
Introduction
Depression is one of the most prevalent mental health conditions globally, with significant personal, social, and economic consequences. According to the World Health Organization, more than 280 million people are affected by depression worldwide, making it a leading cause of disability and a major contributor to the global burden of disease. Despite advances in mental health care and increased awareness, stigma remains a significant barrier to help-seeking, diagnosis, and treatment adherence among individuals with depression [1-3].
Stigmatization of depression manifests through negative stereotypes, prejudice, and discriminatory behavior directed at those experiencing the condition. Such beliefs may include the perception that people with depression are weak, unreliable, or dangerous, or that depression is not a real illness but rather a matter of personal will [2]. This stigmatization not only impairs the quality of life of those affected but also contributes to social exclusion, workplace discrimination, and internalized shame or self-stigma.
In Eastern European low- and middle-income countries (LMIC) such as the Republic of Moldova, research on mental health stigma remains limited, particularly in relation to depression. Historical neglect of mental health, limited access to services, and culturally embedded misconceptions contribute to the persistence of stigmatizing beliefs in this region [4, 5]. In Moldova, although reforms in mental health care have been initiated, public attitudes continue to reflect fear, misunderstanding, and reluctance to engage with individuals who suffer from depression.
Existing studies tend to focus on general stigma toward mental illness, often without differentiating between disorders. However, depression-specific stigma may take unique forms, especially regarding perceptions of functionality, employability, or moral character. Identifying which specific beliefs are most prevalent is essential for designing targeted anti-stigma interventions. Item-level analysis of validated instruments such as the Depression Stigma Scale (DSS) can provide deeper insights into the patterns of belief within a given population and guide context-sensitive strategies for stigma reduction [2, 6].
This article presents the results of an item-level statistical analysis of the DSS applied to a Moldovan sample, aiming to identify the core stigmatizing beliefs about depression in the general population. The findings may inform national efforts and those in similar LMICs regarding public education, workplace inclusion, and mental health policy.
This study aims to identify the core stigmatizing beliefs about depression in the general population of the Republic of Moldova through an item-level statistical analysis of the Depression Stigma Scale.
Material and methods
This cross-sectional study was conducted on a convenience sample of 476 adult participants from various regions of the Republic of Moldova. Inclusion criteria were: age ≥18 years, informed consent to participate. Individuals with a known diagnosis of psychotic disorders or cognitive impairment were excluded.
The study was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (minutes No 44, from 29.05.2024), and all participants provided written informed consent.
To assess stigmatizing beliefs about depression, the Depression Stigma Scale (DSS) was used, which contains 9 items measuring the extent of agreement with commonly held stigmatizing beliefs (e.g., “Depression is a sign of personal weakness”, “I would not employ someone if I knew they had been depressed”, “Depression is not a real medical illness”). Responses were recorded on a 5-point Likert scale from 0 (“strongly disagree”) to 4 (“strongly agree”).
Sociodemographic data were also collected, including age, gender, education, employment status, income, marital status, and urban/rural residence.
Descriptive statistics (mean, standard deviation, minimum, maximum) were calculated for each of the 9 DSS items. Item-level analysis was conducted to examine the distribution and intensity of stigma-related beliefs. Results were presented in the form of bar plots for visualization.
Although the analysis focused primarily on descriptive patterns, inferential comparisons between items were also explored to identify statistically significant differences in the endorsement of specific beliefs. Data were analyzed using SPSS version 24.0, with a significance level set at p < 0.05.
Results
A total of 476 individuals participated in this cross-sectional study on stigma toward depression in the Republic of Moldova. The sample included 301 urban residents (63.2%) and 175 rural residents (36.8%), reflecting the geographic distribution of the population and mental health service access. Participants were recruited from 10 administrative units across the country, including both major urban centers (e.g., Chișinău and Bălți) and smaller districts (e.g., Orhei, Călărași, Ialoveni), to ensure diversity in socio-demographic backgrounds.
