
Introduction
Overactive bladder (OAB) is a prevalent disorder impacting a significant segment of the population, especially women, and its prevalence increases with age. The main symptoms are urgency, frequent urination, nocturia, and urge incontinence [1, 2]. OAB may be characterized as a hypersensitivity condition in which patients manifest increased urge sensations at lower volumes of bladder filling compared to normal healthy individuals. In a study of 45 women and cystometric testing, all those who reported OAB symptoms gave significantly greater sensation of bladder filling at 25%, 50%, and 75% of the bladder’s full capacity irrespective of the frequency of their urgency episodes [3].
Postmenopausal women have a higher probability to suffer from OAB symptoms due to physiological alterations like the reduced amount of estrogen or the weakened pelvic floor muscles [1, 4]. Estrogen receptors within the urogenital tract are sensitive to the hormonal fluctuations that accompany menopause [5].
The intradetrusor injection of botulinum toxin (BoNT-A) in patients with refractory OAB has been commonly documented. Leong's review found that approximately 80% of participants achieve a positive response to this treatment regimen, this treatment reduces the frequency of urination by 12-53% and the amount of urinary incontinence by 35-87% [6, 7]. Clinical efficacy of the therapy with 100 U BoNT-A was the same in older and younger women [8].
Material and methods
During the period 2022–2024, 76 women presenting with overactive bladder symptoms and referred to the Timofei Moșneaga Republican Clinical Hospital were retrospectively analyzed. Patients were categorized into two groups based on age: - reproductive age (RP, n = 49) and climacteric period (CP, n = 27). The study included an analysis of the clinical and urodynamic data from 30 patients with OAB resistant to conservative treatment, performed before and after the injection of BoNT-A. The inclusion criteria included: women older than 18 years, diagnosed with OAB, according to the International Continence Society (ICS) criteria. Exclusion criteria: post-void residual volume >10 ml assessed via USG, acute urinary tract infections, neurological diseases.
All enrolled patients completed 3-day voiding diary, the ICIQ-OAB questionnaire before and after injection. The urodynamic testing was performed to confirm detrusor overactivity (DO) using Medica SpA (Memphis Division, Medolla, Italy). and included: uroflowmetry, cystometry, pressure flow study, and ultrasound of the urinary bladder to evaluate the post-micturition urine volume.
BoNT-A intradetrusor injections were performed under intravenous anesthesia, following antibiotic prophylaxis with Ciprofloxacin 500 mg (KRKA, Slovenia). A dose of 100U BoNT-A (Neuronox®, Medytox Inc., Korea), diluted in 10 ml of 0.9% NaCl, was administered using rigid cystoscop (Karl Storz 19Fr rigid cystoscope). After bladder filling with ~150 ml NaCl 0.9%, injections were delivered supratrigonally using a 5Fr, 4 mm rigid needle, inserting ~2–3 mm into the detrusor. Twenty injections (10 U/mL, 0.5 ml/site) were distributed ~1 cm apart. The trigone, ventral wall, and dome were avoided. The bladder was emptied post-procedure.
Ethical considerations. Prior to enrollment, informed consent was obtained from all patients. The study was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy of Republic of Moldova (Approval No. 24/05.03.2021). Patients who underwent the surgical procedure were required to confirm their understanding of its nature before consenting to the operation by signing an informed consent form.
Statistical methods. Statistical analysis of the data was processed using programs IBM SPSS v.27, RStudio and MedCalc. The comparison of frequencies observed in discrete categories between two or more independent groups was performed using the χ2 test (with the application of continuity correction for adjustment), with probability reporting (p). In the Kruskal-Wallis test, the values of the test (χ2), degrees of freedom (df), effect size (ε² – epsilon square), and probability (p) were reported. Continuous variables were presented using descriptive statistics (median, mean, standard deviation, standard mean error, intervariable interval, and coefficients of variation – CFV). The comparison of the coefficients of variation (CVC) in the independent groups was performed based on the Forkman method, with the reporting of probability (p), the value of the statistical test (F), and the confidence interval (95% CI). Statistical significance was set atp < 0.05.
