
Introduction
Tuberculosis (TB) remains one of the leading causes of morbidity and mortality among individuals living with HIV, alongside other opportunistic infections. Co-infection with the human immunodeficiency virus (HIV) substantially increases the risk of developing active TB, with HIV-positive individuals being approximately 15 to 22 times more likely to develop the disease compared to HIV-negative persons. Despite global advances in prevention and care, TB continues to represent the primary cause of death among HIV-infected patients, accounting for an estimated 167,000 deaths in 2023. In low-resource settings, TB often constitutes the initial clinical indicator of underlying HIV infection, further complicating the diagnostic and therapeutic approach. In the World Health Organization (WHO) European Region, approximately 10.8% of TB patients are co-infected with HIV, with the highest burden observed in Eastern Europe [1, 2].
National data reflect similar patterns. In the Republic of Moldova, the rate of TB/HIV co-infection has doubled over the past decade, increasing from 5% in 2011 to over 11.1% of all new and relapsed TB patients by 2022 [3]. This trend underscores an escalating epidemiological challenge and highlights the urgent need for integrated prevention and control strategies. Marked regional disparities are also evident in TB-related mortality. According to WHO data, the estimated TB mortality rate among HIV-infected individuals in the European region is 0.70 per 100,000 population. However, in Eastern Europe, one-year mortality following TB/HIV diagnosis reaches approximately 29%, whereas in Western Europe it remains below 4%, reflecting significant inequalities in access to timely diagnosis, effective anti-TB treatment, and antiretroviral therapy [1, 4]. These findings are consistent with those of a recent meta-analysis on HIV-associated mortality, which reported mortality rates ranging from 5% to 15% across most studies. Furthermore, HIV-infected TB patients exhibit nearly twice the risk of death compared to HIV-negative TB patients (29.1% vs. 15.2%), suggesting a synergistic effect between the two diseases [5]. This highly vulnerable population warrants prioritized clinical attention, with emphasis on early case detection, prompt initiation of combined antiretroviral and anti-tuberculosis therapy, and close follow-up to improve survival outcomes.
The clinical expression of tuberculosis in patients co-infected with HIV diverges considerably from the classical presentation, often manifesting with atypical features that complicate early recognition and diagnosis. This divergence is closely linked to the degree of HIV-associated immunosuppression. In the initial phases of HIV infection, TB may still exhibit typical pulmonary manifestations – such as chronic cough, hemoptysis, cavitary lung lesions on imaging, and systemic signs like persistent fever, weight loss, and night sweats – closely resembling the disease course observed in HIV-negative individuals [6]. However, as immune function declines, the disease presentation becomes progressively atypical, with an increased propensity for extrapulmonary or disseminated forms that lack hallmark radiological signs [7].
In co-infected patients, chest radiographs may still reveal features of pulmonary TB, whereas abdominal ultrasonography often provides valuable clues for detecting extrapulmonary or disseminated involvement. These imaging tools are considered reliable and widely available for clinical use, particularly in low-resource settings [8].
The burden of extrapulmonary TB is disproportionately high among HIV-positive individuals. Multiple studies report that the risk of extrapulmonary tuberculosis may be up to 32-fold higher greater in HIV-infected patients compared to those without HIV [9]. As the level of immunosuppression worsens, the incidence of classic cavitary lesions decreases, while extrapulmonary involvement – including lymphatic, pleural, neurological, pericardial, skeletal, and abdominal localizations – becomes increasingly prevalent [10]. Disseminated TB, frequently involving multiple organ systems, is also more common in advanced stages and is often diagnosed in the absence of bacteriological confirmation [11, 12]. These atypical and smear-negative forms of TB pose significant diagnostic and therapeutic challenges and are associated with poorer outcomes. A meta-analysis confirmed that extrapulmonary TB confers a more than twofold increase in mortality risk compared to pulmonary TB, due to both extensive mycobacterial spread and the more aggressive disease progression associated with HIV co-infection [5].
Given the elevated clinical risk, individuals with TB/HIV co-infection have long been recognized as a "double priority" group for intervention. When these patients also belong to other vulnerable groups (e.g., people who inject drugs, incarcerated individuals), they are considered a "triple priority" in public health efforts [13]. Beyond TB, these patients often contend with a broad spectrum of comorbidities, including cardiovascular and pulmonary conditions, chronic kidney disease, diabetes mellitus, arterial hypertension, dyslipidemia, obesity, and hepatitis C. Opportunistic infections further complicate the clinical picture, with high prevalence of conditions such as cryptococcal meningitis, HPV-related malignancies, and diseases associated with Kaposi sarcoma herpesvirus (KSHV). Recent cohort data show that over half of TB/HIV co-infected individuals (54.2%) develop opportunistic infections, and among these, mortality reached 61.9%, underscoring the gravity of co-infection and the need for timely, integrated clinical management [14, 15].
Objective of this study was to investigate the clinical manifestations in newly diagnosed patients with pulmonary tuberculosis and human immunodeficiency virus (HIV) co-infection.