The sample was composed of 281 women (59%) and 195 men (41%), with ages ranging from 18 to 65 years (mean age = 34.5 years). Educational attainment was distributed as follows: 36.3% (n = 173) had completed 9 years of school, 25.2% (n = 120) had finished 12 years or vocational school, 19.1% (n = 91) had graduated from college, and 10.9% (n = 52) held a university degree. A small proportion, 8.4% (n = 40), reported having completed only primary education.
This stratified sampling approach was designed to ensure representation across key sociodemographic groups relevant to mental health literacy and stigma. It also allowed for later analysis of stigma variation by gender, education, and area of residence.
The Depression Stigma Scale (DSS) was used to assess the level of stigmatizing beliefs toward people with depression. The analysis of item-level responses revealed that the highest agreement rates were observed for the following items: “People with depression could snap out of it if they wanted”, “Depression is a sign of personal weakness”, and “Depression is not a real medical illness”. These beliefs suggest a persistent conceptual stigma, in which depression is perceived as a lack of willpower or not being a genuine illness.
High scores were also recorded for item – “I would not employ someone if I knew they had been depressed”, suggesting occupational stigma and the belief that individuals with depression are unfit for professional roles.
Conversely, the items with the lowest levels of agreement were: “People with depression are dangerous”, “It is best to avoid people with depression so you don’t become depressed yourself”, and “People with depression are unpredictable”, indicating that fear-based and avoidance-related stigma were less prevalent in this sample.
The average score for the item “People with depression could snap out of it if they wanted” was 3.4 (on a 5-point scale), whereas “People with depression are dangerous” had a mean score of just 1.8. This confirms that the dominant stigma in the Moldovan context tends to be conceptual and occupational rather than fear-based or exclusionary.
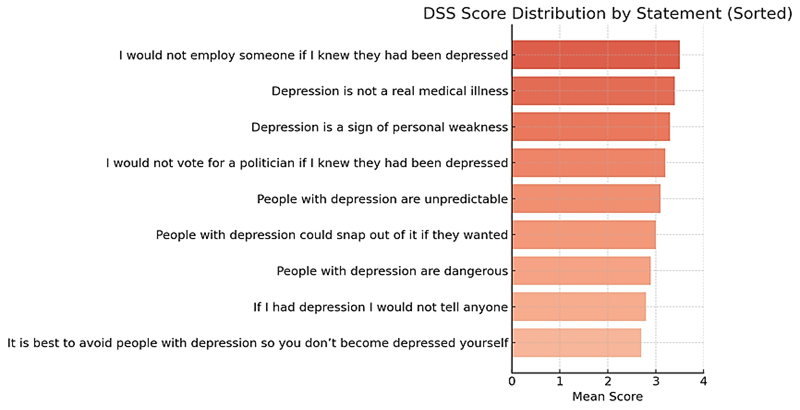 |
Fig. 1 Mean scores for stigmatizing beliefs about depression Note: The chart displays the average agreement level (on a 0–4 Likert scale) with each of the nine DSS items, sorted from highest to lowest mean score. Higher scores indicate stronger endorsement of the respective stigmatizing belief. |
Analysis of stigma variation by gender revealed that men had significantly higher agreement with items suggesting dangerousness and unpredictability. For example, the average score for “People with depression are dangerous” among men was 2.1, compared to 1.6 among women (p < 0.01).
Educational level also influenced stigma levels. Respondents with only secondary education were more likely to agree with stigmatizing statements such as “Depression is not a real medical illness” (mean score 3.7 vs. 2.9 among those with higher education; p < 0.001).
Urban respondents generally showed lower stigma levels across most items compared to rural respondents, particularly on items relating to avoidance and employment discrimination.
In terms of self-stigma, items “If I had depression I would not tell anyone” and “I would not vote for a politician if I knew they had been depressed” – revealed moderate agreement, suggesting a significant degree of anticipated discrimination and secrecy.
The internal consistency of the scale was high (Cronbach’s Alpha = 0.91), confirming the reliability of the instrument in the Moldovan context.
