
Introduction
Juvenile idiopathic arthritis (JIA), as defined by the International League of Associations for Rheumatology (ILAR) refers to a persistent type of arthritis with no defined cause, beginning before the age of 16 years and lasting for at least 6 weeks [1]. JIA is the most common rheumatic disease in children, and can significantly impair joint function, leading to joint deformities, growth failure and persistent active disease into adulthood. The disease is characterized by chronic synovial inflammation, cartilage damage, and bone erosion.
Chronic inflammatory diseases such as JIA pose a major risk of premature coronary heart disease. Dyslipidemia plays a crucial role in atherosclerosis, a condition that might be associated with autoimmune diseases. The risk of developing atherosclerosis increases gradually with rising levels of total cholesterol and triglycerides [2].
Cardiovascular risk factors undergo changes during periods of growth and development. Body mass index, systolic and diastolic blood pressure, and serum concentrations of total cholesterol and triglycerides were strongly associated with the extent of lesions in the aorta and coronary arteries [3].
Disturbances in the traditional lipid profile are considered to be associated with subclinical atherosclerosis [4].Top of Form
Dyslipidemia, which is defined by an increase in total cholesterol and/or triglycerides, is one of the most well-known risk factors in children with JIA. Consequently, increased disease activity is associated with dyslipidemia in children with JIA [5, 6]. The impact of cholesterol on atherogenesis is well-documented, playing a central role in triggering the process [7].
Patients with JIA have an increased risk of developing changes in their lipid profile in comparison to those without arthritis. As a result, adults with a history of JIA during childhood have a 6-fold increased risk of developing subclinical atherosclerosis, ultimately leading to an increased risk of cardiovascular disease over time [2]. Hence, continuous monitoring of the lipid profile could potentially reduce morbidity and mortality among adult patients [8]. In patients with rheumatoid arthritis (RA), the prevalence of dyslipidemia varies between 55% and 65% [6, 9-12].
The pathogenesis of dyslipidemia and cardiovascular risk in patients with JIA has not been fully elucidated. Cholesterol plays a crucial role in triggering endothelial dysfunction by activating endothelial and muscle cells, as well as secreting inflammatory mediators such as proinflammatory cytokines [13-14].
Although hypercholesterolemia is significant in approximately 50% of patients with cardiovascular disease, it is crucial to consider other contributing factors as well [15]. Atherosclerosis is undoubtedly an inflammatory disease and does not solely result from lipid accumulation.
Homocysteine (Hcy) is a sulfur-containing amino acid derived from the essential amino acid methionine during its conversion to cysteine [16-18]. Its plasma concentration depends on various factors such as age, sex, lifestyle (including coffee consumption, smoking, physical activity, and alcoholconsumption), genetic mutations that result insignificantly reduced activity of the enzymes involved in homocysteine catabolism, medications, and diseases that interfere with its metabolism. The most significant factor influencing homocysteine levels is the intake of B vitamins [16-19]. For instance, decreased folate concentrations can lead to hyperhomocysteinemia, which is defined by plasma homocysteine concentrations ≥ 15 μM [20].
Hyperhomocysteinemia (HHcy) is a well-known cardiovascular risk factor both in the general population and in patients with inflammatory conditions [18, 21-23]. Considering the cardiovascular risk associated with RA and chronic systemic inflammation, it is essential to implement anti-inflammatory strategies, as well as interventions aimed at lowering homocysteine levels, in this patient population.
Throughout life, serum homocysteine levels gradually increase until puberty. Normal values of serum homocysteine in children and adolescents range from 5 to 15 µmol/L. During puberty, the serum level of homocysteine typically falls within the range of 6 to7 µmol/L; while in adulthood, it varies between 10 and 11 µmol/L. Hyperhomocysteinemia is defined as serum homocysteine levels exceeding 12-15 µmol/L, with the following grades distinguished: mild (15-30 µmol/L), moderate (30-100 µmol/L), and severe (> 100 µmol/L) [16, 24-25].
Mild hyperhomocysteinemia is often detected in healthy, asymptomatic individuals as well [21, 26].
Elevated serum homocysteine levels contribute to endothelial dysfunction and promote platelet aggregation. This initiates an inflammatory response that directly contributes to the development of atherosclerosis, establishing homocysteine as an independent risk factor in the initiation of atherosclerotic processes. Therefore, circulating homocysteine is considered a sensitive marker associated with inflammation and endothelial dysfunction [7, 21, 27-30].
