

Introduction
Cleft lip and palate are congenital deformities with a multifactorial determinism resulting from the interaction of genetic or environmental factors [1]. The worldwide incidence of cleft lip and palate is 1:700, with the highest in Europe being in Finland at 2.36 cases per 1000 newborns [2].
In the Republic of Moldova, among the most common clefts of the lip and palate are cleft palates [3]. Patients with cleft lip and palate present dento-maxillary anomalies of skeletal and dental form due to deformations of the maxillary bones and imbalance between facial muscle forces [4]. Consequently, the functions of the dento-maxillary system, such as mastication, phonation and facial appearance, may be negatively affected [5]. The craniofacial orthodontist, who is part of the multidisciplinary team, plays an important role in the assessment and treatment of the development of dental occlusion and facial appearance during the main stages of growth [6, 7].
During the development of dental occlusion, the orthodontic treatment of malocclusion goes through 2 phases: the interceptive orthodontic treatment phase, which represents the preparation of the dento-maxillary apparatus for bone grafting surgery, and the complete orthodontic treatment phase with or without orthognathic surgery and possible orthopedic and dental restorative treatments [8].
Reconstruction of the maxillary bone defect in the preadolescent period has become a critical period in the complete treatment of patients with cleft lip and palate after the period of primary reconstruction of the lip, nose, and hard and soft palate. In patients with unilateral and bilateral cleft lip and palate involving alveolar defects, bone grafting surgery has several benefits. It provides bone support for tooth eruption, prevents impaction of the upper canines, and facilitates safe orthodontic treatment [9].
Compression of the maxilla is frequently encountered in patients with cleft lip and palate, leading to malocclusion with a prevalence of anterior reverse occlusion of 62% [10].
Bone grafting surgery is performed after orthodontic treatment by expanding the maxilla. Expansion of the maxillary dental arch during the mixed dentition period is very important because it normalizes the morphology and induces correct and symmetrical eruption of the canine on the dental arch [11, 12].
The aim of the study is to evaluate the size of the upper jaw in children with an average age of 9.35 years with unilateral cleft lip and palate in the transverse and sagittal plane over a period of 9 months and the preparation for bone grafting surgery.
Material and methods
The study included 20 patients with cleft lip and palate, including 8 girls and 12 boys aged 6-12 years The mean age of children was 9.35 years which include unilateral cleft lip and palate, bilateral cleft lip and palate and cleft palate only. All patients underwent primary lip surgery at the age of 3 months and primary hard and soft palate surgery in one stage at the age of 12 months. No formal a priori sample size calculation was performed. The sample consisted of all consecutive children aged 6–12 years with cleft lip and/or palate who met the inclusion criteria and received early interceptive orthodontic treatment at our center during the mixed dentition stage, prior to secondary alveolar bone grafting. All patients were treated and assessed under a uniform clinical workflow at the same institution, to reduce procedural variability. Measurement reproducibility (intra- and inter-examiner reliability) was not formally tested and is acknowledged as a limitation.
For the evaluation of this group of 20 patients with malocclusion in children with unilateral cleft lip and palate during the mixed dentition period, the following research methods were collected: clinical examination, photometric examination, biometric analysis of study models before treatment (T1) and after sagittal/transverse maxillary expansion (T2). The average treatment interval was 12.2 months.
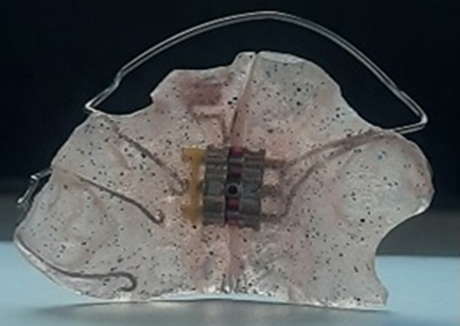
The slow maxillary expansion with plate appliances was performed in the transverse and sagittal planes. The removable orthodontic appliance was fabricated in the dental laboratory from self-curing acrylate material containing a classic monomaxillary orthodontic transverse screw to produce symmetrical widening of the maxillary dental arch or sagittal screw to produce elongation of the maxillary dental arch. The expansion was achieved by activating the screw ¼ turn per week, which caused the two half-frames to move apart by 0.2-0.25 mm per week (Fig. 1). Of all the patients with unilateral cleft lip and palate, 11 patients underwent interceptive orthodontic treatment with a slow expansion orthodontic removable plate appliance in the transverse plane and 9 patients underwent interceptive orthodontic treatment with a slow expansion orthodontic removable plate appliance in the sagittal plane depending on the severity of crossbite in the anterior or posterior region.
