surgeons (Fig. 1).
|
Fig. 1 Stages of the questionnaire evaluation. Note: item = question. |
The results formed the basis for developing items that measure the perceived impact of occupational factors on health status. The quantitative phase aimed to examine the reliability and validity of the measurements in a subset of practicing surgeons employed at the time of the study, conducted between December 2024 and May 2025 in the Republic of Moldova. The instrument was developed according to the following multi-stage process:
Literature review and identification of key components
In the initial stage of developing the questionnaire, our aim was to gain a thorough understanding of the occupational risk factors that may affect surgeons’ health. To this end, we reviewed the current scientific literature, selecting relevant studies from the fields of occupational health, ergonomics, work psychology, and preventive medicine.
Analysis of these sources revealed that surgeons are frequently exposed to a range of occupational factors with a negative impact on both physical and mental health. The most commonly reported include uncomfortable posture maintained for prolonged periods, constant stress linked to decision-making responsibilities, long working hours, lack of sleep, exposure to biological or chemical agents, and difficulty maintaining a work–life balance [5, 14, 15]. Consequently, we identified four key domains considered essential for assessing occupational risks and their effects on health: working conditions, occupational risk factors, general health status, and psycho-emotional state.
Based on these domains, an initial version of the questionnaire was drafted, formulating items intended to reflect as accurately as possible the daily reality of surgeons. At this stage, we relied both on data from the literature and on the observations and recommendations of specialists with experience in practical surgery and occupational hygiene.
Conceptualization and development of the instrument
After identifying the key domains relevant to the study’s objective, we proceeded to develop the questions and scales for each domain, taking into account the realities and specific features of the professional context in the Republic of Moldova. At this stage, our aim was to cover as accurately as possible the essential aspects of surgeons’ work, ensuring that the instrument reflected their real experiences and challenges.
Initially, a total of 70 items were formulated, structured as follows: (i) 8 questions on respondents’ sociodemographic data; (ii) 38 items relating to working conditions and occupational factors (e.g., work environment, schedule, physical and mental demands); (iii) 11 items on general health status; and (iv) 13 items on psycho-emotional state.
The construction of this questionnaire was based on a multidimensional perspective on professional culture and on how psychosocial and occupational factors influence surgeons’ behaviour and well-being. We drew inspiration from the international scientific literature [16] and adapted the concepts to the local context to ensure the instrument’s cultural validity and practical relevance [17, 18].
The first version of the questionnaire was finalised in December 2024 as the result of a collaborative process between public health researchers and medical professionals from the Republic of Moldova. The items were designed to capture the behaviours, attitudes, and subjective perceptions experienced by surgeons in their daily practice, both at the individual level and in relation to the work environment.
- Review by the research team and refinement of the instrument
The first version of the questionnaire underwent scientific review by the research team, resulting in a second version comprising 62 items. Accordingly, 8 items were removed due to ambiguous wording and redundancy.
Review by an expert panel and determination of the instrument’s content validity
Content validation is one of the initial and essential stages in the process of validating a measurement instrument. Its purpose is to determine the extent to which the items included in the questionnaire adequately and representatively reflect the concepts or domains the instrument is intended to assess. Content validity relies primarily on expert evaluation, and the quality of this stage depends significantly on the selection and engagement of the experts.
After developing the initial version of the questionnaire, the research team conducted a preliminary item analysis to identify elements with weak psychometric properties. Items with over 10% non-responses, high rates of abstention, or ambiguous wording were eliminated. As a result, the questionnaire was reduced from 62 to 47 items, this version being used for content evaluation.
For this stage, a panel of seven experts was assembled in relevant fields such as social medicine, occupational hygiene, medical psychology, and surgery. The team comprised two specialists in social medicine, biostatistics, and health management; two experts in occupational hygiene; one specialist in general hygiene; one surgeon; and one medical psychologist.
