

Introduction
Cutaneous melanoma, with a continuously rising incidence worldwide, represents one of the most aggressive forms of skin cancer. Although it accounts for only about 4% of all cutaneous malignancies, melanoma is responsible for approximately 80% of skin cancer-related deaths, reflecting its high metastatic potential and resistance to treatment [1]. The global burden of melanoma has increased significantly over recent decades, with current estimates suggesting over 331,722 new cases annually worldwide [1]. In the United States, the American Cancer Society projects that in 2025, nearly 105,000 new cases of invasive melanoma and over 107,000 cases of melanoma in situ will be diagnosed, resulting in approximately 8,400 deaths [2]. Among white populations, the overall lifetime risk of developing invasive melanoma is estimated at 1 in 29 for males and 1 in 40 for females. Despite significant advancements in understanding melanoma biology and the development of immunotherapeutic and targeted treatment strategies, a substantial proportion of patients continue to succumb to the disease due to therapeutic resistance and metastatic spread [3]. Hence, identification of histopathologic parameters associated with aggressive behavior remains a crucial component of melanoma research and patient management [4]. Among the histopathologic features that may influence tumor aggressiveness, lymphovascular invasion (LVI) and perineural invasion (PNI) have attracted increasing attention. While the prognostic role of LVI remains controversial, several studies have associated it with tumor-positive sentinel node metastasis and poorer survival, particularly in tumors showing regression [5]. Perineural invasion, although rare, is increasingly recognized as a potential route of local spread and recurrence, especially in desmoplastic melanoma, which displays neurotropic characteristics [6].
Materials and methods
A total of 47 tumor specimens (from 24 women and 23 men with a mean age of 65.6 ± 12.2 years, median age 68, range 31-88 years) with confirmed diagnoses of superficial spreading melanoma were selected from the archival database (2020-2024) of the Oncology Institute, Chisinau, Republic of Moldova, along with corresponding morphology reports. Each case was reviewed by two pathologists for tumor thickness, Clark level, ulceration, mitotic activity, microsatellitosis, lymphocytic infiltration, pigmentation status, and lymph node involvement. The presence of lymphovascular and perineural invasion was assessed using routine hematoxylin and eosin (HE) staining (ST Infinity H&E Staining System, 3801698, Leica), as well as immunohistochemically (Leica autostainer XL ST5010) following the S100 (BSB5918/ clone 4C4.9/ RTU/ 45 minutes room temperature/ BioSB) and CD31 (PA0414/ clone JC70A/ RTU/ 25 minutes room temperature/ Leica) protocols (Envision FLEX Target retrieval solution high pH/ DM828/ 20 minutes/ Agilent Dako; Mouse/Rabbit PolyDetector Plus DAB HRP Brown, BSB 0261, 60 minutes/ BioSB) (Figure 1, 2). Statistical correlations were calculated using Pearson or Spearman coefficients, depending on the variable type, with significance level set at p ≤ 0.05.