Material and methods
A retrospective, cross-sectional comparative study was conducted, including clinical data from 320 patients with newly diagnosed pulmonary tuberculosis (TB) in the Republic of Moldova during the year 2021. Inclusion criteria were: age ≥18 years; newly diagnosed pulmonary TB (classified as “new case” according to WHO definitions); confirmed HIV infection for Group I and documented HIV-negative status for Group II; provision of institutional informed consent. Exclusion criteria included: age <18 years or any TB classification other than “new case”.
Group I (study group) comprised all 160 eligible patients with confirmed TB/HIV co-infection, representing almost the entire national cohort of new TB/HIV cases registered that year, including patients from the Transnistrian region. Group II (control group) was selected from the national cohort of new pulmonary TB cases diagnosed in 2021 who tested negative for HIV. From this primary cohort, 160 patients were matched in a 1:1 ratio with Group I based on sex, age (±3 years), place of residence (urban/rural), and Mycobacterium tuberculosis drug resistance profile. The latter criterion included four categories: drug-sensitive (susceptible to all first-line drugs), mono-resistant (resistant to a single first-line drug), poly-resistant (resistant to more than one first-line drug, but not to both isoniazid and rifampicin), and multidrug-resistant (MDR-TB, resistant to at least both isoniazid and rifampicin).
Clinical and paraclinical data (including symptoms, physical examination findings, hematological parameters, ESR, and TB-related complications) were obtained directly from inpatient medical histories in the hospitals where they were admitted and from their outpatient medical records (ambulatory cards). Additional epidemiological and laboratory information was retrieved from the National Tuberculosis Monitoring and Evaluation Information System (SIME-TB). All necessary official documents, authorizations, and institutional agreements were obtained to ensure lawful access to medical data from all participating healthcare facilities, including institutions located in the Transnistrian region.
Matching was performed using the IBM SPSS Statistics 28.0 Case-Control Matching procedure. The database was compiled in Microsoft Excel 2010 and exported to SPSS for analysis. Statistical methods included descriptive statistics (frequencies, percentages, means, medians, 95% confidence intervals), Chi-square test or Fisher’s exact test for categorical variables, Mann–Whitney U test for non-normally distributed continuous variables, and calculation of odds ratios (OR) with 95% confidence intervals. A p-value <0.05 was considered statistically significant.
The required sample size was calculated using EpiInfo 7.2.2.6 (StatCalc – Sample Size and Power) with a 95% confidence level, based on an estimated TB-HIV association of up to 25%, a design effect of 4, and a 10% non-response adjustment. The adjusted sample size was 160 participants per group, based on defined inclusion and exclusion criteria.
Definitions were applied according to the National Clinical Protocol [3]. General condition was classified as satisfactory, moderate, severe, or extremely severe. Disease onset was defined as acute (<2 weeks), subacute (2-8 weeks), insidious (>8 weeks), or asymptomatic. Clinical ‘masks’ of tuberculosis referred to atypical presentations initially resembling pneumonia, COPD, lung cancer, or COVID-19. Radiological extent was defined as limited (single lobe, no extensive cavitation) or extensive (≥2 lobes, bilateral or cavitary disease).
The research protocol, patient information sheet, and consent form were approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (minutes No. 66 from 29.09.2023).
Results
A total of 320 patients were enrolled in the study. In both groups, men predominated over women, with a ratio of 121 (75.6% ,95% CI: 68.4-81.6) to 39 (24.4%, 95% CI: 18.4-31.6) women. Most participants were aged between 25 and 54 years. In Group I (TB/HIV), the mean age was 38.9 years, with a median of 38 years (IQR: 32-44), while in Group II (TB-only) the mean age was 38.7 years, with a median of 38 years (IQR: 32-45).
In the TB/HIV group, the median CD4 count at TB diagnosis was 134 cells/mm³ (interquartile range, IQR: 36-337), with 57.8% of patients having values below 200 cells/mm³. The median HIV RNA level was 5.40×10⁵ copies/mL (IQR: 9.69×10⁴ – 1.56×10⁶), and 7.1% had undetectable viral load. During TB treatment, antiretroviral therapy was administered regularly in 53.3% of patients, irregularly in 28.9%, and not at all in 17.8%. Passive case finding based on symptomatology was the primary detection method in both groups In group I, it accounted for 108 cases (67.5% (95% CI: 59.9-74.3)), compared to 118 (73.7%) cases in Group II (95% CI: 66.4-79.9). Consequently, active detection through clinical or radiological screening accounted for 32.5% and 26.3%, respectively.