All selected experts had extensive experience in professional practice, higher education, and research. Their selection was based on demonstrated expertise in health services, occupational health, and work psychology.
Each expert was provided with the updated version of the questionnaire, and item evaluation was carried out independently. Experts were invited to assess the relevance of each item using a four-point ordinal scale, as recommended by Polit et al. [19, 20]: 1 = not relevant; 2 = somewhat relevant; 3 = quite relevant; 4 = highly relevant, and to assess the clarity of each item using a four-point ordinal scale: 1 = item is not clear; 2 = item requires some revisions; 3 = item is clear but needs minor revisions; 4 = item is very clear.
For the quantitative analysis, the content validity index for each item (I-CVI) was used. The rating scale was dichotomized: scores of 3 and 4 were considered "relevant" and "clear", while scores of 1 and 2 were classified as "not relevant" and "not clear". The I-CVI was calculated as the proportion of experts who rated the item as relevant and clear relative to the total number of experts.
To account for the possibility of chance agreement between evaluators, the modified Kappa coefficient (K*) was also calculated using the formula: K* = (I-CVI − pₐ) / (1 − pₐ), where pₐ represents the probability of chance agreement, calculated according to the binomial distribution.
According to the scientific literature, for a panel of more than six experts, a minimal degree of disagreement is acceptable. The accepted CVI threshold is at least 0.83 [19, 21].
In addition to the scores provided, the experts offered valuable suggestions regarding question formulation, language clarity, and questionnaire structure, most of which were incorporated.
The outcome of this stage was a revised version of the instrument, comprising 47 items, formulated to reflect as accurately and comprehensively as possible the professional reality of surgeons in the Republic of Moldova.
Data collection and evaluation of the instrument’s psychometric properties
To evaluate the psychometric properties of the instrument, we conducted a comprehensive statistical analysis focused on two main directions: item analysis and internal consistency (α), as well as content validity (CVI/Kappa) of the questionnaire.
Internal consistency (reliability)
Internal consistency reflects how well the items measuring the same concept are correlated. For this stage, Cronbach’s α coefficient was used, which is considered the standard in assessing the reliability of questionnaire-type instruments. In general, an α value ≥0.70 is considered acceptable, indicating good internal coherence among items [22-24].
Pilot testing
The questionnaire was tested on a subset of 52 surgeons, selected through convenience sampling from among those working in public healthcare institutions in the Republic of Moldova, taking into account their accessibility and willingness to participate in the study. The study population is specific, given that, according to statistical data [25], the total number of surgeons was 460. Participants were employed in public healthcare institutions (republican and municipal) in the Republic of Moldova. The inclusion criteria were as follows: (i) active status as a physician in a surgical department; (ii) informed consent to participate.
All participants signed an informed consent form. The questionnaires were anonymous, printed, and distributed individually, and completion was carried out in paper format. To ensure confidentiality, the questionnaires and consent forms were collected separately.
Ethical approval. The study was approved by the Research Ethics Committee of the Nicolae Testemițanu State University of Medicine and Pharmacy, approval no. 2 of 07.10.2024.
Data analysis. The results were presented as mean ± standard deviation (SD) for continuous variables and as absolute frequencies and percentages for categorical variables. Sociodemographic characteristics were described using frequency and percentage. Correlation was considered statistically significant when the p-value was less than 0.05. Cronbach’s alpha coefficient was also used to determine internal consistency. Statistical analyses were performed using SPSS Statistics 27 (SPSS, Inc., Chicago, IL, USA).
Results
Content validation of the instrument. The scale-level content validity index (S-CVI) was assessed using two complementary measures. The average score across all items (S-CVI/Ave) reflects the mean level of content validity for the instrument, whereas the universal agreement index (S-CVI/UA) indicates the proportion of items for which all experts provided concordant ratings. These indicators collectively capture the overall validity of the questionnaire in terms of both relevance and clarity (Table 1). The S-CVI/Ave values varied between 0.934 and 1.00 across the evaluated domains, with all domains exceeding the threshold for the S-CVI/Ave. For the S-CVI/UA, three domains scored ≥0.80, while the domain of occupational factors obtained 0.738 (relevance) – acceptable, but below the recommended threshold for unanimous agreement.