Results
The total ICIQ-OAB score showed a statistically significant difference in the distribution of OAB symptom severity between the age groups (RP/CP). In the group of women with a climacteric period, 100% of cases (n = 27) had increased severity (ICIQ-OABST ≥ 8), and in women of reproductive age, moderate severity level predominated in 55.10% of cases (n = 27); those with increased severity followed next, at 44.90% (n = 22).
Significant differences in bladder sensitivity indices were observed between the age groups (Table 1). The reproductive age (RP) group had higher average values for the urine retention duration index (SRBDDuration) (p < 0.001; d > 0.8). Conversely, the climacteric period (CP) group had higher mean scores for the patient’s perception of the intensity of voiding urgency (PPIUS) (p < 0.001 d > 0.8).
A Chi-square test revealed a statistically significant difference in PPIUS levels between the RP and CP groups (χ²(3) = 71.79, p < 0.001), with a large effect size (Cramér's V = 0.972).
Table 1. Self-reported indices of bladder sensitivity (voiding diary) in women with OAB | |||||||||||
| Group | Average | SD | SE | tWelch | p | MD | SED | CI95% | dCohen | |
Lower limit. | Upper limit | ||||||||||
PPIUS | RP (n = 49) | 1.551 | 0.503 | 0.072 | -13.965 | < .001 | -1.819 | 0.130 | -2.08 | -1.557 | -3.40 |
CP (n = 27) | 3.370 | 0.565 | 0.109 | ||||||||
SRBD duration | RP (n = 49) | 22.653 | 7.576 | 1.082 | 8.793 | < .001 | 12.838 | 1.460 | 9.92 | 15.749 | 1.98 |
CP (n = 27) | 9.815 | 5.092 | 0.980 | ||||||||
PPBC | RP (n = 49) | 4.796 | 0.889 | 0.127 | -2.306 | 0.024 | -0.426 | 0.185 | -0.79 | -0.057 | -0.53 |
CP (n = 27) | 5.222 | 0.698 | 0.134 | ||||||||
Note: RP – reproductive period; CP – climacteric period; PPIUS – patient's perception of the intensity of the voiding emergency; SRBDduration – duration of urine retention; PPBC – the patient's perception of the condition of the bladder; SD – standard deviation; SE – standard error; tWelch – test t (Welch); p – probability; MD – average difference; SED – standard error difference; CI95% – confidence interval 95%; dCohen – Effect Size (coefficient d according to Cohen). | |||||||||||
Patient perception about bladder condition, measured by the PPBC questionnaire, was significantly different between groups (p = 0.024). The mean score was higher in the climacteric period group (5.22 ± 0.70) compared to the reproductive age group (4.80 ± 0.89).
In the assessment of the total cohort of women with OAB, disregarding the age group factor, an almost analogous distribution regarding the various levels of severity of the PPBC index was noted (moderate problems, 38%; severe problems, 29%; and very severe problems, 33%). This distribution was not statistically significant (χ2 = 0.974; p = 0.615).