The predominant clinical form in both groups was infiltrative tuberculosis, diagnosed in 98 (61.3%, 95% CI: 53.5-68.5) of cases in Group I and 153 (95.6%, 95% CI: 91.2-97.9) in Group II (p < 0.0001). Generalized TB was significantly more frequent in the co-infected group, in 46 patients (28.8%, 95% CI: 22.3–36.2), compared to only 4 patients in Group II (2.5% ,95% CI: 1.0-6.3) (p < 0.0001). Similarly, disseminated forms was more common in Group 1 (10 cases6.3%, 95% CI: 3.4-11.1) than in Group II (3 cases; 1.9%, 95% CI: 0.6-5.4) (p = 0.045). Lastly, nodular TB was observed only in the Group 1, affecting 6 patients (3.8%, 95% CI: 1.7-7.9). Among the 46 patients with generalized TB in Group I, 26.1% had involvement of a single extrapulmonary organ, 36.9% of two, 21.7% of three, and 15.3% of more than three organs.
Marked differences were noted in disease onset: subacute onset was dominant in Group I -115 (71.9%, 95% CI: 64.5-78.3), p < 0.0001, while insidious onset prevailed in Group II – 114 (71.3%, 95% CI: 63.8-77.7; p < 0.0001). The general condition at the time of diagnosis was more severe in Group I, with 44 (27.4%, 95% CI: 21.2-34.9; p = 0.0215) of patients classified as being in a severe or extremely severe state, compared to 17 in the HIV-negative group (10.6%, 95% CI: 6.7-16.4; p = 0.0071).
Clinical symptomatology differed significantly. Pronounced bronchopulmonary syndrome was observed in 66.2% of Group I versus 47.4% of Group II (OR = 2.17, 95% CI: 1.38-3.41; p = 0.0008). A pronounced intoxication syndrome was also more frequent in the TB/HIV group (66.9% vs. 48.2%; OR = 2.18, 95% CI: 1.38-3.42; p = 0.0008). Hematological findings reflected a more compromised status in HIV-positive patients: anemia occurred in 94 patients (58.8%, 95% CI: 51.0-66.1) vs. 37 patients (23.1%, 95% CI: 17.3-30.2) from Group II (p < 0.0001), leukopenia in 26 patients (16.3%, 95% CI: 11.3-22.7) vs. 2 patients (1.3%, 95% CI: 0.3-4.4) (p < 0.0001), and lymphocytopenia in 19 cases (11.9%, 95% CI: 7.7–17.8) vs. 2 cases (1.3%, 95% CI: 0.3-4.4) (p < 0.0001). The median erythrocyte sedimentation rate (ESR) was also higher in the HIV group (50 mm/h vs. 34 mm/h). ESR distribution differed significantly between groups, as illustrated in Fig. 1.
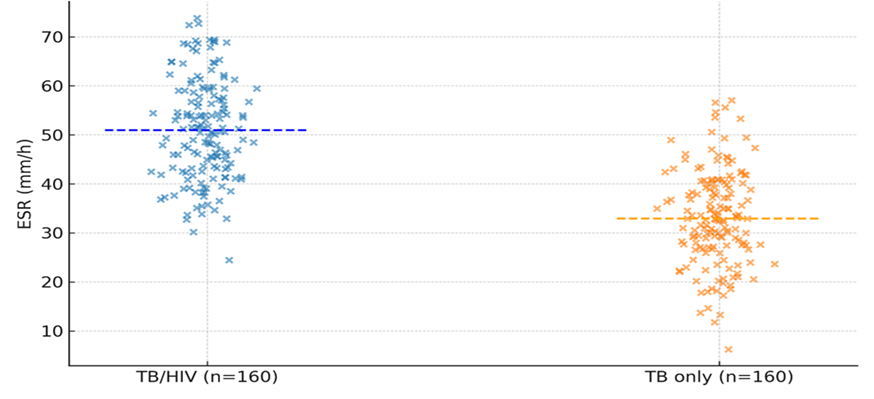 |
Fig. 1 Distribution of ESR in TB/HIV vs. TB-only patients Note: Median ESR: 50 vs. 34 mm/h (p < 0.0001). Median ESR was significantly higher in the TB/HIV group (50 mm/h) compared to TB-only patients (34 mm/h). Dashed lines indicate group medians. Statistical significance: p < 0.0001 (Mann–Whitney U test). |
Radiologically, bilateral lung involvement was slightly more frequent in Group I – 105 (65.6%, 95% CI: 57.9-72.5) vs. 95 (59.4% ,95% CI: 51.6-66.7), with more extensive lesions 116 (72.5%, 95% CI: 65.1-78.8) vs. 100 (62.5%, 95% CI: 54.8-69.6). However, pulmonary destruction (cavitary lesions) was more frequent in Group II - 95 (59.4%, 95% CI: 51.6-66.7) vs. 55 (34.4%, 95% CI: 27.5-42.0) p < 0.0001, in line with typical immune-competent responses.