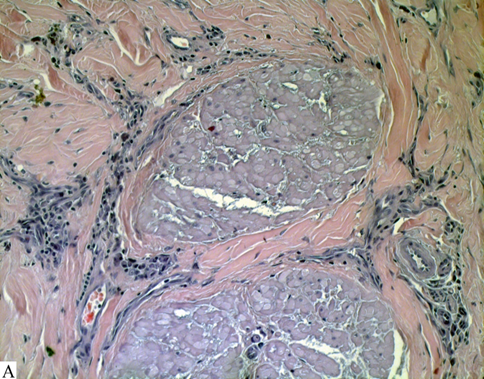 | 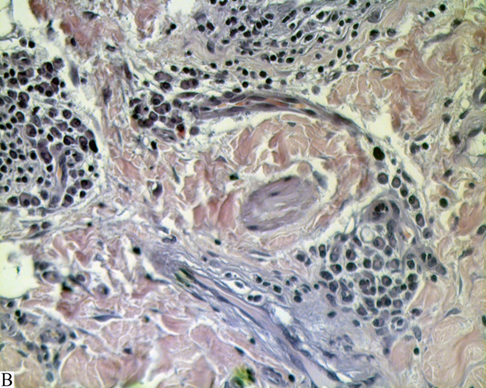 |
Fig. 1 Perineural and perivascular invasion of cutaneous malignant melanoma. Note: (A) Clusters of atypical melanocytic tumor cells infiltrating the perineurium, consistent with perineural invasion (HE, ×200). (B) Tumor cells surrounding and infiltrating the wall of a small dermal vessel, demonstrating perivascular/vascular-associated invasion (HE, ×400) | |
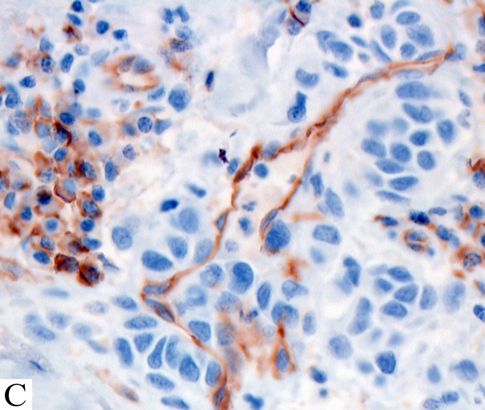 | 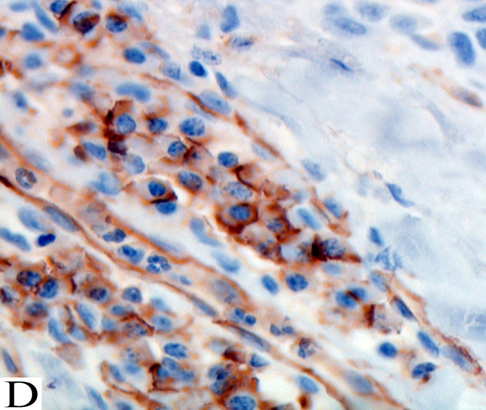 |
Fig. 2 Vascular invasion of cutaneous malignant melanoma. Note: (C–D) Angiotropic spread and intravascular invasion with hyperchromatic melanoma cells. CD31 immunohistochemistry confirms vascular invasion: endothelial cells stain brown (HRP/DAB), while infiltrating melanoma cells distort or penetrate the vascular wall (Mayer’s hematoxylin counterstain, ×400). | |
Results
Lymphovascular invasion (LVI) was significantly correlated with several indicators of tumor aggressiveness (Table 1).
Table 1. Correlation coefficients of lymphovascular and perineural invasion with clinicopathologic variables | ||||
Variable | Lymphovascular invasion | Perineural invasion | ||
r | p | r | p | |
Age | 0.01 | 0.48 | 0.20 | 0.09 |
Gender | 0.22 | 0.07 | –0.14 | 0.17 |
Tumor thickness | 0.54 | 0.001* | –0.03 | 0.41 |
Clark level | 0.46 | 0.001* | 0.11 | 0.22 |
Ulceration | 0.14 | 0.17 | 0.08 | 0.30 |
Mitotic activity | –0.09 | 0.27 | –0.13 | 0.19 |
Lymphocytic invasion | –0.21 | 0.07 | 0.04 | 0.38 |
Microsatellitosis | 0.50 | 0.001* | –0.04 | 0.40 |
Tumor regression | –0.26 | 0.04* | –0.24 | 0.05* |
Tumor stage | 0.33 | 0.01* | 0.12 | 0.20 |
Lymph node involvement | 0.29 | 0.02* | –0.04 | 0.40 |
Pigmentation | –0.26 | 0.04* | –0.24 | 0.05* |
Note: r – correlation coefficient. The asterisk (*) indicates statistically significant results (p < 0.05). | ||||
A significant positive correlation was identified between LVI and tumor thickness (r = 0.54, p < 0.001) as well as Clark level (r = 0.46, p < 0.001). LVI also demonstrated significant associations with microsatellitosis (r = 0.50, p < 0.001), tumor stage (r = 0.33, p = 0.01), and lymph node involvement (r = 0.29, p = 0.02). A moderate, inverse correlation was observed between LVI and pigmented melanomas (r = –0.26, p = 0.04), suggesting that lymphovascular infiltration tends to occur less frequently in melanotic (pigmented) lesions, and is more often associated with amelanotic tumors. No significant correlation was found between LVI invasion and age, gender, or mitotic activity (p > 0.05). Overall, the presence of lymphovascular invasion was associated with deeper, more advanced melanomas and with histopathological parameters reflecting poor prognosis.