Table 1. S-CVI/Ave and S-CVI/UA for the four questionnaire domains of interest | ||||
Questionnaire domains | S-CVI/Ave* | S-CVI/UA** | ||
Relevance | Clarity | Relevance | Clarity | |
Data relating to working conditions | 0.976 | 0.988 | 0.833 | 0.917 |
Data relating to occupational factors | 0.934 | 0.971 | 0.738 | 0.885 |
Data relating to health status | 0.971 | 0.967 | 0.80 | 0.80 |
Data relating to psycho-emotional state | 0.986 | 1.00 | 0.90 | 1.00 |
Total | 0.959 | 0.966 | 0.817 | 0.824 |
Note: *S-CVI/Ave = Scale Content Validity Index, average method – the mean of the item-level content validity indices (I-CVI) for all items in the domain; values ≥0.80 indicate good content validity. | ||||
As shown in Table 2, the item-level content validity index (I-CVI) for relevance varied between 0.857 and 1.00. The corresponding kappa coefficients (κ*) indicated an excellent level of agreement among experts (κ* = 0.75–1.00). For the clarity assessment, I-CVI values ranged from 0.847 to 1.00, with κ* values confirming a similarly high level of consistency (κ* = 0.75–1.00). Following expert feedback, 24 questions were revised, and 15 items were removed to improve the instrument’s overall precision.
Table 2. I-CVI and Kappa* for the relevance and clarity of the questionnaire domains of interest | ||||
Questionnaire domains | I‑CVI Relevance | κ* Relevance | I‑CVI Clarity | κ* Clarity |
Data relating to working conditions | 1.00 | 1.00 | 1.00 | 1.00 |
Data relating to occupational factors | 0.857 | 0.848 | 0.847 | 0.849 |
Data relating to health status | 1.00 | 1.00 | 1.00 | 1.00 |
Data relating to psycho-emotional state | 0.868 | 0.851 | 0.857 | 0.889 |
Note: *κ represents the modified kappa agreement index; κ 0.75–1.00: excellent, κ* 0.60–0.74: good, κ* 0.40–0.59: acceptable, and κ* <0.40: poor. **I-CVI indicates the item-level content validity index | ||||
Internal consistency analysis. The internal consistency of the questionnaire was assessed using Cronbach’s α coefficient, which was applied to evaluate the homogeneity of the responses and the coherence of the research instrument. The overall Cronbach’s α coefficient for the entire questionnaire was 0.808, indicating a very good level of internal reliability and confirming that the items consistently measure the intended constructs.
At the section level, the coefficient ranged between 0.769 and 0.864 (Table 3). The sections "Working conditions" (α = 0.715) and "Occupational risk factors" (α = 0.782) demonstrated good and, respectively, high internal consistency, while "Psycho-emotional state" (α = 0.864) showed very good internal reliability. In contrast, the "Health status" section recorded a lower value (α = 0.769), still indicating good consistency, which may have been influenced by the diversity of aspects assessed.
Table 3. Internal consistency of the questionnaire and its sections | |||
Questionnaire section | Number of items | Cronbach’s α | Interpretation* |
Working conditions | 7 | 0.715 | Good internal consistency |
Occupational risk factors | 15 | 0.782 | High internal consistency |
Health status | 10 | 0.769 | Moderate internal consistency |
Psycho-emotional state | 7 | 0.864 | Very good internal consistency |
Entire questionnaire | 39** | 0.808 | Very good internal reliability |
| Note: *Interpretation of Cronbach’s α coefficient according to George and Mallery (2003): α≥0.9 – excellent; α≥0.8 – very good; α≥0.7 – good; α≥0.6 – acceptable; α<0.5 – inadequate. **The eight questions from the "Sociodemographic data" section were not analyzed. | |||
Pilot test
Sample characteristics. The socio-demographic characteristics of the participants involved in the pre-testing stage of the questionnaire are presented in Table 4. The respondents were aged between 32 and 58 years, with a mean age of 44.92 ± 6.36 (SD) years.