 A |  B |
Fig. 1 Removable orthodontic appliances on the upper jaw Note: A - in the transverse plane; B - in the sagittal plane | |
The plaster models were obtained immediately before and after 12.2 months of slow maxillary expansion orthodontic treatment.
All study plaster models of the upper arch were scanned using the Virtuo Vivo intraoral scanner (Fig. 2) and converted to STL format by an experienced laboratory technician to minimize procedural variability [13]. The measurements were made for both transverse and sagittal dimensions according to Pont and Korhaus indexes [14]. Maxillary expansion was evaluated using the Dolphin Image Software before and after 12.2 months of treatment.
 |
Fig. 2 Virtuo Vivo Straumann intraoral scanner Software. |
The development of the upper dental arch before and after 12.2 months of interceptive orthodontic treatment was determined using the biometric method of study model analysis. The measurements included the inter-permanent-molar width. The distances with a tooth as a landmark were measured from the central fossa of the right and left upper first permanent molars before and after 12.2 months of orthodontic treatment (Fig. 3 A and B).
 A | 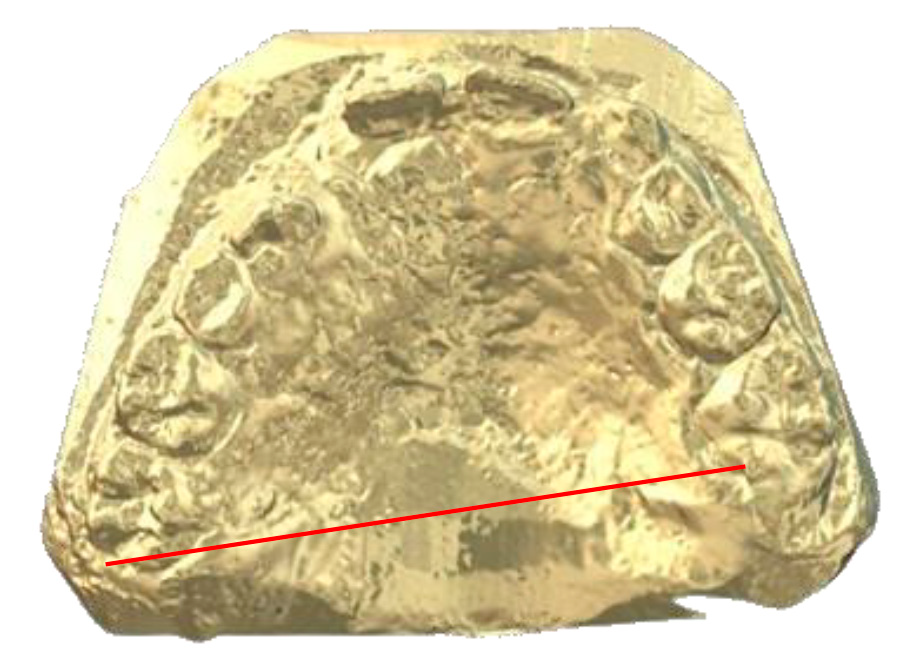 B |
Fig. 3. Maxillary width of the dental arch measured on digital dental cast Note: A- before interceptive orthodontic treatment (T1); B- after interceptive orthodontic treatment (T2) for 12.2 months. | |
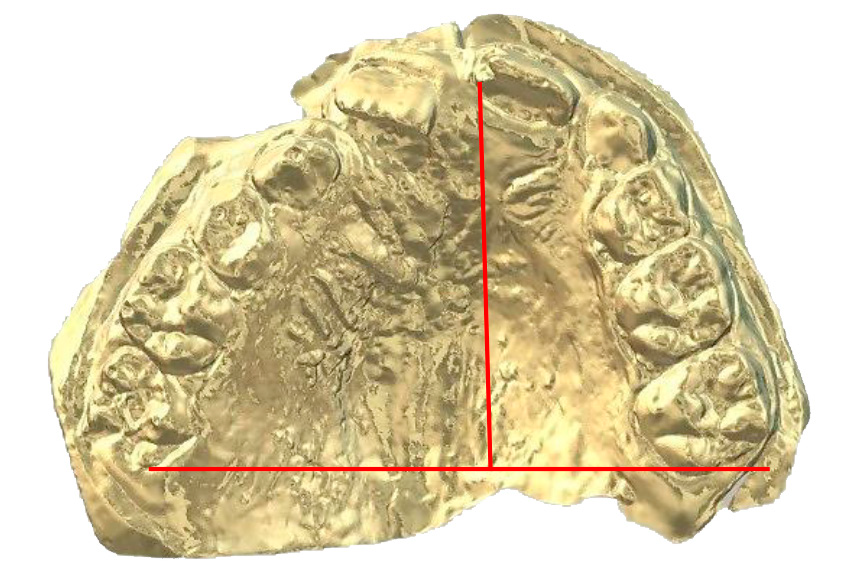
For sagittal dimensions, we analyzed on the cast the length of the upper dental arch which was measured from the point between the upper incisors perpendicular to the junction of the distal surfaces of the first permanent molars before and after 12.2 months of orthodontic treatment (Fig. 4A and B).