From a microbiological standpoint, smear microscopy was positive in 62 cases (38.8%, 95% CI: 31.5-46.5) from Group I compared to 88 cases (55.0%, 95% CI: 47.3-62.5) in Group II (p = 0.0036). GeneXpert testing detected Mycobacterium tuberculosis in 93 patients (58.2%, 95% CI: 50.4-65.5) of Group I and 108 (67.5%, 5% CI: 59.9-74.3) of Group II. Analysis of drug-resistance patterns revealed that fully drug-susceptible tuberculosis was more common among TB-only patients, whereas resistance to at least one first-line drug was significantly higher in the TB/HIV co-infected cohort (35% vs. 22%, p = 0.013). Mono- and poly-resistance occurred at comparable frequencies between the two groups (12% vs. 10%, p = 0.61; 9% vs. 6%, p = 0.37, respectively). Multidrug-resistant TB (MDR-TB) was detected more frequently among TB/HIV co-infected patients than in HIV-negative patients (14% vs. 6%), with an odds ratio of 2.55 (95% CI: 1.15–5.66, p = 0.021).
Complications were more frequent in Group I – 77 patients (48.1%, 95% CI: 40.5-55.8) versus 33 patients (20.6%, 95% CI: 15.1-27.5) in Group II (p < 0.0001). In Group I, the most prevalent complications were cachexia (37 cases, 48.1%, 95% CI: 37.3-59.0); p < 0.0001 and pleurisy – 29 cases, (37.6%, 95% CI: 27.7-48.8), followed by hemoptysis (6.5%), pneumothorax (5.2%), and empyema (2.6%). In Group II, cachexia and hemoptysis were recorded in 12 patients (36.4%, 95% CI: 22.2-53.4), pleurisy in 8 (24.2%, 95% CI: 12.8-41.0), and pneumothorax in one case (3.0%). Empyema was not reported in Group II. Clinical complications showed distinct patterns between the two cohorts, as depicted in Fig. 2.
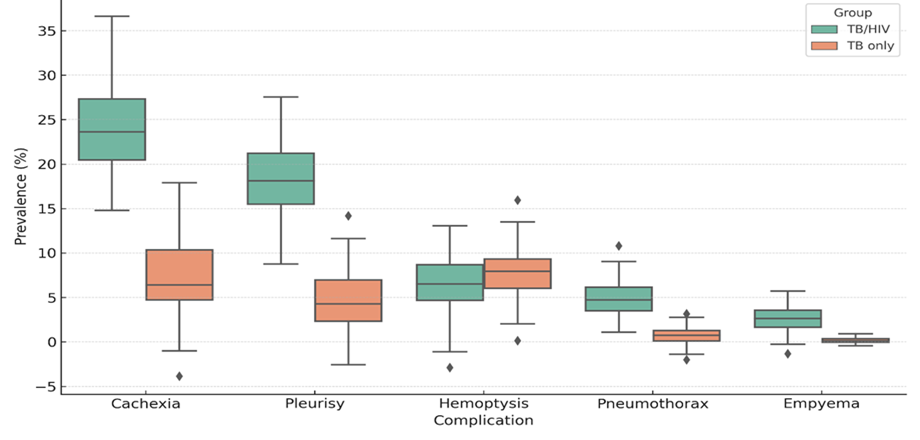 |
Fig. 2 Distribution of clinical complication prevalence in TB/HIV and TB-only patients. Note: Boxplots show higher median and greater variability in cachexia and pleurisy among TB/HIV patients. Hemoptysis shows similar distribution in both groups, while empyema and pneumothorax occurred almost exclusively in TB/HIV group. Boxes indicate interquartile range; whiskers represent 1.5×IQR. |
The frequency of comorbidities and coinfections also differed notably. Liver pathology – including hepatitis B and C, toxic hepatitis, and hepatic cirrhosis – was significantly more common in Group I, affecting 66 (41.3%, 95% CI: 33.9-49.0) compared to 36 in Group II (22.5%, 95% CI: 16.7-30.2; p < 0.0001). Syphilis was diagnosed more frequently in Group I (8.8% vs. 4.3%). Neurological comorbidities such as alcohol-related polyneuropathy and encephalopathy were documented in 9.6% of Group I versus 8.6% of Group II. Epilepsy was identified in 4.1% of Group I and 1.4% of Group II. Conversely, some conditions were more prevalent in the TB-only group. Cerebrovascular accidents occurred more often in Group II (0.8% and 2.9%).Arterial hypertension was more frequent in Group II (5.7% vs. 0.8%). Type 2 diabetes mellitus was present in 1.6% of Group I versus 8.6% of Group II (p = 0.0087), and gastric ulcer was diagnosed in 4.8% versus 14.3% (p = 0.0029), respectively. Isolated cases of laryngeal tuberculosis (1.2% vs. 0.6%), pulmonary cancer, tuberculous peritonitis, and pulmonary abscess (each 0.6%) were also noted across both groups.