Perineural invasion (PNI) was also associated with adverse prognostic features. Its presence correlated positively with lymphovascular invasion (r = 0.28, p = 0.03), indicating a tendency for co-occurrence of vascular and neural infiltration. Weak, non-significant correlations were found between perineural invasion and tumor thickness (r = –0.03, p = 0.41) and Clark level (r = 0.11, p = 0.22). No significant associations were observed between PNI and ulceration, mitotic activity, or lymphocytic infiltration (p > 0.05). A negative correlation with pigmented melanomas (r = –0.24, p = 0.05) approached statistical significance, suggesting that perineural invasion tends to occur less frequently in melanotic lesions and more commonly in amelanotic variants.
Discussion
This study examines the prognostic relevance of lymphovascular and perineural invasion in cutaneous malignant melanoma, emphasizing their association with advanced disease features and markers of aggressive tumor behavior. Our findings show that especially lymphovascular invasion correlate strongly with histopathologic indicators of progression, including increased tumor thickness, higher Clark level, the presence of microsatellitosis, and lymph node involvement.
Taken together, these relationships underscore the importance of lymphovascular and perineural invasion as meaningful markers of invasive potential in cutaneous malignant melanoma. The current findings are consistent with evidence in the literature suggesting that lymphovascular invasion represents a strong predictor of tumor aggressiveness and poor prognosis [5]. Previous studies have demonstrated that lymphovascular invasion correlates with increased tumor thickness, ulceration, and sentinel lymph node positivity, all of which are established prognostic factors in melanoma [5]. The observed correlations in our cohort between lymphovascular invasion and parameters such as Breslow thickness, Clark level, microsatellitosis, and lymph node involvement reinforce its prognostic significance. This aligns with the results reported by Egger et al. (2011), who found lymphovascular invasion to be an independent factor associated with shorter disease-free and overall survival [5].
Interestingly, we observed a negative correlation between lymphovascular invasion and tumor pigmentation, suggesting that amelanotic melanomas may represent a more aggressive biological subtype with enhanced invasive potential. This observation is in accordance with prior research showing that amelanotic or hypopigmented melanomas are often diagnosed at a more advanced stage due to delayed clinical recognition and tend to have worse outcomes [7]. The association between lack of pigmentation and the presence of lymphovascular invasion may therefore reflect a distinct biological phenotype with enhanced invasive potential [7]. Loss of pigmentation in melanoma is often associated with cellular dedifferentiation and the epithelial –mesenchymal transition, processes that increase cell movement and invasiveness [8, 9]. This dedifferentiation is accompanied by reduced expression of melanocytic antigens, such as microphthalmia-associated transcription factor and tyrosinase, and by increased secretion of molecules that promote the formation of new blood vessels, including vascular endothelial growth factor A and vascular endothelial growth factor C [8, 9]. These molecular alterations create a microenvironment that supports invasion into blood vessels and the spread of cancer to distant sites.
Perineural invasion, although less common, showed a positive correlation with lymphovascular invasion, suggesting that both processes may share similar mechanisms of invasiveness. Infiltration of nerve tissue is known to involve neurotropic signaling pathways mediated by nerve growth factor and its receptor tropomyosin receptor kinase A, also known as neurotrophic receptor tyrosine kinase 1, as well as glial cell line-derived neurotrophic factor [10]. These signaling molecules promote the migration of tumor cells along nerve sheaths and enhance their survival.
