

Introduction
Stroke is a leading cause of adult disability worldwide. Beyond motor and speech deficits, stroke survivors frequently develop psychological and cognitive complications that can hinder recovery. Post-stroke depression (PSD) is the most common psychiatric condition after stroke and post-stroke anxiety (PSA) is also prevalent [1]. Recent literature indicates that roughly 30% of stroke survivors experience clinically significant depression, and a similar proportion experience anxiety during the first year. Cognitive impairment after stroke is another major concern: estimates of post-stroke cognitive impairment (PSCI) range from about 40% to as high as 60% of patients, depending on timing and assessment criteria. These post-stroke neuropsychiatric problems are not benign: PSD, in particular, is associated with worse functional outcomes and higher mortality, underscoring the need for monitoring and treatment [2]. Notably, anxiety can be independent of depression and affect rehabilitation engagement, which supports screening separately for both conditions rather than assuming they always co-occur [3]. Likewise, untreated anxiety and cognitive deficits can impede recovery by reducing engagement in therapy and self-care.
Despite their impact, depression and anxiety often go under-recognized in acute stroke settings, and cognitive deficits, especially in milder forms, may be overlooked if formal neuropsychological testing is not performed. The acute phase of stroke (days to weeks post-event) is a critical window when early detection of these issues could allow timely intervention. However, much of the existing data on PSD and PSA prevalence comes from chronic or subacute phases of stroke or heterogeneous populations. Fewer studies have focused specifically on the acute post-stroke hospitalization period. Moreover, prior research in this area from Eastern Europe and low-to-middle income countries is limited, underscoring the need for local data to guide clinical practice.
The aim of the study. In this context, we conducted an original research study to evaluate the prevalence and severity of depression, anxiety, and cognitive impairment in patients with acute ischemic stroke. We hypothesized that a substantial proportion of acute stroke patients would exhibit at least mild to moderate depressive or anxious symptomatology and measurable cognitive deficits even in the early post-stroke phase. By quantifying these issues and characterizing their severity, we aim to highlight the importance of routine mental health and cognitive screening in stroke units. This study also seeks to provide baseline data for our center, which can inform the development of integrated neurorehabilitation strategies addressing both the physical and psychological needs of stroke patients.
Materials and methods
Study design and setting. We performed a cross-sectional observational study at the Institute of Emergency Medicine in Chișinău, Republic of Moldova, in a tertiary care unit. The study was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy, issued on 9 July 2024 and recorded in Minutes No. 41/21 May 2024. All procedures complied with the EU GDPR (Reg. 2016/679) and ICH-GCP guidelines; every member of the research team holds a current GCP certificate. Written informed consent was obtained from each participant or, when applicable, from a legally authorized representative.
We used the officially licensed Romanian versions of the EQ-5D (including its Visual Analogue Scale), CANSAS, PHQ-9, GAD-7, HAM-D, HAM-A and MMSE, all of which have been previously validated in Moldovan clinical populations.
Before enrolment began, the assessors (two psychiatrists and one clinical psychologist) completed a 4-hour calibration workshop led by senior supervisors; inter-rater reliability on 10 pilot cases was excellent (κ ≥ 0.82 for the HAM-D total score). Evaluations were performed at the bedside in a quiet ward room, typically lasting 20-30 min, with rest pauses ad-libitum to minimize fatigue. For patients with reading difficulties, items were read aloud verbatim; scoring followed the manuals without modification.
The study is part of a larger project on post-stroke neuropsychiatric outcomes. Patients were recruited between December 2023 and May 2025. Inclusion criteria were: age ≥18 years, acute ischemic stroke confirmed by clinical evaluation and imaging (CT/MRI), within approximately two weeks of stroke onset. We enrolled consecutive patients admitted for acute ischemic stroke who were medically stable enough to undergo a structured interview and brief cognitive testing. Exclusion criteria included hemorrhagic stroke, transient ischemic attack, severe aphasia, altered level of consciousness, or any condition that precluded informed consent or valid neuropsychological assessment (e.g., pre-stroke dementia or severe psychiatric illness). We ultimately included 99 patients with acute ischemic stroke (referred to as the stroke cohort). Although a control group of patients without stroke was initially planned, it is not included in the present analysis; therefore, no control comparisons are reported.
Assessments. Within 7-14 days post-stroke (median ~10 days), each patient underwent a standardized evaluation by a study physician and psychologist. Demographic and clinical data were recorded, including age, sex, education level, employment status, vascular risk factors (hypertension, diabetes mellitus, etc.), and stroke characteristics. Stroke severity was documented using neurological examination and imaging reports. However, formal stroke severity scores (NIHSS) were not uniformly available for all patients and thus are not reported here. We did note whether the stroke was a first-ever vs. recurrent event.