Tuberculosis „masks” were identified in both groups: 44 cases (27.5%, 95% CI: 21.2-34.9) in Group I and 36 cases (22.5%, 95% CI: 16.7-29.6) in Group II. Pneumonia was observed more frequently in Group 1, affecting 28 patients (17.5%, 95% CI: 12.4-24.1) compared to 11 (6.8%, 95% CI: 3.9-11.9) cases. Notably, SARS-CoV-2 coinfection was present in 22 patients (13.8%, 95% CI: 9.3-19.9) in Group I compared to 50 patients (31.2%, 95% CI: 24.6–38.8) in Group II. Chronic obstructive pulmonary disease (COPD) was diagnosed in 0.6% of Group I and 1.9% of Group II, while bronchial asthma was reported exclusively in Group II (0.6%).
Opportunistic infections were observed exclusively in Group I – 28 patients (17.5%). The most frequent were oropharyngeal candidiasis 15 (53.6%, 95% CI: 35.8-70.5) and herpes zoster 6 (21.3%, 95% CI: 10.2-39.5), with rare conditions including cryptococcal meningitis, cerebral toxoplasmosis, Kaposi sarcoma, Pneumocystis jirovecii pneumonia, non-tuberculous mycobacteriosis, oral leukoplakia, and pulmonary aspergillosis, each identified in a single case.
Mortality was significantly higher in the co-infected group. In Group I, there were 45 deaths (28.1%, 95% CI: 21.7-35.5). Of these, 34 (75.6%, 95% CI: 61.3-85.8) were due to tuberculosis and 11 (24.4%) to tuberculosis associated with other comorbidities. In contrast, Group II recorded 11 deaths (6.9%, 95% CI: 3.9-11.9); p < 0.0001, with 7 (63.6%, 95% CI: 35.4-84.8) attributable to TB and 4 (36.4%) due to TB combined with other underlying conditions.
The clinical and radiological presentations varied significantly between the two groups (Table 1). In the TB/HIV cohort, the clinical picture was often less specific, with a higher proportion of patients presenting with subacute or insidious onset, nonspecific systemic complaints (fatigue, weight loss), and a lower frequency of classical signs such as hemoptysis, compared with the TB-only group.
Table 1. Clinical, paraclinical, and radiological manifestations in patients with tuberculosis and tuberculosis/HIV co-infection. | ||||||
Parameter | Group I (TB/HIV) | % | Group II (TB only) | % | OR [95% CI] | p-value |
Disease onset | ||||||
Asymptomatic | 12 | 7.5 | 10 | 6.3 | 1.22 [0.51–2.90] | = 0.83 |
Insidious | 32 | 20.0 | 114 | 71.3 | 0.10 [0.06–0.17] | <0.0001 |
Subacute | 115 | 71.9 | 36 | 22.5 | 8.80 [5.30–14.61] | <0.0001 |
Acute | 1 | 0.6 | – | – | NE | 1.00 |
General condition at diagnosis | ||||||
Satisfactory | 44 | 27.5 | 43 | 26.9 | 1.03 [0.63–1.70] | = 0.90 |
Moderate severity | 72 | 45.0 | 100 | 62.5 | 0.49 [0.32–0.75] | = 0.0011 |
Severe | 27 | 16.8 | 13 | 8.1 | 2.28 [1.13–4.60] | 0.0215 |
Extremely severe | 17 | 10.6 | 4 | 2.5 | 4.60 [1.51–14.01] | 0.0071 |
Bronchopulmonary syndrome | ||||||
Absent | 13 | 8.1 | 6 | 3.8 | 1.33 [0.57–3.12] | 0.50 |
Moderate | 41 | 25.7 | 78 | 48.8 | 0.41 [0.25–0.67] | 0.0003 |
Pronounced | 106 | 66.2 | 76 | 47.4 | 2.17 [1.38–3.41] | 0.0008 |
Intoxication syndrome | ||||||
Absent | 13 | 8.1 | 10 | 6.2 | 1.33 [0.57–3.12] | 0.50 |
Moderate | 40 | 25.0 | 73 | 45.6 | 0.41 [0.25–0.67] | 0.0003 |
Pronounced | 107 | 66.9 | 77 | 48.2 | 2.18 [1.38–3.42] | 0.0008 |
Hematological changes | ||||||
Anemia | 94 | 58.8 | 37 | 23.1 | 4.73 [2.92–7.68] | <0.0001 |
Leukocytosis | 38 | 23.8 | 53 | 33.1 | 0.63 [0.38–1.03] | 0.0828 |
Leukopenia | 26 | 16.3 | 2 | 1.3 |
15.33 [3.57–65.78] | <0.0001 |
Lymphocytopenia | 19 | 11.9 | 2 | 1.3 |
10.65 [2.44–46.51] | 0.0001 |
Erythrocyte sedimentation rate (mm/h) | ||||||
<20 | 29 | 18.2 | 75 | 46.9 | 0.25 [0.15–0.42] | – |
21–30 | 9 | 5.6 | 22 | 13.8 | 0.37 [0.17–0.84] | 0.0140 |
31–40 | 18 | 11.3 | 18 | 11.3 | 1.00 [0.50–2.00] |
1.0000 |
41–50 | 30 | 18.7 | 21 | 13.1 |
1.53 [0.83–2.80] | 0.1693 |
51–60 | 34 | 21.2 | 15 | 9.3 | 2.61 [1.36–5.01] |
0.0032 |
>60 | 40 | 25.0 | 9 | 5.6 | 5.59 [2.61–11.98] |
<0.0001 |
Microscopy | ||||||
Smear microscopy (AFB-positive) | 62 | 38.8 | 88 | 55.0 | 0.52 [0.33–0.81] | 0.0036 |
Molecular Genetic test |
|
|
| |||
GeneXpert positive | 93 | 58.2 | 108 | 67.5 | 0.67 [0.42–1.05] | 0.1054 |
Lesion localization | ||||||