 A |  B |
Fig. 4 Maxillary length of the dental arch measured on digital dental cast Note: A - before interceptive orthodontic treatment (T1); B - after interceptive orthodontic treatment (T2) for 12.2 months. | |
The data were analyzed using SPSS ver.18 for Windows platform (SPSS Inc., Chicago, Illinois, USA) and MS. Excel (Microsoft Office, Windows 2007, USA).
Descriptive statistics for the quantitative variables were obtained using mean and standard, deviation values for maxillary width and length before and after 12.2 months of orthodontic interceptive treatment. To evaluate differences in width and length of the dental arch before and after orthodontic treatment of 12.2 months paired t-tests with interaction effects were used to compare the maxillary arch dimensions before and after orthodontic treatment of 12.2 months and to determine significant differences (SPSS ver.18) in children with cleft lip and palate. For the analysis, p < 0.05 was considered statistically significant.
Results
The scanned dental casts for this study were taken at a mean age of 9.35 years. Boys slightly outnumbered girls in the study population (n = 12 vs n = 8). The most common cleft in this study was unilateral cleft lip and palate (n = 16), which clinically presented with anterior and posterior crossbite (Fig. 5).
 A |  B |  C |
Fig. 5 Anterior and posterior reverse occlusion in patient AC, 10 y. o. with unilateral cleft lip and palate. A -frontal view; B- lateral right view; C- lateral left view | ||
Frequency of crossbite in children with cleft lip and palate
During the clinical evaluation of patients with cleft lip and palate, we analyzed the frequency of crossbite at the beginning of the treatment, in which anterior and posterior crossbite was determined in 11 patients (55%) and anterior crossbite - in 3 patients (15%), unilateral posterior crossbite - in 3 patients (15%) and bilateral - in 3 patients (15%) (Fig. 6).
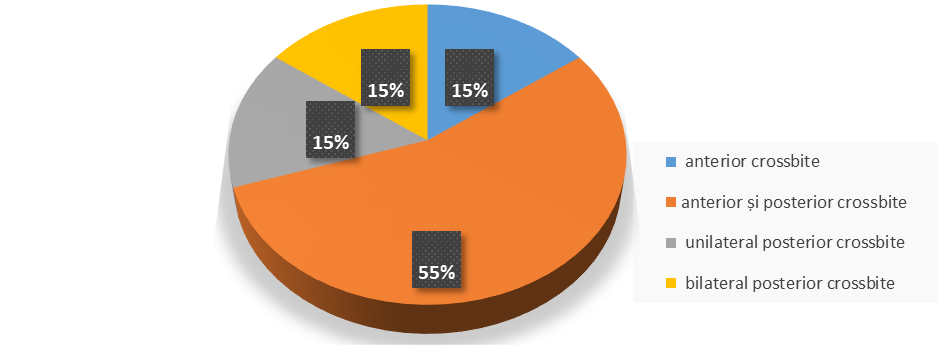 |
Fig. 6 Clinical forms of crossbite in patients with cleft lip and palate |
In 11 children with cleft lip and palate who underwent interceptive orthodontic treatment with a removable appliance in the transverse plane (Fig. 7), the following values were observed between T1 (pre-treatment) and T2 (12.2 months post-treatment) – the mean dimension in transversal plane has statistically significantly increased from 43.40 ± 2.94 to 45.77 ± 3.55 (p = 0.002), but in the sagittal plane, the post-treatment mean values (25.27 ± 2.64) did not change significantly (p = 0.711) from the pre-treatment mean values (25.13 ± 2.59) ( Table 1).