Depression and anxiety. Depression symptoms were assessed using the Patient Health Questionnaire-9 (PHQ-9), a 9-item self-report scale validated in stroke populations for screening depression severity. PHQ-9 scores range from 0 to 27. We used standard cut-offs to categorize depression severity as minimal (0-4), mild (5-9), moderate (10-14), moderately severe (15-19), or severe (20-27). A PHQ-9 score ≥10 was taken as indicative of at least moderate depression, a threshold commonly used to identify clinically significant depression symptoms requiring follow-up [1]. Anxiety symptoms were measured with the 7-item Generalized Anxiety Disorder scale (GAD-7), similarly categorized into minimal (0-4), mild (5-9), moderate (10-14), and severe (15-21) anxiety; GAD-7 ≥10 was considered positive for moderate-to-severe anxiety. In addition to these self-report instruments, trained clinicians administered the Hamilton Depression Rating Scale (17-item HAM-D) and Hamilton Anxiety Rating Scale (14-item HAM-A) for a subset of patients to corroborate self-reported findings with clinical interview-based ratings. HAM-D scores ≥17 and HAM-A scores ≥18 were defined as moderate or greater symptom severity based on conventional cut-offs.
Cognitive function. Global cognitive status was evaluated using the Mini-Mental State Examination (MMSE). The MMSE assesses orientation, attention, memory, language, and visuoconstructional abilities, with scores ranging from 0 to 30. A score below 24 was used to define cognitive impairment, a widely accepted threshold indicative of at least mild cognitive deficit. Because the MMSE has known ceiling effects and may miss executive dysfunction, we interpreted our cognitive findings cautiously. Patients with severe comprehension deficits or dysphasia who could not complete the MMSE were excluded from cognitive analyses (these largely overlapped with the exclusion criteria mentioned above).
Other measures. Health-related quality of life was documented using the EQ-5D-5L questionnaire (results not the focus of this report). We also recorded any use of psychotropic medications. At the time of evaluation, none of the patients were on antidepressant therapy (baseline “additional treatment (AD)” with antidepressants was recorded; all patients in this acute phase had “No” for current antidepressant use).
Data analysis. Descriptive statistics were used to summarize the cohort’s characteristics and assessment results. Continuous variables (e.g., age, scale scores) are presented as mean ± standard deviation (SD) or median [interquartile range] as appropriate, and categorical variables as counts and percentages. The prevalence of depression, anxiety, and cognitive impairment was calculated as the proportion of patients exceeding the defined cut-off scores (PHQ-9 ≥10, GAD-7 ≥10, MMSE <24, etc.). We constructed a frequency distribution of depression and anxiety severity categories. No imputation was done for missing data; only patients who completed a given assessment were included in that specific analysis. All statistical analyses were performed using SPSS 25 and Python (pandas) for data handling. As this was primarily a descriptive study, no hypothesis testing or regression analyses were performed. However, we did explore correlations between scales (e.g., PHQ-9 and HAM-D) to ensure consistency of findings. The threshold for statistical significance (if any tests were applied post-hoc) was set at p<0.05.
Results