Unilateral | 55 | 34.4 | 65 | 40.6 | 0.77 [0.49–1.21] | 0.2987 |
Bilateral | 105 | 65.6 | 95 | 59.4 | 1.31 [0.83–2.06] | 0.2987 |
Lesion extent | ||||||
Limited | 44 | 27.5 | 60 | 37.5 | 0.63 [0.39–1.01] | 0.0732 |
Extensive | 116 | 72.5 | 100 | 62.5 | 1.58 [0.99–2.54] | 0.0732 |
Pulmonary destruction | 55 | 34.4 | 95 | 59.4 | 0.36 [0.23–0.56] | 0.0000 |
Note: Odds ratios (OR) with 95% confidence intervals and p-values were omitted for variables where statistical comparison was not applicable due to low event counts, incomplete data, or non-significant variability between groups. | ||||||
The spectrum of disease manifestations, including primary and extrapulmonary involvement, also differed between the two cohorts as described in Table 2.
Table 2. Clinical forms of tuberculosis. | |||||
Clinical form | Group I (TB/HIV) | % | Group II (TB only) | % | p-value |
Nodular | 6 | 3.6 | – | – |
|
Infiltrative | 98 | 61.3 | 153 | 95.6 | <0.0001 |
Disseminated | 10 | 6.3 | 3 | 1.9 | - |
Generalized | 46 | 28.8 | 4 | 2.5 | <0.0001 |
Note: Data are presented as number of patients and percentages. Statistical comparison between groups was performed using Fisher’s exact test. A significantly higher proportion of infiltrative forms was observed in Group II (p < 0.0001), while generalized TB was more frequent in Group I (p < 0.0001). | |||||
Associated comorbidities played an important role in shaping the clinical course of patients as shown in Table 3.
Table 3. Associated diseases in patients with tuberculosis and tuberculosis/HIV co-infection. | |||||
Associated disease | Group I (TB/HIV) | % | Group II (TB only) | % | p-value |
Liver disease (hepatitis B, C, toxic hepatitis, liver cirrhosis) | 66 | 53.3 | 16 | 22.8 | <0.0001 |
Type 2 diabetes mellitus | 2 | 1.6 | 6 | 8.6 | - |
Gastric ulcer | 6 | 4.8 | 10 | 14.3 | - |
COVID-19 | 17 | 13.7 | 22 | 31.4 | - |
Syphilis | 14 | 11.3 | 3 | 4.3 | - |
Epilepsy | 5 | 4.1 | 1 | 1.4 | - |
Stroke | 1 | 0.8 | 2 | 2.9 | - |
Polyneuropathy and alcohol-related encephalopathy | 12 | 9.6 | 6 | 8.6 | - |
Arterial hypertension | 1 | 0.8 | 4 | 5.7 | - |
Note: Data are presented as number of patients and percentages. Statistical comparisons were conducted using Fisher’s exact test. A significant difference was observed only in the prevalence of liver disease, which was higher in the TB/HIV group (p < 0.0001). | |||||
Discussion
The results of this study highlight the significant impact of HIV infection on the clinical manifestations of newly diagnosed tuberculosis. A comparison of two matched cohorts revealed substantial differences in clinical presentation, disease severity, and associated comorbidities, confirming that HIV-related immunodeficiency alters the clinical spectrum of tuberculosis. These findings are consistent with existing literature indicating that tuberculosis in HIV-positive patients tends to be more severe and atypical [6, 9].
Subacute onset was predominant in the HIV group, whereas insidious onset prevailed in the HIV-negative group, suggesting that immunosuppression accelerates disease progression. Consequently, general condition at diagnosis was more severe in co-infected patients, with 27.4% classified as severe or extremely severe, compared to only 10.6% in the control group.
The clinical forms analysis revealed a significantly higher prevalence of generalized tuberculosis in the co-infected group (28.8% vs. 2.5%). Among those with generalized TB in the HIV group, 73.9% had multiple extrapulmonary involvements, indicating more extensive disease. In contrast, the infiltrative form predominated in HIV-negative patients (95.6%), suggesting typical pulmonary localization. These findings align with the study by Stoica Călăraşu C. et al., who reported higher incidence of extrapulmonary TB in HIV-positive individuals due to immunosuppression [7].
These findings justify the characterization of TB/HIV cases as “atypical”, since the clinical picture deviates from the classical pulmonary TB presentation, with diminished frequency of hallmark respiratory symptoms and predominance of nonspecific systemic manifestations.