Table 4. Demographic and educational profile of respondents: pilot testing stage | ||
Characteristics | n | % |
Gender | ||
| 30 | 57.7 |
| 22 | 42.3 |
Marital status | ||
| 2 | 3.8 |
| 44 | 84.6 |
| 6 | 11.5 |
Place of residence | ||
| 48 | 92.3 |
| 4 | 7.7 |
Work experience | ||
| 2 | 3.8 |
| 14 | 26.9 |
| 14 | 26.9 |
| 20 | 38.5 |
| 2 | 3.8 |
Type of healthcare institution | ||
| 40 | 76.9 |
| 8 | 15.4 |
| 4 | 7.7 |
Note: n - absolute number; % - percent. | ||
As shown in Table 4, the majority of the 52 respondents in the sample were male (57.7%). It is noteworthy that most participants were from urban areas (92.3%) and were married (84.6%).
The questionnaire also included three open-ended questions, to which the respondents provided qualitative answers (Table 5).
Table 5. Results of responses to the three open-ended questions in the questionnaire at the face validity stage (n = 52) | |||
| n (%) | ||
Yes | No | Excluded from analysis | |
1. Please indicate the serial numbers of the questions in this questionnaire that are unclear or difficult to understand. | 38 (73.1) | 6 (11.5) | 8 (15.4) |
2. Please indicate the serial numbers of the questions that are clear. | 16 (30.8) | 28 (53.9) | 8 (15.4) |
3. Please suggest ways to improve the unclear or difficult-to-understand questions in this questionnaire. | 30 (57.7) | 14 (26.9) | 8 (15.4) |
Note: n - absolute number; % - percent. | |||
The respondents provided feedback on the open-ended question regarding the clarity and comprehensibility of the questionnaire items. Most respondents considered the questions clear and easy to understand. Some participants, however, noted that certain questions were personal, direct, and sensitive. It was also mentioned that some questions contained multiple sub-questions.
From the responses provided regarding ways to improve unclear or difficult-to-understand questions in the questionnaire, some participants offered valuable suggestions for refinement, such as adding the response option "not applicable", rephrasing certain questions, clarifying specific technical terms, and reducing or simplifying lengthy formulations. A frequent observation concerned the repetitiveness of some questions, particularly those related to occupational risk factors.
Of the 52 individuals who participated in the questionnaire, 8 did not comment on any item; therefore, these responses were excluded from the analysis.
Discussion
The results of the study highlighted a high content validity of the questionnaire developed to assess the working conditions, occupational risk factors, health status, and psycho-emotional state of surgeons. For all investigated domains, the S-CVI/Ave values exceeded the 0.80 threshold, while the I-CVI and κ indices were, for the most part, classified as "excellent". The level of agreement obtained among the evaluators is comparable to that reported by Rapisarda et al. (2020) during the validation of the "Mental Health Professional Culture Inventory" (MHPCI) [26]. In that study, the involvement of a multidisciplinary panel, combined with the application of standardized criteria, allowed for the exclusion of items with reduced psychometric properties and the strengthening of the relevant dimensions. Similarly, Beyera et al. (2020), in validating a questionnaire designed to analyse determinants of healthcare service utilization for low back pain, reported high values of content validity indices, emphasizing the essential role of rigorous item selection and formulation [27].