Participant characteristics. A total of 99 acute ischemic stroke patients were included (mean age 64.8 ± 8.1 years, range 41-89; 63.5% male). Table 1 summarizes the key demographic and clinical features of the cohort. Most patients had low to moderate levels of educational attainment, with 74% having completed only primary or secondary education. Additionally, the majority (approximately 58%) were retired at the time of stroke, reflecting the older age distribution of the cohort. Vascular comorbidities were highly prevalent: 88% of patients had a history of hypertension and 33% had type 2 diabetes mellitus. About one-quarter (25%) had experienced a prior stroke before the index event, indicating recurrent stroke in a substantial subset. In terms of stroke localization, most infarcts were in the middle cerebral artery territory. Detailed neuroimaging data will be reported elsewhere. Neurologically, common deficits included hemiparesis, speech impairment (aphasia in 20% mild/moderate, severe aphasia in 5% leading to exclusion from full neuropsychological assessment), and sensory changes. All patients were within 2 weeks post-stroke (median 10 days). At the time of assessment, they were medically stable, however, many were in early stages of rehabilitation. Table 1 provides an overview of patient characteristics and key outcome measures:
Table 1. Baseline characteristics and neuropsychological outcomes of the stroke patient cohort (N=99). | |
Variable | Value* |
Age, years | 64.8 ± 8.1 (range 41–89) |
Sex | Male 54 (63.5%); Female 31 (36.5%) |
Education level: ≤Secondary | 74% (primary 8%, gymnasium 66%) |
Employment status: Retired | 58% (actively employed 28%; unemployed 8%) |
Hypertension (history) | 75 (88%) |
Diabetes mellitus | 28 (33%) |
Previous stroke (recurrent) | 21 (25%) |
PHQ-9 Depression score | 7.2 ± 2.6 (mild average) |
Moderate-to-severe depression | 14 (16%) – PHQ-9 ≥ 10 |
GAD-7 Anxiety score | 9.6 ± 2.9 (mild-to-moderate average) |
Moderate-to-severe anxiety | 36 (42%) – GAD-7 ≥ 10 |
MMSE score | 25.2 ± 4.1 |
Cognitive impairment (MMSE <24) | 22 (26%) |
Note: PHQ-9: Patient Health Questionnaire-9; GAD-7: Generalized Anxiety Disorder-7 scale; MMSE: Mini-Mental State Exam. Percentages for depression, anxiety, and cognitive impairment are based on N=85 with complete data. Patients with severe aphasia or other barriers were unable to complete PHQ-9/GAD-7/MMSE and are excluded from those calculations. *Continuous variables shown as mean ± SD; categorical variables as n (%). Depression, anxiety, and cognitive impairment prevalence are calculated among the 85 patients who completed those assessments. | |
Prevalence of depression. Symptoms of depression were widespread in this cohort, though often of mild intensity. The mean PHQ-9 score was 7.2 ± 2.6, which corresponds to the mild depression range on average. A remarkable 92% of patients scored ≥5 on the PHQ-9 (indicating at least mild depressive symptoms).
Figure 1 illustrates the distribution of depression severity categories, with most patients (75%) falling in the mild range. Cognitive screening revealed a mean MMSE of 25.2 ± 4.1; 26% scored <24, indicating cognitive impairment.
|
Fig. 1 Distribution of depression severity (PHQ-9) among acute ischemic stroke patients (n=85) Note: Bars show the number of patients; values above bars give absolute counts and cohort percentages. Depression was classified as Minimal (0-4), Mild (5-9), Moderate (10-14), Moderately severe (15-19), and Severe (≥20). Most participants (64/85; 75%) reported mild symptoms, 14 patients (16%) fell in the moderate range, and 7 (8%) had minimal symptoms. No patient scored in the moderately severe or severe ranges (≥15) during this acute post-stroke phase, indicating that very marked depressive symptomatology was absent or rare within the first two weeks after stroke. |
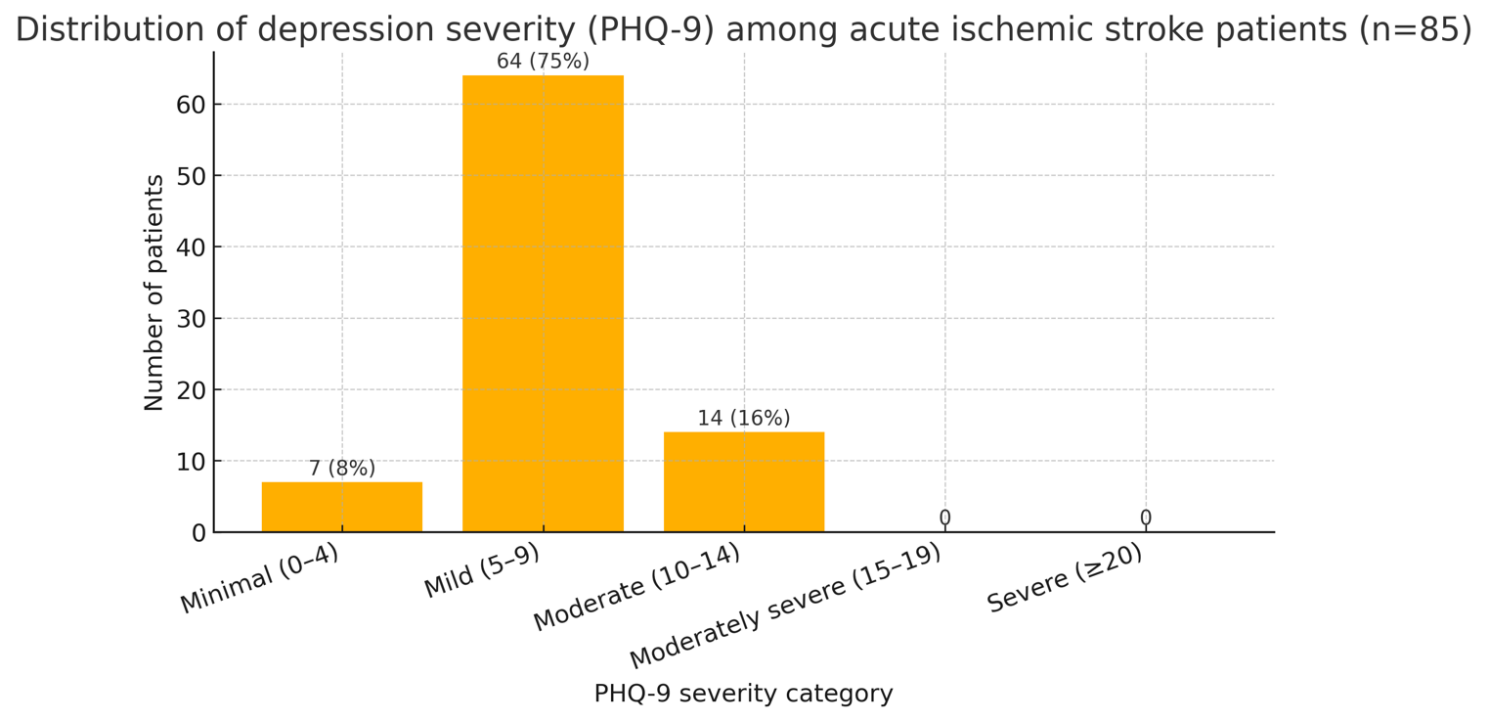