Extensive lesions was more frequent in the HIV group, although pulmonary destruction was more common in HIV-negative patients, likely due to cavitary lesions typically formed in immunocompetent hosts.
Bronchopulmonary and intoxication syndromes were more pronounced in co-infected patients. Laboratory results showed higher frequency of anemia, leukopenia, and lymphocytopenia in the HIV group – markers of immunosuppression – while leukocytosis was more common in the HIV-negative group. Median erythrocyte sedimentation rate was also higher in the HIV group (50 mm/h vs. 34 mm/h), with 25% of cases exceeding 60 mm/h, indicating more intense systemic inflammation. Although a blunted inflammatory response would be expected in immunocompromised individuals, in our cohort ESR values were significantly higher in TB/HIV patients. This apparent paradox may be explained by the high prevalence of anemia, hypergammaglobulinemia, and co-existing chronic infections in this group, all of which are known to increase ESR independently of immune competence.
Smear positivity was lower in the HIV group, consistent with Meintjes (2024) who described lower bacillary load in disseminated or extrapulmonary forms in HIV-infected patients. However, GeneXpert detected Mycobacterium tuberculosis in a high proportion of both groups, confirming its diagnostic utility. In our study, Xpert MTB/RIF sensitivity in the TB/HIV-negative cohort was lower than expected for immunocompetent patients, despite this test being generally recognized for its high sensitivity in such populations. Possible explanations include a higher proportion of paucibacillary forms, suboptimal specimen quality, or delays in processing, which may have reduced bacterial load and test performance. The impaired immune response in HIV-infected individuals often prevents granuloma formation, facilitating the dissemination of Mycobacterium tuberculosis to extrapulmonary sites. This leads to atypical and generalized TB forms, which are frequently smear-negative and require advanced diagnostic tools for detection [16].
Furthermore, integrated screening data from Moldova revealed that in 67.5% of TB/HIV co-infection cases, tuberculosis and HIV were diagnosed simultaneously, underscoring the importance of dual testing among vulnerable populations to ensure early detection and comprehensive management [17].
Radiological findings showed more frequent bilateral and extensive lesions in co-infected patients, though cavitary lesions were less prevalent – typical for anergic forms with deficient cell-mediated immunity, where caseating necrosis and cavity formation are impaired [11].
Complications were more common in the HIV group, especially cachexia and pleurisy. In contrast, hemoptysis was more frequent in the HIV-negative group. Among comorbidities, liver pathology was more prevalent in co-infected patients, linked to viral hepatitis and drug toxicity. SARS-CoV-2 infection was more frequent in HIV-negative patients. Opportunistic diseases (e.g., oropharyngeal candidiasis, herpes zoster) were observed exclusively in the HIV group, emphasizing patient vulnerability.
Mortality was significantly higher in co-infected patients (28.1% vs. 6.9%), with tuberculosis as the primary cause in 75.6% of deaths. These findings are consistent with the 2024 Global Tuberculosis Report, which recognizes tuberculosis as the leading cause of death among HIV-positive individuals, underscoring the urgency of targeted interventions.
This study is not without limitations. Its retrospective design may inherently involve incomplete or inconsistent documentation; however, an exhaustive review of all available medical records was undertaken at the national level, including cases from the Transnistrian region, in order to minimize information bias. Although laboratory and imaging data were unavailable for a small subset of patients who either died shortly after diagnosis or initiated ambulatory treatment, matching procedures ensured comparability between groups with respect to demographic characteristics and drug resistance profiles. The analysis was restricted to a single year (2021), yet this interval was considered representative of the national epidemiological context, as no substantial differences were observed in adjacent years. Finally, the findings, while nationally representative, should be extrapolated to other settings with caution.
Conclusions
This comparative study highlights the considerable influence of HIV on the clinical presentation and progression of tuberculosis. In co-infected patients, TB more often manifests as generalized, extrapulmonary disease with subacute onset and atypical symptoms – marked by anemia, lymphopenia, systemic inflammation, and fewer cavitary lesions, and lower rates of bacteriological confirmation. Higher complication and comorbidity rates in the HIV group underscore the need for early detection, adapted diagnostic strategies, and rapid initiation of both antiretroviral and anti-TB therapy. Clinicians should maintain a high index of suspicion, especially in high-prevalence HIV settings, where TB may mimic other conditions.
Competing interests
None declared.
Author`s contribution
II performed data collection and analysis and prepared the initial manuscript draft. AU provided scientific oversight and contributed significantly to the critical revision of the manuscript. CI supported the methodological framework and participated in the interpretation of clinical parameters. AC supervised the final data interpretation and ensured the comprehensive scientific review of the article.
Ethics approval
The study protocol was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (minutes No 66 from 29.09.2023).
Informed consent for publication
Obtained.
Acknowledgements and funding
No external funding was received for this study.
Provenance and peer review
Not commissioned, externally peer reviewed.