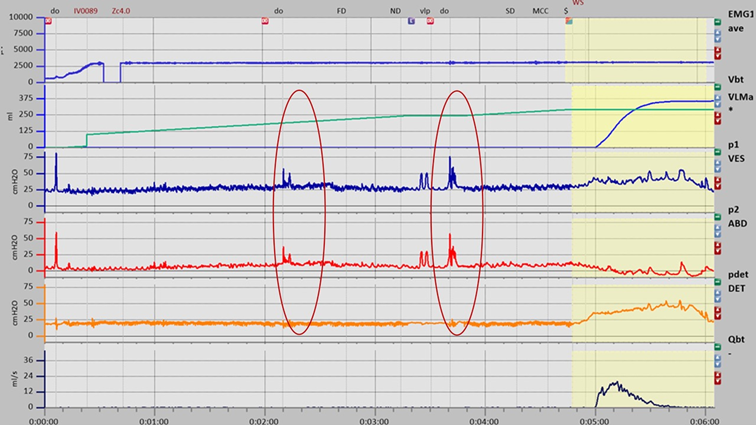 |
Fig. 1 Urodynamic test in women with refractory OAB before BoNT-A injection. Phasic detrusor contractions. Note: DO – detrusor overactivity; FD – first desire to void; ND – normal desire to void; SD – strong desire to void; MCC – maxim cystometric capacity; Vlp – Valsalva leak point; EMG – electromyography; Vbt – infused volume; P1ves – intravesical pressure; P2abd – intraabdominal pressure; Pdet – detrusor pressure; Qbt – flow rate of urine. |
In females with OAB during the menopausal transition (Fig. 1), mean values of urodynamic indices tended to be lower (Table 2), with statistical significance for the following parameters (in decreasing order of probability): p < 0.001, urinary index IU (large effect size d > 0.8), strong urge to urinate SDV (large effect size d > 0.8), estimated isovolumetric pressure – modified PIP1 (moderate effect size d > 0.5).
Table 2. Urodynamic indices in women with OAB in reproductive and climacteric period group | |||||||||||
UDS | Group | Average | SD | SE | tWelch | p | MD | SED | CI95% | dCohen | |
Lower limit | Upper limit | ||||||||||
FSV | RP (n = 49) | 64.735 | 17.379 | 2.483 | 50.908 | 0.452 | 3.290 | 4.341 | -5.425 | 12.00 | 0.183 |
CP (n = 27) | 61.444 | 18.502 | 3.561 | ||||||||
FDV | RP (n = 49) | 92.612 | 14.283 | 2.040 | 36.894 | 0.162 | 7.057 | 4.950 | -2.975 | 17.08 | 0.364 |
CP (n = 27) | 85.556 | 23.436 | 4.510 | ||||||||
SDV | RP (n = 49) | 117.633 | 15.837 | 2.262 | 40.923 | < .001 | 17.188 | 4.830 | 7.434 | 26.94 | 0.892 |
CP (n = 27) | 100.444 | 22.171 | 4.267 | ||||||||
MCC | RP (n = 49) | 150.245 | 24.868 | 3.553 | 36.071 | 0.841 | 1.800 | 8.906 | -16.26 | 19.86 | 0.052 |
CP (n = 27) | 148.444 | 42.436 | 8.167 | ||||||||
PIP1 | RP (n = 49) | 68.218 | 12.744 | 1.821 | 62.350 | 0.007 | 5.481 | 1.969 | 1.56 | 9.417 | 0.582 |
CP (n = 27) | 62.737 | 3.896 | 0.750 | ||||||||
Note: RP – reproductive period; CP – climacteric period; FSV – first sensation of urination (ml); FDV – first desire of voiding (ml); SDV – strong desire of voiding (ml); MCC – maximum cystometric capacity of the bladder (ml); PIP1 – Estimated isovolumetric pressure – modified; SD – standard deviation; SE – standard error; tWelch – test t (Welch); p – probability; MD – average difference; SED – standard error difference; CI95%–confidence interval 95%; dCohen – Effect Size (coefficient d according to Cohen). | |||||||||||
In the study, all patients who received drug treatment were managed for 6 months with combined conservative treatment: anticholinergic medication (66.6%) and selective β3-adrenoceptor agonists (43.3%). This treatment resulted in symptom improvement in 52.6% of the cases. The remaining 47.3% of the cases (19 patients in the reproductive period and 11 patients in the climacteric period) were non-responders to the treatment and thus invited for third-line therapy (intradetrusor injection of botulinum toxin type A).