Most patients (75%) reported mild depressive symptoms (PHQ-9 score 5-9). Moderate depression (PHQ-9 10-14) was present in 16% of patients, while none scored in the severe range (≥20) in this acute phase. As shown, the largest proportion fell into the “Mild” category (5-9 points) with 64 patients (75%). Fourteen patients (16% of the sample) had PHQ-9 scores between 10 and 14, indicating moderate depression. Importantly, no patients met criteria for severe depression (PHQ-9 ≥20), and none fell in the 15-19 “moderately severe” range either, suggesting that very severe depressive symptoms were absent or rare shortly after stroke. When considering clinician-rated depression, the HAM-D scale (administered to 85 patients) yielded a mean of 16.0 ± 5.9. According to HAM-D, 30 patients (35% of those assessed) had scores ≥17, consistent with at least moderate depression, including 13 (15%) with severe depression (HAM-D ≥24). The discrepancy between PHQ-9 and HAM-D results (fewer patients endorsing severe symptoms on self-report) might reflect under-reporting or the challenges of self-assessment in acute illness. Nonetheless, using either instrument, we estimate that roughly 15-35% of acute stroke patients in our cohort experienced clinically significant depressive symptoms.
Prevalence of anxiety. Anxiety symptoms were even more prominent. The average GAD-7 score was 9.6 ± 2.9, on the upper end of the mild range (5-9) and nearing moderate. A GAD-7 score ≥10 (moderate or severe anxiety) was recorded in 36 patients, representing 42% of those assessed – a substantial portion. Specifically, 31 patients (36%) had moderate anxiety (GAD-7 10-14) and 5 (6%) had severe anxiety levels (GAD-7 ≥15). Thus, about 4 in 10 acute stroke patients suffered moderate-to-severe anxiety symptoms. Self-reported anxiety was corroborated by clinician ratings: the HAM-A scale mean was 17.3 ± 5.8, and 30 patients (35%) had HAM-A ≥18 (moderate or severe anxiety), of whom 9 (11%) were in the severe range (HAM-A ≥25). Many patients described constant worry about their health, fear of disability, or feelings of tension and restlessness in the hospital. Notably, there was considerable overlap between depression and anxiety: among patients with PHQ-9 ≥10, the majority also had GAD-7 ≥10, and vice versa, consistent with a comorbid depressive-anxiety syndrome. We found that 14% of the total sample had combined moderate depression and anxiety (both PHQ-9 ≥10 and GAD-7 ≥10). However, it was also evident that some patients had significant anxiety without depression (e.g., “worried well” about recovery), which underscores the need to screen for both conditions separately rather than assuming they always co-occur.
Cognitive impairment. On cognitive testing with the MMSE, the cohort’s mean score was 25.2 ± 4.1 (out of 30). Sixty-three patients (74%) scored in the “normal” range (24-30). Meanwhile, 22 patients – representing 26% of those tested – scored below 24, consistent with cognitive impairment. Most of these fell in the mild impairment range (MMSE 18-23); only 3 patients (3.5%) had MMSE <18, indicating moderate-to-severe cognitive impairment. The cognitive domains commonly missed included short-term recall and complex commands, whereas orientation and basic language were relatively preserved in many cases. It should be noted that patients with severe aphasia (≈5% of the original 99) could not be meaningfully tested with MMSE and were excluded from the MMSE analysis, so the true prevalence of cognitive impairment might be slightly underestimated. Nonetheless, about one-quarter of acute ischemic stroke survivors in our sample showed objective evidence of cognitive deficits even at this early stage. This finding aligns with expectations that vascular cognitive impairment can manifest acutely, particularly with strategic infarcts or high vascular risk burden.