 A | 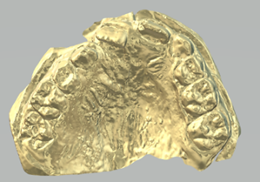 B |  C | 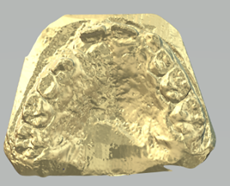 D |
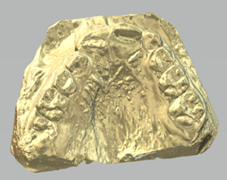
Fig. 7. Evolution of transverse expansion of maxillary dental arch in children with cleft lip and palate Note: A – initial dental cast; B – 3 months of treatment; C- 6 months of treatment; D -12 months of treatment. | |||
Table 1. Biometric parameters of the maxillary dental arch in transverse and sagittal plane pre- and post-treatment for 12.2 months during transverse expansion | |||||||
Comparisons (pre- vs. post-treatment) | t | p | Mean difference | SE difference | 95% CI | Effect Size (Cohen's d) | |
Lower | Upper | ||||||
Dimension in transverse plane | -4.280 | 0.002 | -2.364 | 0.552 | -3.594 | -1.133 | -1.291 |
Dimension in sagittal plane | -0.382 | 0.711 | -0.136 | 0.357 | -0.933 | 0.660 | -0.115 |
Note: t- t-student test; p - probability; SE – Standard Error; CI -confidence interval; Cohen effect size coefficient method | |||||||
In sagittal plane (Fig. 8) the results showed that in 9 children with cleft lip and palate who underwent interceptive orthodontic treatment with a removable appliance, the following values were observed between T1 (pre-treatment) and T2 (12.2 months post-treatment) – the mean dimension in the transverse plane slightly increased from 45.83 ± 2.92 to 45.88 ± 2.96 (p = 0.347), but in the sagittal plane, the post-treatment mean value (26.44 ± 4.71) modified significantly (p = 0.05) from the pre-treatment mean values (24.83 ± 3.89) (Table 2).
 A |  B |  C | 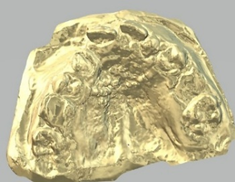 D |
Fig. 8 Evolution of sagittal expansion of maxillary dental arch in children with cleft lip and palate Note: A – initial dental cast; B – 3 months of treatment; C- 6 months of treatment; D -12 months of treatment. | |||
Table 2. Biometric parameters of the maxillary dental arch in transverse and sagittal plane pre- and post-treatment during sagittal expansion in average 12.2 months | |||||||
Comparisons (pre- vs. post-treatment) | t | p | Mean difference | SE difference | 95% Confidence Interval | Effect Size (Cohen's d) | |
Lower | Upper | ||||||
Dimension in transverse plane | -1.00 | 0.347 | -0.0556 | 0.0556 | -0.184 | 0.0726 | -0.333 |
Dimension in sagittal plane | -3.88 | 0.05 | -1.6111 | 0.4148 | -2.568 | -0.6546 | -1.295 |
Note: t -t-student test; p -probability; SE – Standard Error; CI -confidence interval; Cohen effect size coefficient method | |||||||
Discussion
The results of this study showed that interceptive maxillary expansion orthodontic treatment for 12.2 months in children with cleft lip and palate, using a removable orthodontic appliance, resulted in a greater increase in the sagittal plane than in the transverse plane. The growth of the maxilla in children with cleft lip and palate is important for the development of the dento-maxillary system and the eruption of permanent teeth. Surgical intervention at a very young age slows the growth and development of the maxilla, which is demonstrated by several studies [15-17].
Early orthodontic rehabilitation of children with cleft lip and palate leads to improved aesthetic, morphological and social appearance. The specific features of interceptive orthodontic treatment in children with cleft lip and palate aim to prepare the dental arches for secondary bone grafting before the eruption of the upper canines.