Intravenous anesthesia was used during the surgical intervention. All subjects undergoing the procedure were administered prophylactic antibiotics (Ciprofloxacin 500 mg). The dosage utilized was 100 IU of BoNT-A (Neuronox®, Medytox Inc., Korea) and this dosage was diluted in 10 ml of 0.9% saline solution. The bladder was dilated under Karl Storz 19Fr rigid cystoscope guidance by infusing approximately 150-200 ml of NaCl at a concentration of 0.9%. A 5 Fr, 4 mm long rigid injection needle and was used to inject BoNT-A supratrigonally into the detrusor muscle (2-3 mm), in twenty separate locations with each injection site receiving 10 units/mL in 0.5 ml, spaced about 1 cm apart. Care was taken to avoid the bladder trigone, ventral wall, and dome due to their proximity to the peritoneal cavity. Post-injection, the bladder was drained using Foley an 18 Fr urethral catheter [9].
The OAB symptoms were present in all cases in patients prior to BoNT-A injection (Fig. 2). Botulinum toxin improved urinary symptoms, with daytime frequency decreasing in 40% of patients and urinary urgency decreasing in 71%. After detrusor BoNT-A injection, 73.9% of patients reported the resolution of nocturia symptoms.
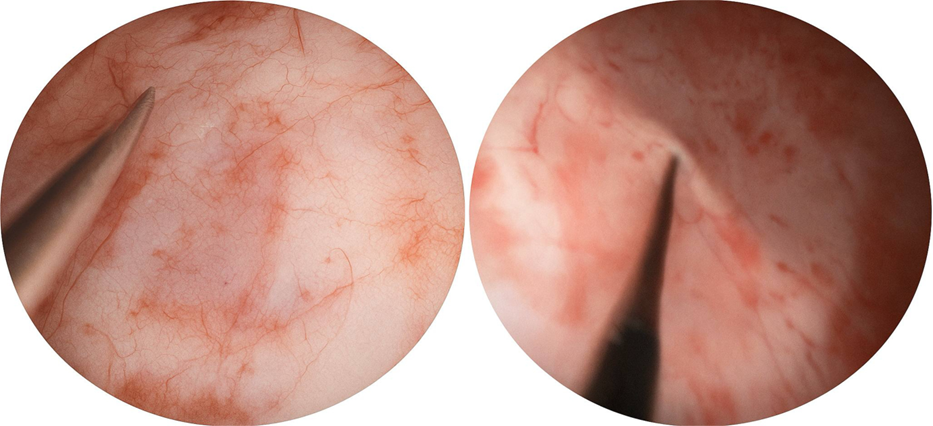 |
Fig. 2 Intradetrusor BoNT-A injections in women with refractory OAB. |
Two weeks after the BoNT-A injections, patients showed improvements in urinary frequency (41.7%), nocturia (26.1%), and urinary urgency scores (34.1%) compared to baseline measurements.
Table 3. Injection efficacy according to the degree of impairment of symptoms from ICIQ-OAB questionnaire | ||
Severity of ICIQ-OAB | BoNT-A pre-injection
(n = 30) | BoNT-A post-injection (after 2 weeks) (n = 30) |
Absence of symptoms | 0 | 21 (70%) |
Mild | 18 (60%) | 9 (30%) |
Severe | 12 (40%) | 0 |
Note: ICIQ-OAB – overactive bladder symptoms questionnaire; BoNT-A – botulinum toxin type A. | ||
The severity of LUTS/OAB, measured by the ICIQ-OAB questionnaire, showed a statistically significant reduction (Table 3).
Table 4. Refractory OAB before and after surgery | |||
Urodynamic parameters | BoNT-A pre-injection
(n = 30) | BoNT-A post-injection (after 2 weeks) (n = 30) | |
Cystometry | FS (ml) | 82.7 ± 61.22 | 290.03 ± 29.33 |
FDV (ml) | 123.5 ± 112.3 | 313.3 ± 33.6 | |
SDV (ml) | 170 ± 135 | 315 ± 28.2 | |
MCC (ml) | 194.57 ± 150.93 | 333.56 ± 37.7 | |
PIP1 | 119.4 ± 39.2 | 54.9 ± 7.52 | |
Note: FS – first sensation of bladder filling; FDV – first desire to void; SDV – strong desire to void; MCC – maximum cytometric bladder capacity; PIP1 – Estimated isovolumetric pressure-modified; BoNT-A – botulinum toxin type A. | |||
UDS performed after 2 weeks of injections (fig. 3) demonstrated an enhancement in bladder capacity/sensation, the complete absence of phasic detrusor contractions, and a normalization of detrusor pressure levels (Table 4).