Additional findings. Nearly all patients (95%) reported some degree of physical disability or limitation on the EQ-5D, and the mean EQ-5D visual analog scale (patient-rated health state) was 71.5 ± 14.8 (on a 0-100 scale, where 100 represents perfect health), reflecting a moderate self-perceived health status post-stroke. We observed that patients with higher depression/anxiety scores tended to rate their overall health and recovery confidence lower (qualitatively). No significant differences in depression or anxiety prevalence were found between men and women in this sample, although women had a non-significantly higher mean PHQ-9 (by ~1 point). Patients with cognitive impairment (MMSE <24) were slightly older on average than cognitively intact patients (66.3 vs. 64.3 years), but this difference was not statistically significant in our sample. Those with cognitive impairment also tended to have lower education levels (e.g., all patients with ≤4 years of schooling were cognitively impaired) and a higher frequency of prior strokes, suggesting that these factors may contribute to early post-stroke cognitive deficits.
Summary of key outcomes. In summary, within the acute phase of ischemic stroke, about one-third of patients experienced clinically relevant depression or anxiety symptoms, and one-quarter had measurable cognitive impairment. Mild symptoms were extremely common, with only a minority of patients being entirely free of any depressive or anxious symptoms. These results underscore that psychiatric and cognitive sequelae are the rule rather than the exception, even shortly after stroke onset.
Discussion
In this study of acute ischemic stroke patients, we found a high prevalence of affective symptoms and cognitive deficits even in the immediate post-stroke period. To our knowledge, this is one of the first detailed reports from our region quantifying these issues in an acute stroke setting. Our findings are broadly consistent with the international literature, with some nuances specific to the acute post-stroke timeframe.
Comparison with prior studies. The rate of post-stroke depression (PSD) observed in our cohort (approximately 16% with PHQ-9 ≥10 in-hospital and 35% with moderate depression per HAM-D) aligns with the lower end of the range reported in meta-analyses. A 2023 systematic review by Liu et al. noted an overall depression prevalence of around 27% in stroke survivors, with early assessments (within 3 months) yielding ~24-29% depending on the method [1]. Our self-reported depression rate (16%) is slightly lower, possibly because we captured patients within days of stroke when some were still mobilizing coping resources, or because some patients underreported symptoms due to the hospitalization context. In the first two weeks post-stroke, studies have noted a wide range (12-32%) of depression prevalence [4], so our PHQ-9 finding falls within this interval. By contrast, the clinician-rated depression prevalence (HAM-D 35%) was higher, suggesting that clinical interviewing detected depressive signs (e.g., sad affect, sleep disturbance, apathy) that patients did not fully report on questionnaires. This discrepancy highlights the importance of active clinical screening; relying solely on self-report may underestimate PSD immediately post-stroke, when patients might attribute symptoms to stroke recovery rather than depression per se. Nevertheless, by any measure, a substantial subset of our patients had clinically significant depression very early after stroke. This is notable because early-onset PSD is known to often persist and is linked to worse outcomes if not addressed [1]. Known risk factors for PSD include female sex, a prior history of depression, and stroke severity [5].
The prevalence of post-stroke anxiety (PSA) in our study (~40% with GAD-7 ≥10) was high and in line with, or slightly above, prior estimates. Literature on PSA has been less extensive than that on PSD, but a recent narrative review stated that anxiety affects roughly one-third of stroke survivors in the first year [6]. Our acute-phase data suggest that anxiety might even be more common than depression initially. One possible explanation is that hospitalization and uncertainty about recovery may acutely heighten anxiety. Patients often voiced concerns about disability, future strokes, or loss of autonomy, which can drive anxiety symptoms in the hospital. Nelsone and colleagues (2023) found that 17.6% of patients reported anxiety at 3 months and 15.7% at 12 months after a mild to moderate stroke, and these symptoms were significantly associated with poorer perceived recovery, although the study did not cover the acute hospitalization period [7]. A new 2024 meta-analysis focusing on young stroke patients found 39% had anxiety symptoms, almost exactly matching our 42% in a mixed-age cohort. Thus, our findings reinforce that anxiety is a frequent and often under-recognized problem in acute stroke care. Clinicians should be aware that even patients who do not meet full criteria for depression might be experiencing significant anxiety that could benefit from intervention (e.g., counseling, relaxation techniques, or cautious short-term anxiolytic use) [8].