The observation that perineural invasion occurs more frequently in non-pigmented, or amelanotic, melanoma variants supports the hypothesis that dedifferentiated melanomas acquire neurotropic characteristics, which facilitate local recurrence and spread along nerves [11].
Beyond these morphological findings, recent molecular research provides mechanistic explanations for these invasive behaviors [10]. Tumors that display lymphovascular invasion or perineural invasion often show reduced numbers of tumor-infiltrating lymphocytes and increased expression of programmed death-ligand 1, creating an immunosuppressive environment that allows tumor cells to evade immune detection. The resulting “immune-cold” phenotype promotes the formation of new blood vessels and remodeling of nerve tissue while diminishing the cytotoxic activity of cluster of differentiation 8-positive T cells.
This interaction between immune evasion and stromal invasion has been confirmed by recent immunogenomic studies of melanoma, which demonstrate that overexpression of programmed death-ligand 1 and low tumor-infiltrating lymphocyte counts are associated with increased vascular invasion and poorer survival outcomes [3, 4].
From a pathological standpoint, the identification of lymphovascular and perineural invasion in melanoma specimens should prompt careful staging and follow-up, as both features may indicate a higher risk of regional or distant metastasis. Including these variables in histopathological reports could therefore improve risk stratification and guide treatment decisions, particularly regarding sentinel lymph node biopsy and adjuvant therapy considerations.
Our study may have some limitations. The retrospective design introduces potential selection bias, and the relatively small number of cases may limit the generalizability of our findings. Additionally, the lack of follow-up and survival data precludes the assessment of the prognostic impact of lymphovascular and perineural invasion on patient outcomes. Another limitation is the restriction of our analysis to superficial spreading melanoma, which limits the extrapolation of results to other histological subtypes such as nodular or acral lentiginous melanoma.
Despite these limitations, our study adds to the growing body of evidence emphasizing the prognostic value of lymphovascular and perineural invasion in cutaneous malignant melanoma. The integration of these histopathologic features into routine diagnostic evaluation could enhance prognostic accuracy and ultimately contribute to more individualized management strategies for melanoma patients. Future research incorporating molecular profiling and long-term clinical follow-up is warranted to clarify the biological pathways underlying these invasive patterns and their potential therapeutic implications.
Conclusions
Lymphovascular invasion emerges as a robust histopathologic marker of aggressive biological behavior in superficial spreading melanoma. Its significant associations with tumor thickness, Clark level, microsatellitosis, and lymph node involvement underscore its prognostic importance and support its routine inclusion in pathology reports. The inverse relationship with pigmentation further suggests that amelanotic melanomas may possess greater invasive potential, likely reflecting tumor dedifferentiation and the activation of angiogenic pathways that promote vascular dissemination.
Perineural invasion, although less common, showed a positive correlation with lymphovascular invasion, implying partially overlapping mechanisms of tumor spread involving both vascular and neural structures. This observation aligns with the hypothesis that neurotropic signaling and microenvironmental remodeling contribute to melanoma progression, particularly in amelanotic variants.
Collectively, these findings position lymphovascular and perineural invasion as complementary indicators of tumor aggressiveness in melanoma. Their combined assessment –ideally integrated with molecular parameters such as tumor-infiltrating lymphocyte density and PD-L1 expression – has the potential to enhance prognostic precision and inform more individualized therapeutic strategies.
Competing interests
None declared.
Authors’ contribution
AC: Resources, Investigation, Formal Analysis, Writing – Original Draft Preparation; EF: Conceptualization, Methodology, Writing & Editing; EC: Data Curation, Literature Review; DB: Assistance in the acquisition of histological specimens, Investigation, Formal Analysis; VD: Methodology, Data Curation, Validation; LȘ: Supervision, Validation; VF: Project Administration, Supervision, Final Approval of the Manuscript. All authors approved the final version of the manuscript.