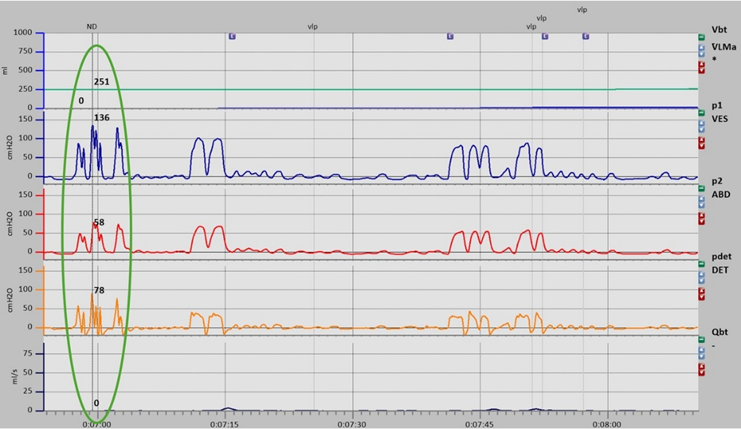 |
Fig. 3 Urodynamic test in women with refractory OAB after BoNT-A injection. Note: ND – normal desire to void; Vlp – Valsalva leak point; EMG – electromyography; Vbt – infused volume; P1ves – intravesical pressure; P2abd – intraabdominal pressure; Pdet – detrusor pressure; Qbt – flow rate of urine. |
In the current cohort of 27 patients undergoing intravesical therapy with BoNT-A, 4 instances of urinary tract infection were identified, representing 14.8% of the cases, confirmed by positive urine cultures. The average of PVR was 3.9 ml, indicating the absence of postinjection acute urinary retention and the low urinary flow rate.
Discussion
Patients with overactive bladder (OAB) exhibit heightened sensitivity to bodily signals, which can evoke somatic or psychological symptoms. Younger and older OAB patients void with similar frequency, mean voided volume, and urge severity, with no differences noted in nocturia or bladder fullness sensation between the age groups. Perceptions of bladder fullness in asymptomatic older adults were compared to OAB patients at different ages and the result showed that age-related changes are a contributing factor in the development of overactive bladder. To confirm storage dysfunction signs aligning with the ICS-established OAB criteria the Sensation-related bladder diaries can be used [10].
In our qualitative evaluation of the PPIUS index, we observed that the perception of voiding urgency intensity was most often of moderate severity in women with OAB, with variations depending on age group. In the reproductive age (RP) group, moderate severity was the most common (55%, n = 27), followed by the mild variant (45%, n = 22), and no other levels of severity were recorded. In the climacteric period (CP), severe cases were the most common (56%, n = 15), followed by the highest degree (PPIUS = 4), urinary incontinence (41%, n = 11), and moderate severity was the most common (4%, n = 1), with no instances of mild severity recorded.
According to the literature, the age did not appear to significantly influence the voided volume associated with bladder feelings, as assessed through sensation-related bladder diaries [10], but the indices of the clinical questionnaires in OAB patients (total scores) showed significant differences in the mean values between the groups of OAB patients of different age groups (RP/PC), with higher values in women in the climacteric period than in those of reproductive age (p < 0.001). In patients of climacteric age, the clinical manifestations assessed according to the questionnaires were characterized by a narrower range of responses regarding frequency, intensity, and severity compared to patients of reproductive age.