Regarding cognitive impairment, about one-quarter of our patients had MMSE-defined impairment acutely. This is somewhat lower than long-term studies showing ~40-60% of stroke survivors have cognitive deficits when assessed within the first year [9-10]. The lower figure in our study likely reflects two factors: timing and assessment tool sensitivity. First, some cognitive sequelae of stroke may evolve or become more evident over time (for instance, vascular cognitive impairment can worsen due to post-stroke neurodegeneration or the uncovering of pre-existing deficits). Immediately after stroke, certain patients may not yet manifest the full extent of cognitive dysfunction, or they may partially recover cognitive function that was transiently affected (e.g., due to acute encephalopathy or swelling). Indeed, a proportion of early post-stroke cognitive impairment can improve, as suggested by studies in which some patients show cognitive recovery by 3-6 months [11]. Second, the MMSE has limitations in detecting mild executive dysfunction or attention deficits common in vascular cognitive impairment. Tools like the Montreal Cognitive Assessment (MoCA) are more sensitive in stroke cohorts. Had we used MoCA or a detailed neuropsychological battery, we might have identified a higher prevalence of subtle cognitive deficits (particularly in domains like processing speed or executive function). Therefore, our figure of 26% likely represents the more overt cases of cognitive impairment. It is worth noting that all patients with MMSE impairment had either a large cortical stroke or multiple vascular risk factors, aligning with known risk factors for PSCI such as age, low education, diabetes, hypertension, and prior strokes [11]. These risk factors were common in our sample, suggesting our patients remain at risk for further cognitive decline. Follow-up at 6-12 months will be needed to determine whether more patients develop late cognitive impairment or dementia.
Clinical implications of our findings. Our findings carry several important implications for clinical care and stroke rehabilitation. Firstly, the high rates of depression and anxiety in the acute setting underscore the need for routine psychological screening as part of stroke unit care. Brief instruments like the PHQ-9 and GAD-7 can be feasibly integrated into the nursing/neurology assessment protocol. Early identification of PSD/PSA is crucial because these conditions are treatable, and their treatment can meaningfully improve patient outcomes. For example, evidence suggests that treating post-stroke depression can enhance participation in rehabilitation therapies and is associated with better functional recovery [12]. Untreated depression or anxiety, on the other hand, may lead to reduced motivation, poorer engagement with physiotherapy, longer hospital stays, and diminished functional gains [2, 3, 13]. In our setting, we observed informally that patients with moderate-to-severe mood symptoms were often less active in therapy sessions and more likely to refuse or withdraw from some activities, corroborating these concerns. Early involvement of mental health professionals (such as consultation-liaison psychiatrists or clinical psychologists) could help implement supportive counseling, psychoeducation, or pharmacotherapy when appropriate. Interventions such as therapeutic optimism, involving family support, and managing sleep or pain issues can also alleviate depression/anxiety.
Secondly, recognizing cognitive impairment in the acute phase is important for discharge planning and rehabilitation tailoring. Patients with cognitive deficits may struggle with learning new rehabilitation strategies, adhering to safety precautions, or managing medications after discharge. Simple measures, such as providing written instructions, involving caregivers in education, and occupational therapy cognitive training, can mitigate risks. Moreover, early cognitive rehabilitation strategies might improve outcomes; some studies have shown that targeted cognitive training in post-stroke patients can modestly enhance cognitive function and even influence functional recovery. Our data suggest that even mild cognitive impairment was present in one-quarter of patients, so incorporating cognitive evaluation (e.g., MoCA screening before discharge) is advisable for most stroke survivors. This approach will help identify those who may benefit from neuropsychological follow-up or cognitive rehabilitation programs.
Thirdly, the fact that none of our patients were on antidepressants during the acute phase (and few on anxiolytics) reflects a potential gap in care. There is ongoing debate about prophylactic antidepressant use after stroke. Trials like FLAME (fluoxetine for motor recovery) initially suggested that SSRIs might improve motor outcomes, although later, larger trials did not confirm a clear benefit and raised safety concerns (e.g., falls, seizures). Current guidelines do not recommend routine prophylactic antidepressants for all stroke patients, but they do emphasize treating established depression or anxiety. Our hospital has since instituted a policy to have a psychiatrist evaluate any stroke patient who screens positive for depression or anxiety before discharge, to consider treatment. In the context of our study, had we identified major depression in any patient (e.g., PHQ-9 >20 or HAM-D >23, which we did not in this acute sample), initiation of an SSRI would have been strongly considered. For moderate depression/anxiety, options include psychotherapy (even brief CBT-based interventions or guided self-help), in addition to or instead of medications.