In different countries of the world there are different protocols for surgical rehabilitation of cleft lip and palate. A study that evaluated the growth of the maxilla following surgical treatment of the hard and soft palate in two stages and orthodontic treatment during the period of mixed, early and late permanent dentition showed that the width, length and surface of the hard palate increase satisfactorily during the period of mixed dentition. It was also found that the expansion of the maxilla occurs more in patients who underwent primary surgical rehabilitation in two stages compared to primary surgical rehabilitation in one stage [18].
Interceptive orthodontic treatment with slow or rapid maxillary expansion has been evaluated by several authors in both patients with and without cleft lip and palate [19, 20].
The results of one study showed that the duration of slow expansion treatment compared to rapid expansion treatment depends on the activation protocol of the dental appliance. Thus, both slow and rapid expansion resulted in significant increases in maxillary width and dental arch perimeter, but dental arch length and palatal depth decreased insignificantly after slow expansion and significantly after rapid maxillary expansion [21, 22].
Another study demonstrated the therapeutic effects with plate appliance in children without cleft lip and palate which showed that the increases in width, height and surface differed only slightly between the patient groups and did not relapse: the morphological changes were comparable in patients of different ages, with the greatest effects being observed in the posterior molar region [23].
The present study showed that the increase in length of the maxilla was greater than the width in children with cleft lip and palate. This may be due to early surgical intervention on the palate in children with cleft lip and palate and the plate appliances cannot generate considerable forces that can lead to stimulation of the midpalatal suture.
This study has several limitations. It is a single-center observational case series of 20 children with cleft lip and/or palate, aged 6–12 years, followed for about one year. No formal a priori power or sample size calculation was performed; instead, we included all consecutive eligible patients treated at our clinic during the mixed dentition stage, before planned secondary alveolar bone grafting. Cleft lip and/or palate occurs in roughly 1 in 600–800 live births worldwide (around 0.7–1.3 per 1,000 births in European countries) and shows substantial variation in presentation (unilateral, bilateral, isolated palate), requiring long-term multidisciplinary care. Because management strategies differ not only between centers but also between surgeons, creating a larger, homogeneous, prospectively followed cohort within a single institution is realistically difficult. The present analysis should therefore be interpreted as exploratory and descriptive rather than confirmatory.
A second limitation is the lack of a parallel control group (for example, unaffected peers or cleft patients managed with a different or delayed protocol). As a result, the post-treatment increases in maxillary arch dimensions cannot be attributed with certainty to the expansion protocol alone. Part of the change may reflect normal craniofacial growth during the mixed dentition period, when the maxilla continues to widen and lengthen. Maxillary and midfacial growth in cleft patients is also influenced by how and when the palate was surgically closed; early one-stage palatal repair has been associated with greater midfacial restriction, whereas staged or later closure tends to preserve maxillary growth more effectively. Because these surgical choices vary widely, they represent an additional confounder.
Third, all patients were treated in one institution using the same interceptive orthodontic workflow, and all maxillary measurements were obtained using the same digital workflow. This standardization helps reduce internal procedural variability, but we did not formally test intra- or inter-examiner reproducibility, so measurement bias cannot be excluded. External validity is also limited. Different cleft teams prepare the maxillary arch before secondary alveolar bone grafting in different ways: some use slow expansion, others use rapid maxillary expansion, and some perform preliminary anterior alignment before grafting. The timing of expansion relative to grafting also differs. These choices can influence arch form, segment position in the cleft area, and even graft performance, so our findings may not translate directly to centers using other biomechanics, activation schedules, or timelines.
Despite these limitations, the findings are clinically relevant in a coordinated cleft care pathway. Interceptive orthodontic expansion during the mixed dentition is commonly used as preparation for secondary alveolar bone grafting: it helps open and derotate collapsed maxillary segments, improves transverse and sagittal arch form, creates bony support for eruption and alignment of teeth adjacent to the cleft (especially the canine and lateral incisor), and facilitates surgical closure of the alveolar defect. In most cleft protocols, the alveolar bone graft is placed in the mixed dentition, usually shortly before eruption of the permanent teeth bordering the cleft and often within a few months after expansion, with the aim of stabilizing the maxillary segment and supporting future occlusion, facial balance, nasal base support, and speech. Early orthodontic–surgical coordination is therefore regarded as part of functional rehabilitation, not just an aesthetic procedure. Prospective controlled studies with larger samples and standardized follow-up are still needed to determine whether the dimensional changes observed here persist and translate into long-term functional and aesthetic benefit after grafting and comprehensive orthodontic treatment.