The overall internal consistency of the questionnaire (α = 0.808) indicates a very good level of reliability, comparable to the values reported for other multidimensional instruments. For example, Jafari-Golestan et al. (2024), in the validation of the "Post-Stroke Self-Care Activities" (PSCA), reported a general α of 0.901, with variations between 0.734 and 0.948 across domains [28]. Similarly, the Spanish adaptation of the "Self-Efficacy for Ostomy Adjustment Scale" (SE-OAM-SV) achieved a high α of 0.96, while the Arabic validation of the "Long-Term Conditions Questionnaire" (LTCQ) conducted by Al-Qerem et al. (2025) reported α values of 0.90 for the factor "Empowerment and Functional Wellbeing" and 0.83 for "Health-Related Psychosocial Distress" [29]. In the present questionnaire, α values ranged between 0.715 and 0.864 across domains, an interval that remains within the accepted limits. This variation reflects, as in the LTCQ, the diversity of the constructs assessed, with certain domains demonstrating greater homogeneity than others.
The pilot stage confirmed both the face validity and the level of acceptability among the target population. Most participants considered the wording of the questions clear and easy to understand; however, some suggestions for adjustments were also made, a finding consistent with other studies. In research within the fields of nursing and nutritional management, linguistic and cultural adaptations have been identified as essential factors for enhancing the comprehensibility and relevance of instruments [30, 31].
From a structural perspective, the results confirm a coherent organization of the questionnaire domains, comparable to the multidimensional architecture reported in other validation processes. This convergence suggests that, regardless of cultural context or the characteristics of the population studied, the multidimensional approach remains relevant for assessing experiences related to health and professional activity.
A distinctive feature compared with many instruments described in the literature, including the LTCQ, PSCA, and SE-OAM-SV, is the specificity of the target group. While those questionnaires were primarily designed for patients with chronic conditions, our instrument is aimed exclusively at a professional population exposed daily to well-defined occupational risk factors. This particularity justifies the inclusion of domains focused on the assessment of the working environment; an aspect rarely encountered in clinical instruments with a general applicability.
Nevertheless, the applied methodology, which encompasses content validity assessment, internal consistency analysis, and piloting, remains consistent with that used internationally, thereby confirming the universal nature of psychometric principles.
In terms of applicability, the literature emphasizes that rigorously validated instruments can be integrated into clinical practice, research, and public policy development. In the case of the "Long-Term Conditions Questionnaire" (LTCQ), the authors recommended its use for monitoring quality of life and for planning patient-centered interventions, including its direct integration into electronic health systems. A similar framework could be adapted for our questionnaire, enabling the periodic assessment of the health status of medical professionals and supporting the development of occupational prevention and protection measures based on objective data.
The parallel with recent research in public health, clinical nutrition, and chronic disease prevention is relevant [31-35]: those studies demonstrated that personalized interventions, designed on the basis of detailed initial assessments, yield superior outcomes. Similarly, our questionnaire could support the personalization of strategies for preventing burnout syndrome and other occupational conditions, optimizing preventive interventions according to the identified risk profile.
Limitations
This study has several limitations that should be taken into account when interpreting the results. First, the investigated population is specific, consisting of surgeons actively working in public healthcare institutions in the Republic of Moldova. The total number of surgeons at the national level is 460, which means that the results cannot be directly extrapolated to other professional categories or contexts.
Second, the relatively small sample size (n = 52) did not allow for the performance of either a confirmatory factor analysis (CFA) or an exploratory factor analysis (EFA). The literature recommends, for such analyses, a minimum ratio of 5-10 participants per item, a condition that could not be met at this stage. Consequently, this phase of the study focused exclusively on content validity assessment, item analysis (discrimination, directionality), and internal consistency (Cronbach’s α), with EFA and CFA planned to be conducted on a larger sample in a future study.