Study limitations. Several limitations must be acknowledged. Most importantly, our study lacked a control group of non-stroke patients. This limits our ability to attribute the observed depression and anxiety solely to the stroke event, as opposed to general hospitalization or prior psychiatric history. Nonetheless, the prevalence we observed is much higher than the general population point prevalence of mood disorders for this age group, suggesting a stroke-related effect. Another limitation is the single-center, relatively small sample size. With 99 patients (85 completing all assessments), our estimates, especially for subgroups (e.g., severe depression = 0%), should be interpreted with caution. The study may have been underpowered to detect certain differences (for instance, sex differences or correlations with stroke location). There is also potential selection bias: patients with very severe strokes (e.g., large infarcts causing coma or global aphasia) could not be assessed and were excluded, which might underestimate the true burden of neuropsychiatric complications in all stroke patients. Conversely, patients with minor strokes might have been discharged early and missed; however, given our hospital’s practice, most acute strokes were admitted for at least a few days, so we believe our sample is representative of moderate-to-severe stroke hospitalizations.
Additionally, the assessment tools have inherent limitations. The PHQ-9 and GAD-7, while validated and convenient, are screening tools and not equivalent to a clinical diagnosis. We did not perform structured psychiatric interviews (e.g., SCID) to formally diagnose major depressive disorder or anxiety disorders according to DSM-5 criteria, which means we are reporting “symptom prevalence” rather than diagnosed disorder prevalence. Some patients might have transient adjustment reactions or subclinical symptoms that would not qualify as disorders upon detailed evaluation. However, from a clinical standpoint, even subclinical symptoms can be important to address in stroke recovery. Our reliance on the MMSE for cognition is another limitation – a more detailed cognitive battery would provide richer information on domains such as executive function and could reveal higher impairment rates. We plan to incorporate the MoCA in future assessments.
Finally, this study only captures a cross-sectional snapshot in the acute phase. We do not have longitudinal data in this report to determine how depression, anxiety, or cognition evolve in these patients (though follow-ups at 3 and 12 months are underway in our project). Therefore, we cannot infer the persistence or prognosis of these conditions from our data. Some patients who were not depressed at discharge may develop depression later (post-stroke mood disorders can have delayed onset in a minority of cases), and vice versa. Similarly, cognitive impairment could worsen (due to post-stroke neurodegeneration) or improve (recovery, neuroplasticity) over time. Our acute-phase findings thus underscore an initial high burden, but longitudinal research is needed to inform when and how to intervene most effectively.
Conclusions
This study demonstrates that depression, anxiety, and cognitive impairment are common and consequential in patients hospitalized with acute ischemic stroke. Even within two weeks of stroke onset, about one-third of patients showed clinically meaningful symptoms of depression or anxiety, and one-quarter had cognitive deficits on screening. These figures reinforce that post-stroke neuropsychiatric complications begin early and should be proactively monitored. We found that most patients had at least mild depressive or anxious symptoms, underlining the need for routine psychological support as part of comprehensive stroke care.
Using a brief (20-30 min), structured battery of validated self-report and clinician-rated scales at the bedside in a real-world Moldovan hospital, we showed that such screening is both feasible and valuable, while also providing much-needed data from an Eastern European population often underrepresented in stroke research. The consistency of our results with international literature suggests that they are generalizable to similar clinical settings.
Our findings add to the growing recognition that stroke recovery is not only about physical rehabilitation but also about addressing mental health and cognitive function. Early identification and management of PSD and PSA might improve participation in therapy, functional recovery, and overall quality of life for stroke survivors. We advocate that stroke units implement standard screening for depression, anxiety, and cognition, and establish referral pathways for psychological and cognitive interventions. Future research should explore the efficacy of early interventions (pharmacological or psychotherapeutic) in ameliorating these conditions and whether such treatments translate into better stroke outcomes.
Competing interests
None declared.
Authors’ contribution
MB and RC conceived the study, performed the statistical analysis, and drafted the manuscript. RC, MB, and MaB conducted the data collection. DJ assisted with data management and operational coordination. IN and JC supervised the overall project and coordinated the scientific implementation. JC contributed to the methodological framework and interpretation of findings. LB, AE, AB, and CA assisted with the literature review and critically revised the manuscript. All authors reviewed the work critically and approved the final version of the manuscript.
Informed consent for publication
Obtained.