Conclusions
Slow maxillary expansion treatment during the mixed dentition period in children with cleft lip and palate was found to be more effective in the sagittal plane than in the transverse plane. Overall, the treatment-related changes were more pronounced in length than in width.
The practical application of orthodontic treatment techniques in patients with cleft lip and palate demonstrated a favorable therapeutic evolution and an advantageous recovery of maxillofacial structures for subsequent stages of treatment.
Competing interests
None declared.
Authors’ contributions
SR conceived the study and help drafting the manuscript, SM helped in drafting the manuscript, GB participated in the study design and performed the statistical analysis, CP performed the study design and performed digital model analysis. All authors have read and approved the final version of the manuscript.
Ethics approval
The study was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes No. 42, dated 14.12.2016).
Patient consent
Obtained.
Acknowledgements and funding
Carried out within the research and innovation project „Stimulating excellence in scientific research 2025-2026” entitled „Prediction of developmental disorders and reduction of the degree of disability through early morpho-functional interventions in children with congenital craniofacial malformations (MCCF)”, no. 25.80012.8007.0858, project leader Gudumac Eva, approved by the Decision of the Council of the Contracting Authority no. 04 of 22.07.2025 and the Order of the Contracting Authority no. 19 of 22.07.2025, funded by the National Agency for Research and Development
Provenance and peer review
Not commissioned, externally peer reviewed.
Authors’ ORCID IDs
Silvia Railean – https://orcid.org/0000-0002-8919-3317
Cristina Poștaru –https://orcid.org/0000-0002-7101-6443
Svetlana Melnic – https://orcid.org/0009-0000-9507-582X
Gheorghe Bordeniuc – https://orcid.org/0000-0002-4013-9918
References
Dixon MJ, Marazita ML, Beaty TH, Murray JC. Cleft lip and palate: understanding genetic and environmental influences. Nat Rev Genet. 2011;12(3):167-78. doi: 10.1038/nrg2933.
Lithovius RH, Ylikontiola LP, Harila V, Sándor GK. A descriptive epidemiology study of cleft lip and palate in Northern Finland. Acta Odontol Scand. 2014;72(5):372-375.doi: 10.3109/00016357.2013.840737.
Railean S. Anomalii congenitale cranio-maxilo-faciale la copii – abordare multidisciplinară [Congenital cranio-maxillofacial anomalies in children – multidisciplinary approach]. Chișinău: Medicina; 2020. 268 p. Romanian.
Szyszka-sommerfeld L, Wozniak K, Matthews-Brzozowska T, Kawala B, Mikulewicz M, Machoy M. The electrical activity of the masticatory muscles in children with cleft lip and palate. Int J Paediatr Dent. 2018;28(2):257-265. doi: 10.1111/ipd.12349.
Alpagan Ozdemir S, Esenlik E. Three-dimensional soft-tissue evaluation in patients with cleft lip and palate. Med Sci Monit. 2018;24:8608-8620 doi: 10.12659/MSM.912305.
Dogan E, Dogan EI, Dogan S. Interdisciplinary treatment approaches for cleft lip and palate patients to obtain esthetic and functional results. J Dent Oral Hyg. 2019;11(1):1-5.doi: 10.5897/JDOH2019.0234.
Perillo L, Vitale M, d’Apuzzo F, Isola G, Nucera R, Matarese G. Interdisciplinary approach for a patient with unilateral cleft lip and palate. Am J Orthod Dentofacial Orthop. 2018;153(6):883-894. doi: 10.1016/j.ajodo.2016.12.035.
Berkowitz S, editor. Cleft lip and palate: diagnosis and management. 2nd ed. Berlin: Springer; 2006. 799 p.
Antunes CL, Aranha AM, Bandeca MC, de Musis CR, Borges ÁH, Vieira EM. Eruption of impacted teeth after alveolar bone graft in cleft lip and palate region. J Contemp Dent Pract. 2018:19(8):933-936.