Conclusions
The final structure of the questionnaire fully corresponds to the initially defined theoretical dimensions and demonstrates robust psychometric properties, as evidenced by the high values of the content validity indices (I-CVI, S-CVI/Ave, S-CVI/UA, Kappa) and the very good overall internal consistency (Cronbach’s α = 0.808). The domain-level analysis confirmed that each section consistently measures the intended constructs, with α values ranging from 0.715 to 0.864, indicating a balance between item homogeneity and the coverage of the diversity of aspects assessed.
The adjustments made based on expert feedback and observations from the piloting stage, such as the removal of items with low relevance, the rephrasing of unclear questions, and the clarification of technical terms, contributed to improving the clarity and practical applicability of the instrument. These results are consistent with data reported in the international literature for similar instruments, confirming that the applied methodology is robust and yields a tool comparable in psychometric performance to established questionnaires.
The resulting questionnaire is suitable for assessing health status and occupational risk factors among surgeons and can be applied both in research and in periodic institutional evaluations. Extending validation to larger samples and multicentric contexts, as well as adapting it to other medical specialties, will enhance its applicability, international comparability, and utility in informing occupational health policies.
Competing interests
None declared.
Authors’ contributions
All the authors participated in the study design and contributed to drafting the manuscript. The authors critically reviewed the work and approved the final version of the manuscript.
Acknowledgements
The authors express their sincere thanks to the health specialists and teaching staff who contributed essentially to the evaluation, improvement, and adjustment of the questionnaire: Victor Meșina, PhD, Associate Professor, Hygiene Discipline, Nicolae Testemițanu SUMPh; Vladimir Bernic, MD, PhD, Research Associate, National Agency for Public Health; Mariana Cernițanu, PhD, Psychology Associate, Department of Mental Health, Medical Psychology and Psychotherapy, Nicolae Testemițanu SUMPh; Alina Ferdohleb, MD, PhD, Associate Professor, Department of Social Medicine and Management, Nicolae Testemițanu SUMPh; Cătălina Croitoru, MD, PhD, Associate Professor, Hygiene Discipline, Nicolae Testemițanu SUMPh.
Ethics approval.
The study protocol was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Protocol No. 02 of 07.10.2024).
Provenance and peer review
Not commissioned, externally peer-reviewed.
Authors’ ORCID IDs
Ana Vîlcova – https://orcid.org/0009-0004-9739-6378
Alexandru Ferdohleb – https://orcid.org/0000-0003-3290-8139
Larisa Spinei – https://orcid.org/0000-0002-5370-9801
Angela Paraschiv – https://orcid.org/0000-0003-0817-8316
Raisa Deleu – https://orcid.org/0000-0001-8922-2491
Elena Ciobanu – https://orcid.org/0000-0002-8969-922X
References
Hess P, Athanasiadis D, Kissane Lee N, Monfared S, Moyers Cleveland P, Stefanidis P. Preventing surgeon work-related musculoskeletal disorders: a pilot study of the comprehensive operating room ergonomics (CORE) program. Am J Occup Ther. 2024;78(5):7805205090. doi: 10.5014/ajot.2024.050395.
Rață AL, Barac S, Garleanu LL, Onofrei RR. Work-related musculoskeletal complaints in surgeons. Healthcare (Basel). 2021;9(11):1482. doi: 10.3390/healthcare9111482.
Gorce P, Jacquier-Bret J. Work-related musculoskeletal disorders among surgeons: a bibliometric analysis from 1982 to 2024. Explor Musculoskeletal Dis. 2024;2:317-35. doi: 10.37349/emd.2024.00059.
Sánchez-Guillén L, Lozano-Quijada C, Soler-Silva Á, et al. A calculator for musculoskeletal injuries prediction in surgeons: a machine learning approach. Surg Endosc. 2024;38(11):6577-6585. doi: 10.1007/s00464-024-11237-4.
Landford WN, Ngaage LM, Lee E, Rasko Y, Yang R, Slezak S, et al. Occupational exposures in the operating room: are surgeons well-equipped? PLoS One. 2021;16(7):e0253785. doi: 10.1371/journal.pone.0253785.