Ethics approval
The Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy granted ethical approval to the study protocol (Favourable Opinion No. 3, issued on 9 July 2024), as documented in Minutes No. 41 of 21 May 2024, and written informed consent was obtained from each participant or, when applicable, from a legally authorised representative.
Acknowledgements and funding
No funding/conflict of interest were reported.
Authors’ ORCID IDs
Mihaela Belous – https://orcid.org/0000-0002-2597-1060
Radislav Cosulean – https://orcid.org/0000-0001-8699-6862
Dorin Jelaga – https://orcid.org/0009-0004-7761-450X
Madalina Bivol – https://orcid.org/0009-0005-2827-9992
Igor Nastas – https://orcid.org/0000-0001-8751-9101
Jana Chihai– https://orcid.org/0000-0002-7720-5544
Larisa Boronin– https://orcid.org/0000-0001-8180-8711
Andrei Esanu – https://orcid.org/0000-0003-1289-4622
Alina Bologan – https://orcid.org/0000-0002-1771-7476
Cornelia Adeola – https://orcid.org/0009-0002-0728-9196
References
Liu L, Xu M, Marshall IJ, et al. Prevalence and natural history of depression after stroke: A systematic review and meta-analysis of observational studies. PLOS Med. 2023;20(3):e1004200. doi: 10.1371/journal.pmed.1004200.
Ayerbe L, Ayis S, Wolfe CDA, Rudd AG. Natural history, predictors and outcomes of depression after stroke: systematic review and meta-analysis. Br J Psychiatry. 2013;202:14-21. doi: 10.1192/bjp.bp.111.107664.
Lee EH, Kim JW, Kang HJ, Kim SW, Kim JT, Park MS, et al. Association between anxiety and functional outcomes in patients with stroke: a 1-year longitudinal study. Psychiatry Investig. 2019;16(12):919-25. doi: 10.30773/pi.2019.0188.
Butsing N, Zauszniewski JA, Ruksakulpiwat S, Quinn Griffin MT, Niyomyart A. Association between post-stroke depression and functional outcomes: a systematic review. PLoS One. 2024 Aug 22;19(8):e0309158. doi: 10.1371/journal.pone.0309158.
Shi Y, Yang D, Zeng Y, Wu W. Risk factors for post-stroke depression: a meta-analysis. Front Aging Neurosci. 2017;9:218. doi: 10.3389/fnagi.2017.00218.
Chun HYY, Ford A, Kutlubaev MA, Almeida OP, Mead GE. Depression, anxiety, and suicide after stroke: a narrative review of the best available evidence. Stroke. 2022 Apr;53(4):1402–1410. doi: 10.1161/STROKEAHA.121.035499.
Nelsone L, Rafsten L, Abzhandadze T, Sunnerhagen KS. A cohort study on anxiety and perceived recovery 3 and 12 months after mild to moderate stroke. Front Neurol. 2023;14:1273864. doi: 10.3389/fneur.2023.1273864.
Ignacio KHD, Muir RT, Diestro JDB, Singh N, Yu MHLL, Omari OE, et al. Prevalence of depression and anxiety symptoms after stroke in young adults: a systematic review and meta-analysis. J Stroke Cerebrovasc Dis. 2024;33(7):107732. doi: 10.1016/j.jstrokecerebrovasdis.2024.107732.
Ma Y, Yang Y, Wang X, et al. Prevalence and risk factors of poststroke cognitive impairment: a systematic review and meta-analysis. Public Health Nurs. 2025;42(2):1047-1059. doi: 10.1111/phn.13503.
Mtambo ML, Ragunathan T, Mohan D, Warren N, Su TT, Quek KF. Post-stroke cognitive impairment and dementia research in Southeast Asia: a scoping review. Asian J Psychiatr. 2025;107:104460. https://doi.org/10.1016/j.ajp.2025.104460.
El Husseini N, Katzan IL, Rost NS, Blake ML, Byun E, Pendlebury ST, et al. Cognitive impairment after ischemic and hemorrhagic stroke: a scientific statement from the American Heart Association/American Stroke Association. Stroke. 2023;54(6):e272-e291. doi: 10.1161/STR.0000000000000430.
Towfighi A, Ovbiagele B, El Husseini N, et al. Poststroke depression: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2017;48(2):e30-e43. doi: 10.1161/STR.0000000000000113.
Butsing N, Zauszniewski JA, Ruksakulpiwat S, Griffin MTQ, Niyomyart A. Association between post-stroke depression and functional outcomes: a systematic review. PLoS ONE. 2024;19(8):e0309158. doi: 10.1371/journal.pone.0309158.