Discussion
This study provides a comprehensive analysis of public attitudes toward depression in a representative sample in the Republic of Moldova, using the Depression Stigma Scale (DSS). The results reveal that stigmatizing beliefs remain prevalent, particularly those that conceptualize depression as a personal weakness or a lack of willpower. The most frequently endorsed items were: “People with depression could snap out of it if they wanted,” “Depression is a sign of personal weakness,” and “Depression is not a real medical illness.” These findings align with prior research highlighting the persistence of conceptual stigma in LMICs, where mental illness is often viewed through a moral or characterological lens rather than a biomedical one [2, 7, 8].
Moreover, the relatively high agreement with occupational stigma – such as “I would not employ someone if I knew they had been depressed” – indicates that discriminatory attitudes may translate into tangible social and economic exclusion. This echoes findings from studies conducted in LMICs, including in Eastern Europe, where mental illness is still associated with reduced trust in competence and productivity [3 ,9, 10].
Conversely, items reflecting fear-based and avoidance stigma (e.g., “People with depression are dangerous” and “It is best to avoid people with depression”) were less frequently endorsed. This pattern suggests that although respondents may not view individuals with depression as threatening, they still hold beliefs that contribute to marginalization and discrimination, especially in the workforce and public life [9, 11, 12].
The analysis also demonstrated statistically significant variations in stigma levels across sociodemographic groups. Male respondents exhibited higher endorsement of beliefs related to dangerousness and unpredictability, consistent with gender-based differences observed in international literature. Educational attainment was inversely associated with stigma, with individuals holding only secondary education more likely to deny the medical legitimacy of depression. Similarly, stigma scores were higher among respondents residing in rural areas, supporting evidence that urban environments may provide greater exposure to mental health information and services [13, 14].
Self-stigmatizing attitudes were also evident. Items such as “If I had depression, I would not tell anyone” and “I would not vote for a politician if I knew they had been depressed” revealed moderate levels of internalized stigma and anticipated discrimination. These beliefs are of particular concern, as self-stigma has been shown to negatively impact help-seeking behavior and adherence to treatment [15-17].
The internal consistency of the DSS was high (Cronbach’s Alpha = 0.91), confirming its reliability for use in the Moldovan context. The item-level analysis allowed for a nuanced understanding of specific stigma domains – conceptual, occupational, fear-based, and self-stigma – highlighting the complex ways in which public perceptions about depression are structured [18].
Taken together, these findings underscore the need for adapted anti-stigma interventions in in LMICs, such as Republic of Moldova. Efforts should focus on increasing mental health literacy, challenging harmful stereotypes, and promoting recovery-oriented narratives. Special attention should be given to men, individuals with lower educational attainment, and rural communities, where stigma levels are highest. Public health campaigns, inclusion of mental health education in school curricula, and peer-led awareness initiatives may serve as effective tools for reducing stigma [19-21].
Future research should explore causal pathways through longitudinal designs and assess the effectiveness of anti-stigma programs in LMIC settings. Additionally, qualitative studies may offer deeper insights into the lived experiences of individuals affected by depression and stigma.
Conclusion
This study provides the first item-level analysis of depression stigma in the Republic of Moldova, offering a nuanced understanding of the specific beliefs that sustain stigma in a low- and middle-income country context. The findings reveal that the most strongly endorsed beliefs relate to questioning the medical legitimacy of depression, attributing it to personal weakness, and concerns about the employability of individuals with depression. In contrast, fear-based beliefs, such as the idea that people with depression are dangerous or should be avoided, were less commonly held. These insights represent a valuable contribution to the evidence base needed to design targeted and culturally adapted anti-stigma interventions in LMICs.
Competing interests
None declared.