Authors’ ORCID IDs
Igor Ivanes – https://orcid.org/0000-0002-7726-3197
Aurelia Ustian – https://orcid.org/0000-0002-2679-5767
Constantin Iavorschi – https://orcid.org/0000-0002-6371-687X
Alexandru Corlăteanu – https://orcid.org/0000-0002-3278-436X
References
- World Health Organization. Global tuberculosis report 2024. Geneva: WHO; 2024.
- Kraef C, Roen A, Podlekareva D, Bakowska E, Nemeth J, Knappik M, et al. Incident tuberculosis in people with HIV across Europe from 2012 to 2022: incidence rates, risk factors and regional differences in a multicentre cohort study. Eur Respir J. 2025;65(6):2401904. doi:10.1183/13993003.01904-2024.
Ministry of Health of the Republic of Moldova. [Tuberculosis in adults: National Clinical Protocol]. 6th ed. Chișinău: The Ministry; 2024. Romanian.
- Kraef C, Bentzon A, Roen A, Bolokadze N, Thompson M, Azina I, et al. Long-term outcomes after tuberculosis for people with HIV in Eastern Europe. AIDS. 2023;37(13):1997-2006. doi: 10.1097/QAD.0000000000003670.
- Moges S, Lajore BA. Mortality and associated factors among patients with TB-HIV co-infection in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2024;24(1):773. doi: 10.1186/s12879-024-09683-5.
- Peters JS, Andrews JR, Hatherill M, Hermans S, Martinez L, Schurr E, et al. Advances in the understanding of Mycobacterium tuberculosis transmission in HIV-endemic settings. Lancet Infect Dis. 2019;19(3):e65-e76. doi: 10.1016/S1473-3099(18)30477-8.
- Stoica Călăraşu C, Popa Miulescu AM, Turcu AA, Nitu FM. The profile of the patients with double infection HIV and TB in South West of Romania. Curr Health Sci J. 2021;47(1):107-13. doi: 10.12865/CHSJ.47.01.17.
- Meintjes G, Maartens G. HIV-associated tuberculosis. N Engl J Med. 2024;391(4):343-55. doi: 10.1056/NEJMra2308181..
- Nzuzi CN, Onyamboko M, Kokolomami J, Tukadila HA, Natuhoyila AN, Longo-Mbenza B. Factors associated with tuberculosis-HIV co-infection in diagnosis in the Nzanza Health Zone. Open Access Libr J. 2021;8(3):1-14. doi: 10.4236/oalib.1107105.
- Philipose CS, KM S, Haridas H, Ramapuram J, Rai S. Clinico-pathological profile of patients with HIV and tuberculosis co-infection. HIV AIDS Rev. 2024;23(3):204-8. doi: 10.5114/hivar/170270.
- Patel A, Pundkar A, Agarwal A, Gadkari C, Nagpal AK, Kuttan N. A comprehensive review of HIV-associated tuberculosis: clinical challenges and advances in management. Cureus. 2024;16(9):e68784. doi: 10.7759/cureus.68784.
- Chan AC, Huang SS, Wong KH, Leung CC, Lee MP, Tsang TY, et al. Changes in the epidemiology and clinical manifestations of human immunodeficiency virus-associated tuberculosis in Hong Kong. Hong Kong Med J. 2024 Aug;30(4):281-290. doi: 10.12809/hkmj2310683.
- Goncharova O, Abrahamyan A, Nair D, Beglaryan M, Bekbolotov A, Zhdanova E, et al. Triple priority: TB/HIV co-infection and treatment outcomes among key populations in the Kyrgyz Republic: a national cohort study (2018-2022). Trop Med Infect Dis. 2023;8(7):342. doi: 10.3390/tropicalmed8070342.
- Kerkhoff AD, Havlir DV. CROI 2021: tuberculosis, opportunistic infections, and COVID-19 among people with HIV. Top Antivir Med. 2021;29(2):344-51.
- Lelisho ME, Wotale TW, Tareke SA, Alemu BD, Hassen SS, Yemane DM, et al. Survival rate and predictors of mortality among TB/HIV co-infected adult patients: retrospective cohort study. Sci Rep. 2022;12(1):18360. doi: 10.1038/s41598-022-23316-4.
- Ivanes I. TB și HIV: o dublă povară în sănătatea publică [TB and HIV: a double burden in public health]. Bull Acad Sci Mold. Med Sci. 2024;(3):160-165. doi: 10.52692/1857-0011.2024.3-80.29. Romanian.
- Ivanes I, Ustian A, Iavorschi C, Popa V, Paladi C. Caracteristica cazurilor noi de tuberculoză pulmonară la persoanele care trăiesc cu HIV [Characteristics of new pulmonary tuberculosis cases in people living with HIV]. In: 5th Congress of family doctors of the Republic of Moldova with international participation; 2024 May 17-18; Chișinău, Moldova: Articles and abstracts. Chișinău: Medicina; 2024. p. 158-164. Romanian.