White AJ, Nowacki AS, Woodrow SI, Steinmetz MP, Benzil DL. Ergonomics, musculoskeletal disorders, and surgeon gender in spine surgery: a survey of practicing spine surgeons. J Neurosurg Spine. 2024;40(4):529-538. doi: 10.3171/2023.11.SPINE23705.
Rai R, El-Zaemey S, Dorji N, Fritschi L. Reliability and validity of an adapted questionnaire assessing occupational exposures to hazardous chemicals among health care workers in Bhutan. Int J Occup Environ Med. 2020;11(3):128-139. doi: 10.34172/ijoem.2020.1878.
Bagheri M, Torabizadeh C, Amiri A, Adelmanesh Y. Development and psychometric evaluation of a questionnaire for assessment of exposure to chemical hazards in operating room nurses. Perioper Care Oper Room Manag. 2023;(23):100334. doi: 10.1016/j.pcorm.2023.100334.
International Labour Organization. Occupational safety and health profile in the Republic of Moldova [Internet]. Chisinau; 2021 [cited 2025 Aug 5]. Available from: https://www.ilo.org/sites/default/files/2025-04/OSH_Profile_2021_Moldov…
Vîlcova A. Psychoemotional health of medical workers during pandemic period. In: MedEspera: 10th International Medical Congress for Students and Young Doctors; 2024 Apr 24-27; Chisinau, Republic of Moldova: Abstract book. Chisinau; 2024. p. 435.
Vîlcova A. Epuizarea profesională: sinteză narativă [Professional burnout: narrative synthesis]. One Health Risk Manag (Chisinau). 2023;75. [cited 2025 Aug 7]. Available from: https://journal.ohrm.bba.md/index.php/journal-ohrm-bba-md/article/view/…;
Vîlcova A, Dumitras C, Ferdohleb A, Ciobanu E. The impact of burnout syndrome on the quality of surgical services. Antropol Res Stud (Bucharest). 2023;(8):102. 5th International conference “Individual, family, society – contemporary challenges”; 2023 Oct 4-5; Bucharest, Romania.
Curteanu M, Vîlcova A, Ciobanu E. Riscurile profesionale ale lucrătorilor din domeniul sănătății [The professional risks of healthcare workers]. One Health Risk Manag (Chisinau). 2023;(Spec ed: Nov.):108-111. doi: 10.38045/ohrm.2023.SE.03.
Memon AG, Naeem Z, Zaman A, Zahid F. Occupational health related concerns among surgeons. Int J Health Sci (Qassim). 2016;10(2):279-291. doi: 10.12816/0048819.
Mache S, Vitzthum K, Klapp BF, Danzer G. Surgeons' work engagement: influencing factors and relations to job and life satisfaction. Surgeon. 2014;12(4):181-190. doi: 10.1016/j.surge.2013.11.015.
Lesser CS, Lucey CR, Egener B, Braddock CH 3rd, Linas SL, Levinson W. A behavioral and systems view of professionalism. JAMA. 2010;304(24):2732-2737. doi: 10.1001/jama.2010.1864.
Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine (Phila Pa 1976). 2000;25(24):3186-3191. doi: 10.1097/00007632-200012150-00014.
Johnson TP. Methods and frameworks for crosscultural measurement. Med Care. 2006;44(11 Suppl 3):S17-S20. doi: 10.1097/01.mlr.0000245424.16482.f1.
Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res Nurs Health. 2007;30(4):459-467. doi: 10.1002/nur.20199.
de Alwis MP, Lo Martire R, Äng BO, et al. Development and validation of a web-based questionnaire for surveying the health and working conditions of high-performance marine craft populations. BMJ Open. 2016;6:e011681. doi: 10.1136/bmjopen-2016-011681.
Polit DF, Beck CT. The content validity index: Are you sure you know what's being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489-497. doi: 10.1002/nur.20147.