Acknowledgements
The authors express their gratitude to the Department of Histology, Cytology and Embryology and to the Laboratory of Morphology of the Nicolae Testemițanu State University of Medicine and Pharmacy, as well as to Department of Pathology of Oncological Institute from Republic of Moldova. No external funding.
Ethics approval
This study was conducted with the approval of the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy, Chisinau, Republic of Moldova (Minutes No. 4, dated 12.09.2025). All procedures adhered to institutional and national ethical standards for biomedical research and were performed in accordance with the principles outlined in the Declaration of Helsinki.
Provenance and peer review
Not commissioned; externally peer-reviewed.
Authors’ ORCID IDs
Alexandrina Cenusa – https://orcid.org/0009-0007-9135-5569
Ecaterina Foca – https://orcid.org/0000-0001-7629-4875
Ecaterina Carpenco – https://orcid.org/0000-0003-1464-3149
Dumitru Brinza – https://orcid.org/0000-0002-3133-1502
Valeriu David – https://orcid.org/0000-0001-9799-7369
Lilian Șaptefrați – https://orcid.org/0000-0003-2779-718X
Veaceslav Fulga – https://orcid.org/0000-0002-7589-7188
References
Mallardo D, Basile D, Vitale MG. Advances in melanoma and skin cancers. Int J Mol Sci. 2025;26(5):1849. doi: 10.3390/ijms26051849.
Galambus J, Smythe C, Cockerell CJ. Pathology of melanoma: new concepts (2025 Update). Dermatol Clin. 2025;43(3):409-18. doi: 10.1016/j.det.2025.03.008.
Voiculescu VM, Popescu AI, Costache M. Immunohistochemistry for skin cancers: new insights into diagnosis and treatment of melanoma. Cancers (Basel). 2025;17(11):1769.doi: 10.3390/cancers17111769.
de Oliveira GAF, de Oliveira DA, Nisimoto MYSM, Rubinho R, Gomes HC, Marti LC, et al. Advances in tumor-infiltrating lymphocyte (TIL) as a prognostic factor and for treating invasive cutaneous melanoma. Int J Mol Sci. 2024;25(23):12596.doi: 10.3390/ijms252312596.
Egger ME, Gilbert JE, Burton AL, McMasters KM, Callender GG, Quillo AR, et al. Lymphovascular invasion as a prognostic factor in melanoma. Am Surg. 2011;77(8):992-7.
Law WP, Pereira N, Vaska K. Perineural spread of recurrent cutaneous melanoma along cervical nerves into the spinal cord. BJR Case Rep. 2017;3(2):20160122. doi: 10.1259/bjrcr.20160122.
Thomas NE, Kricker A, Waxweiler WT, Dillon PM, Busman KJ, From L, et al.; Genes, Environment, and Melanoma (GEM) Study Group. Comparison of clinicopathologic features and survival of histopathologically amelanotic and pigmented melanomas: a population-based study. JAMA Dermatol. 2014 Dec;150(12):1306-314. doi: 10.1001/jamadermatol.2014.1348.
Wellbrock C, Arozarena I. Microphthalmia-associated transcription factor in melanoma development and MAP-kinase pathway targeted therapy. Pigment Cell Melanoma Res. 2015 Jul;28(4):390-406. doi: 10.1111/pcmr.12370.
Dadras SS, Lin RJ, Razavi G, Kawakami A, Du J, Feige E, et al. A novel role for microphthalmia-associated transcription factor-regulated pigment epithelium-derived factor during melanoma progression. Am J Pathol. 2015 Jan;185(1):252-65. doi: 10.1016/j.ajpath.2014.09.012.
Liu Q, Ma Z, Cao Q, Zhao H, Guo Y, Liu T, et al. Perineural invasion-associated biomarkers for tumor development. Biomed Pharmacother. 2022 Nov;155:113691. doi: 10.1016/j.biopha.2022.113691..
Croker J, Burmeister B, Foote M. Neurotropic melanoma: the management of localized disease. J Skin Cancer. 2012;2012:706452. doi: 10.1155/2012/706452.