Authors’ contribution
JC conceived the study, led the study design, coordinated the data collection process, and drafted the manuscript. AE contributed to the study design, supervised the analysis, and revised the manuscript critically. IN performed statistical analysis and supported interpretation of the findings. ID and AB participated in data collection and contributed to manuscript preparation. CA and RC assisted with participant recruitment and data entry. MB, MBel, and DJ conducted literature review and formatting. RP contributed to data visualization and statistical validation. All authors reviewed the manuscript critically and approved the final version for publication.
Informed consent for publication
Obtained.
Ethics approval
The study was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (minutes No 44, from 29.05.2024).
Acknowledgements and funding
The authors gratefully acknowledge PhD Associate Professor Evelina Gherghelijiu for her essential support in coordinating the research process and managing participant recruitment and data collection. We thank PhD Associate Professor Oleg Arnaut for his contribution to the statistical analysis and validation of the findings. Special appreciation is extended to Dr.P.H. Emily Peca, M.A., Adjunct Faculty at the Milken Institute School of Public Health, George Washington University, for her expert guidance throughout the study design and interpretation phases. We also wish to thank Professor Kathleen M. Griffiths, former Director of the National Centre for Mental Health Research, Australian National University, for her foundational role in developing the Depression Stigma Scale (DSS), which served as the core measurement instrument in this study. Finally, we express our deep gratitude to all participants for their openness and contribution to this research.
This study was realized in the framework of the "Implementation Science Study to investigate community-based mental health interventions for high-risk communities in low- and middle-income countries" HEARD, 2024, financed by USAID
Provenance and peer review
Not commissioned; externally peer-reviewed.
Authors’ ORCID IDs
Jana Chihai – https://orcid.org/0000-0002-7720-5544
Andrei Eșanu – https://orcid.org/0000-0003-1289-4622
Igor Nastas – https://orcid.org/0000-0001-8751-9101
Inga Deliv – https://orcid.org/0000-0001-6080-9256
Alina Bologan – https://orcid.org/0000-0002-1771-7476
Cornelia Adeola – https://orcid.org/0009-0002-0728-9196
Radislav Coșulean – https://orcid.org/0000-0001-8699-6862
Madalina Bivol – https://orcid.org/0009-0005-2827-9992
Mihaela Belous – https://orcid.org/0000-0002-2597-1060
Dorin Jelaga – https://orcid.org/0009-0004-7761-450X
Romil Popescu – https://orcid.org/0009-0007-6414-7377
References
Esanu A, Morais V, Araújo J, Ramos E. Stigma toward people with mental disorders in adolescents: comparison between Portugal and Moldova. Porto Biomed J. 2020;5(6):e089. doi: 10.1097/j.pbj.0000000000000089.
Al-Shannaq Y, Jaradat D, Ta’an WF, Jaradat D. Depression stigma, depression literacy, and psychological help seeking attitudes among school and university students. Arch Psychiatr Nurs. 2023 Oct;46:98-106.doi: 10.1016/j.apnu.2023.08.010.
Pybus K, Pickett KE, Lloyd C, Wilkinson R. The socioeconomic context of stigma: examining the relationship between economic conditions and attitudes towards people with mental illness across European countries. Front Epidemiol. 2023;3:1076188. doi: 10.3389/fepid.2023.1076188.
Thornicroft G, Brohan E, Rose D, Sartorius N, Leese M. Global pattern of experienced and anticipated discrimination against people with schizophrenia: a cross-sectional survey. Lancet. 2009 Jan 31;373(9661):408-15. doi: 10.1016/S0140-6736(08)61817-6.
Rüsch N, Angermeyer MC, Corrigan PW. Mental illness stigma: concepts, consequences, and initiatives to reduce stigma. Eur Psychiatry. 2005 Dec;20(8):529-39. doi: 10.1016/j.eurpsy.2005.04.004.
Corrigan PW, Watson AC. Understanding the impact of stigma on people with mental illness. World Psychiatry. 2002 Feb;1(1):16-20.
Hansson L, Jormfeldt H, Svedberg P, Svensson B. Mental health professionals’ attitudes towards people with mental illness: do they differ from attitudes held by people with mental illness? Int J Soc Psychiatry. 2013 Mar;59(1):48-54. doi: 10.1177/0020764011423176.