Heliövaara A, Leikola J, Rautio J. Anterior crossbite, dental arch dimensions, and later need for orthognathic surgery in 6-year-old children with unilateral cleft lip and palate. Cleft Palate Craniofac J. 2014;51(5)579-584. doi: 10.1597/12-198.
Watson ACH, Sell DA, Grunwell P. Management of cleft lip and palate. London: Whurr; 2001. 418 p.
Corcoran M, Karki S, Ylikontiola L, Lithovius R, Sándor GK, Harila V. Maxillary arch dimensions in 6-year-old cleft children in Northern Finland: a cross-sectional study. Int J Environ Res Public Health. 2021;18(14):7432. https://doi.org/10.3390/ijerph18147432.
Haque S, Khamis MF, Alam MK, Wan Ahmad WMA. The assessment of 3D digital models using GOSLON Yardstick index: exploring confounding factors responsible for unfavourable treatment outcome in multi-population children with UCLP. Front Pediatr. 2021;9:646830. doi: 10.3389/fped.2021.646830..
Dorobăț V, Stanciu D. Ortodonție și ortopedie dento-facială. Bucharest: Editura medicală; 2003. 493 p. Romanian.
Rando GM, Ambrosio ECP, Jorge PK, Prado DZA, Falzoni MMM, Carrara CFC, Soares S, Machado MA, Oliveira TM. Anthropometric analysis of the dental arches of five-year-old children with cleft lip and palate. J Craniofac Surg. 2018;29(6):1657-1660. doi: 10.1097/SCS.0000000000004806.
Jorge PK, Gnoinski W, Vaz Laskos K, Felício Carvalho Carrara C, Gamba Garib D, Okada Ozawa T, et al. Comparisonof two treatment protocol s in children with unilateral complete cleft lip and palate: tridimensional evaluation of the maxillary dental arch. J Craniomaxillofac Surg 2016;44(9):1117-1122. doi: 10.1016/j.jcms.2016.06.032.
Reiser E, Skoog V, Andlin-Sobocki A. Early dimensional changes in maxillary cleft size and arch dimensions of children with cleft lip and palate and cleft palate. Cleft Palate Craniofac J. 2013;50(4):481-490. doi: 10.1597/11-003.
Eriguchi M, Watanabe A, Suga K, Nakano Y, Sakamoto T, Sueishi K, Uchiyama T. Growth of palate in unilateral cleft lip and palate patients undergoing two-stage palatoplasty and orthodontic treatment. Bull Tokyo Dent Coll. 2018;59(3):183-191. doi: 10.2209/tdcpublication.2017-0014.
Façanha AJO, Lara TS, Garib DG, da Silva Filho OG. Transverse effect of Haas and Hyrax appliances on the upper dental arch in patients with unilateral complete cleft lip and palate: a comparative study. Dental Press J Orthod. 2014;19(2):39-45. doi: 10.1590/2176-9451.19.2.039-045.oar.
Bratu DC, Bratu EA, Popa G, Luca M, Bălan R, Ogodescu A. Skeletal and dentoalveolar changes in the maxillary bone morphology using two-arm maxillary expander. Romanian J Morphol Embryol. 2012;53(1):35-40.
de Medeiros Alves AC, Garib DG, Janson G, de Almeida AM, Calil LR. Analysis of the dentoalveolar effects of slow and rapid maxillary expansion in complete bilateral cleft lip and palate patients: a randomized clinical trial. Clin Oral Investig. 2016;20(7):1837-1847.doi: 10.1007/s00784-015-1675-1.
Garib D, Lauris RC, Calil LR, Alves AC, Janson G, De Almeida AM, Cevidanes LH, Lauris JR. Dentoskeletal outcomes of a rapid maxillary expander with differential opening in patients with bilateral cleft lip and palate: a prospective clinical trial. Am J Orthod Dentofacial Orthop. 2016 Oct;150(4):564-574. doi: 10.1016/j.ajodo.2016.05.006.
Kinzinger GSM, Hourfar J, Kim HJ, Lisson JA. Morphological changes in the palate after transverse expansion with removable orthodontic plate appliances: Short-term effects and follow-up stability. J Orofac Orthop. 2025 Jun 11. English. doi: 10.1007/s00056-025-00592-z. Epub ahead of print. PMID: 40498108.