The assessment of bladder sensitivity in patients with OAB also showed significant differences. In the reproductive age (RP), 51% of the patients had moderate problems, 31% had severe problems, and 18% had very severe problems. The differences in proportions were significant (p = 0.02). In the group of women in the climacteric period (CP), the following order of magnitude was observed: 15% of the patients had severe problems, and the differences in proportions were not significant (p = 0.10).
Conclusions
The study showed that the women from both groups had different levels of symptoms. Women in the reproductive period had some moderate symptoms, whereas women in the climacteric period had more severe symptoms. The intradetrusor injections of 100U BoNT-A were proven effective in the management of hard-to-manage OAB with a DO established on UDS.
Competing interests
None declared.
Authors’ contributions
Both authors participated in the study design and contributed to drafting the manuscript. The authors critically reviewed the work and approved the final version of the manuscript.
Ethics approval
The research project was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes no. 24 from 05.03.2021).
Patient consent
Obtained.
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer reviewed.
Authors’ ORCID IDs
Mihaela Ivanov – https://orcid.org/0000-0002-5990-320X
Emil Ceban – https://orcid.org/0000-0002-1583-2884
References
Choi SJ, Lee H, Kim DI. Thread embedding acupuncture in postmenopausal women with overactive bladder: a prospective, single-arm, before-after study. Int J Womens Health. 2024;16:2287-2296. doi: 10.2147/IJWH.S494135.
Palmer MH, Willis-Gray MG. Overactive bladder in women. An evidence-based review of screening, assessment, and management. Am J Nurs. 2017;117(4):34-41. doi: 10.1097/01.NAJ.0000515207.69721.94.
Yamaguchi O, Honda K, Nomiya M, Shishido K, Kakizaki H, Tanaka H, et al. Defining overactive bladder as hypersensitivity. Neurourol Urodyn. 2007;26(6 Suppl):904-907. doi: 10.1002/nau.20482.
Blümel JE, Chedraui P, Baron G, Belzares E, Bencosme A, Calle A, et al. Menopausal symptoms appear before the menopause and persist 5 years beyond: a detailed analysis of a multinational study. Climacteric. 2012;15(6):542-551. doi: 10.3109/13697137.2012.658462.
Chen Y, Yu W, Yang Y, Duan J, Xiao Y, Zhang X, et al. Association between overactive bladder and peri-menopause syndrome: a cross-sectional study of female physicians in China. Int Urol Nephrol. 2015;47(5):743-749. doi: 10.1007/s11255-015-0948-6.
Gotoh D, Torimoto K, Takamatsu N, Onishi K, Morizawa Y, Hori S, et al. Intravesical injection of onabotulinumtoxina (Botulinum toxin type A) in Japanese patients with refractory overactive bladder. In Vivo (Brooklyn). 2024;38(3):1332-1337. doi: 10.21873/invivo.13573.
Grishin A., Spaska A., Kayumova L. Correction of overactive bladder with botulinum toxin type A (BONT-A). Toxicon, 2021; 200: 96–101.
Nurkkala M, Salo H, Piltonen T, Sova H, Rossi HR. Efficacy of 100-U Onabotulinumtoxin A treatment in female idiopathic overactive bladder – a prospective follow-up study. Int Urogynecol J. 2025;36(3):685-693. doi: 10.1007/s00192-025-06047-8.
Ivanov M, Ceban E. Role of Botulinum toxin A injections as a salvage therapy for refractory overactive bladder: insights from urodynamic studies. In: Sontea V, Tiginyanu I, Railean S, editors. 6th International Conference on Nanotechnologies and Biomedical Engineering: Proceedings of IFMBE-2023, Sep 20-23, 2023, Chisinau, Moldova. Cham: Springer; 2024. Vol. 2: Biomedical engineering and new technologies for diagnosis, treatment, and rehabilitation. p. 267-277.
Herrewegh A, Marcelissen T, van Koeveringe G, Vrijens D. Overactive bladder ‘symptoms’ or ‘complaints’ in young and elderly patients or healthy volunteers? Continence. 2024;9:101068. https://doi.org/10.1016/j.cont.2024.101068.