Griffiths KM, Christensen H, Jorm AF. Predictors of depression stigma. BMC Psychiatry. 2008 Apr 18;8:25. doi: 10.1186/1471-244X-8-25.
Mak WWS, Poon CYM, Pun LYK, Cheung SF. Meta-analysis of stigma and mental health. Soc Sci Med. 2007 Jul;65(2):245-61.doi: 10.1016/j.socscimed.2007.03.015.
Pescosolido BA, Medina TR, Martin JK, Long JS. The “backbone” of stigma: identifying the global core of public prejudice associated with mental illness. Am J Public Health. 2013 May;103(5):853-60. doi: 10.2105/AJPH.2012.301147.
Lasalvia A, Zoppei S, Van Bortel T, Bonetto C, Cristofalo D, Wahlbeck K, et al. Global pattern of experienced and anticipated discrimination reported by people with major depressive disorder: a cross-sectional survey. Lancet. 2013 Nov 9;381(9860):55-62. doi: 10.1016/S0140-6736(12)61379-8.
Schomerus G, Schwahn C, Holzinger A, Corrigan PW, Grabe HJ, Carta MG, et al. Evolution of public attitudes about mental illness: a systematic review and meta-analysis. Acta Psychiatr Scand. 2012 Jun;125(6):440-52. doi: 10.1111/j.1600-0447.2012.01826.x.
Rüsch N, Müller M, Ajdacic-Gross V, Rodgers S, Corrigan PW, Rössler W. Shame, perceived knowledge and satisfaction associated with mental health as predictors of attitude patterns towards help-seeking. Epidemiol Psychiatr Sci. 2014 Jun;23(2):177-87. doi: 10.1017/S204579601300036X.
Evans-Lacko S, Brohan E, Mojtabai R, Thornicroft G. Association between public views of mental illness and self-stigma among individuals with mental illness in 14 European countries. Psychol Med. 2012 Jan;42(8):1741-52. doi: 10.1017/S0033291711002558.
Dinos S, Stevens S, Serfaty M, Weich S, King M. Stigma: the feelings and experiences of 46 people with mental illness. Br J Psychiatry. 2004 Dec;184:176-81. doi: 10.1192/bjp.184.2.176.
Reavley NJ, Jorm AF. Public recognition of mental disorders and beliefs about treatment: changes in Australia over 16 years. Br J Psychiatry. 2012 Jun;200(5):419-25. doi: 10.1192/bjp.bp.111.104208.
Livingston JD, Boyd JE. Correlates and consequences of internalized stigma for people living with mental illness: a systematic review and meta-analysis. Soc Sci Med. 2010 Dec;71(12):2150–61.doi: 10.1016/j.socscimed.2010.09.030.
Esanu A, Chihai J. Stigmatizarea persoanelor cu depresie [Stigma towards people with depression]. Stud Univ Mold (Educ Sci Ser). 2018;(9):41-44. Romanian.
Wasserman D, Apter G, Baeken C, Bailey S, Balazs J, Bec C, et al. Compulsory admissions of patients with mental disorders: State of the art on ethical and legislative aspects in 40 European countries. Eur Psychiatry. 2020;63(1):e82. doi: 10.1192/j.eurpsy.2020.79.
Chihai J, Spinei L, Cerniţanu M, Garaz G, Eşanu A, Bologan A. Probleme psihosociale determinate de pandemia COVID-19 = Psychosocial problems caused by the COVID-19 pandemic. Mold J Health Sci. 2020;(2):161-169. Romanian, English.
Harhaji S, Tomori S, Nakov V, Chihai J, Radić I, Mana T, Stoychev K, Esanu A, Pirlog MC. Stigmatising attitudes towards mental health conditions among medical students in five South-Eastern European countries. Zdr Varst. 2024 Sep 23;63(4):188-197. doi: 10.2478/sjph-2024-0025.