George D, Mallery P. SPSS for Windows step by step: A simple guide and reference. 11.0 Update. 4th ed. Boston: Allyn & Bacon; 2003.
DiIorio CK. Measurement in health behavior: methods for research and evaluation. New York: John Wiley & Sons; 2006.
Jafari-Golestan N, Dalvandi A, Hosseini M, Fallahi-Khoshknab M, Ebadi A, Rahgozar M, et al. Designing and validating of a questionnaire measuring perceived self-care ability (PSCA) in chronic stroke patients at home. BMC Neurol. 2024;24(1):125. doi: 10.1186/s12883-024-03612-4.
Anuarul statistic al sistemului de sănătate din Moldova anii 2022- 2023 [Statistical yearbook of the healthcare system in Moldova 2022-2023]. Romanian. [cited 2025 Nov 6]. Available from: https://bit.ly/495yUlp
Rapisarda F, Corbière M, Lesage AD, et al. Development and validation of the mental health professional culture inventory. Epidemiol Psychiatr Sci. 2019;29:e80. doi: 10.1017/S2045796019000787.
Beyera GK, O'Brien J, Campbell S. The development and validation of a measurement instrument to investigate determinants of health care utilisation for low back pain in Ethiopia. PLoS One. 2020;15(1):e0227801. doi: 10.1371/journal.pone.0227801.
Jafari-Golestan N, Dalvandi A, Hosseini M, et al. Designing and validating of a questionnaire measuring perceived self-care ability (PSCA) in chronic stroke patients at home. BMC Neurol. 2024;24(1):125. doi: 10.1186/s12883-024-03612-4.
Al-Qerem W, Abdo S, Jarab A, Hammad A, Eberhardt J, Al-Asmari F, et al. Validation of the Arabic version of the long-term conditions questionnaire (LTCQ): a study of factor and rasch analyses. Healthcare (Basel). 2025;13(13):1485. doi: 10.3390/healthcare13131485.
Dellafiore F, Arrigoni C, Ghizzardi G, Baroni I, Conte G, Turrini F, et al. Development and validation of the pressure ulcer management self‐efficacy scale for nurses. J Clin Nurs. 2019;28(17-18):3177-3188. doi: 10.1111/jocn.14875.
McKenna A, Thurecht RL, Swanepoel L, Blair G, Pelly FE. Development and preliminary validation of the PC-FCQ: the parent and carer food choice questionnaire. Nutrients. 2025;17(10):1735. doi: 10.3390/nu17101735.
Croitoru C, Ciobanu E, Ferdohleb A. Validarea chestionarului: Cunoștințe, Atitudini și Practici privind fenomenul de antibiorezistență la medici [Validation of questionnaire: Knowledge, Attitudes and Practices regarding the antibioresistance phenomenon to doctors]. Arta Medica. 2022;(3):4-15. Romanian. doi: 10.5281/zenodo.7305448.
Croitoru C, Ferdohleb A, Ceban T, Ferdohleb E. OCRA checklist and ergonomic risk assessment in the surgery department. In: Proceedings of the Conference of “Francisc I. Rainer” Anthropology Institute of the Romanian Academy; 2015 May, Bucharest, Romania.
Bologan V, Mazur-Nicorici L, Spinei L, Cebanu S, Visnevschi A, Ciobanu E. Development and validation of a questionnaire for hygienic estimation of the impact of risk factors on morbidity due to osteoporosis. Mold J Health Sci. 2024;4(11):15-21. doi: 10.52645/MJHS.2024.4.03.
Curteanu M, Marinescu V, Ferdohleb A, Bahnarel I, Pînzaru I, Ciobanu E. Testing and validation of the questionnaire for evaluating the chemical composition of bottled water in relation to public health. Mold J Health Sci. 2025;1(12):41-47. doi: 10.52645/MJHS.2025.1.07.