Currently, there is a lack of data on the effectiveness of homocysteine-lowering strategies for cardiovascular disease (CVD) prevention in this population. However, almost all prospective studies have clearly demonstrated a reduction in morbidity and mortality attributed to methotrexate treatment, partially due to folic acid supplementation reducing methotrexate-induced HHcy [31].
It is worth mentioning that patients with RA have a 60% increased risk of death from myocardial infarction and stroke compared to the general population, along with a 48% increased risk of incident myocardial infarction [32]. Therefore, homocysteine-lowering strategies might be suitable for reducing CVD risk in RA populations.
Homocysteine (Hcy) plays a primary role in the onset of early endothelial dysfunction. It participates in the oxidation process of low-density lipoproteins, the proliferation of smooth muscle cells, and the activation of platelets. Elevated Hcy concentrations in both children and adults have direct and indirect toxic effects on the vascular endothelium, posingan additional risk factor for cardiovascular damage and early cerebrovascular accidents, especially when associated with other risk factors such as hypercholesterolemia [4].
Children with chronic rheumatic diseases exhibit an increased prevalence of accelerated atherosclerosis in adulthood. Therefore, it is crucial to identify childhood risk factors to prevent cardiovascular manifestations in adulthood [33].
The aim of the study was to evaluate certain cardiovascular risk factors (homocysteine, total cholesterol, and triglycerides) in juvenile idiopathic arthritis.
Material and methods
A prospective clinical study was conducted at the Rheumatology Department of the Mother and Child Institute, Chisinau, Republic of Moldova, between 2014 and 2019. The study aimed to evaluate cardiovascular risk factors in children diagnosed with juvenile idiopathic arthritis (JIA). The project was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes №49, dated June 8, 2015), and written informed consent was provided by parents or guardians of all participants.
Study population. The study enrolled a total of 215 children, including 90 children diagnosed with JIA (Group 1 – study group) and 125 healthy controls (Group 2 – control group). Diagnosis of JIA was established according to the classification criteria adopted by the International League of Associations for Rheumatology (ILAR, 1997).
Data collection and clinical assessment
Clinical evaluation included:
Number of painful joints (NPJ),
Number of swollen joints (NSJ),
Physician Global Assessment (PhGA) and Patient Global Assessment (PGA),
Physical function assessed using the Childhood Health Assessment Questionnaire (CHAQ), a validated tool comprising 13 items recommended by the American College of Rheumatology.
Disease activity was further quantified using the Disease Activity Score in 28 joints (DAS28).
Laboratory assessments
Paraclinical investigations included:
Complete blood count,
Acute-phase inflammatory markers: erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP),
Biochemical analysis of homocysteine, total cholesterol (TC), triglycerides (TG), and total lipids.
Blood samples were collected in the morning following an overnight fast. Homocysteine was measured using enzymatic ELISA techniques from plasma obtained after centrifugation within 30 minutes of collection (EDTA tubes used). Total lipids, cholesterol, and triglycerides were quantified enzymatically by spectrophotometry (cholesterol oxidase/peroxidase method) using the Cobas C 311 biochemical analyzer.
Reference pathological values were defined as:
Total cholesterol ≥ 5.2 mmol/L,
Triglycerides > 1.7 mmol/L,
Homocysteine > 12 μmol/L.
Statistical analysis. Data were processed and analyzed using IBM SPSS Statistics version 20 and Microsoft Excel 2010. Qualitative variables were summarized in contingency tables, and associations were tested by the Chi-square (χ²) test. The Student's t-test was applied for comparison of means between two groups, while analysis of variance (ANOVA) was used for comparisons involving three or more groups. Correlations between quantitative variables (e.g., anthropometric, hemodynamic, biochemical, and ultrasound parameters) were evaluated using Pearson’s correlation coefficient (r), interpreted according to Hopkins’ scale:
r < 0.1: negligible correlation,
0.1 ≤ r < 0.7: moderate correlation,
0.7 ≤ r < 0.9: strong correlation,
r ≥ 0.9: very strong/almost perfect correlation.
Statistical significance was set at p < 0.05, with further gradations for high significance (p < 0.01 and p < 0.001).
Risk assessment. Relative risk (RR) and odds ratio (OR) were calculated to estimate the association between JIA and cardiovascular risk factors, specifically hyperhomocysteinemia, hypercholesterolemia, and hypertriglyceridemia.
The RR was computed based on the 2x2 contingency table:
| Outcome+ | Outcome- | Total |
Exposed (JIA) | a | b | a+b |
Unexposed | c | d | c+d |
Risk in exposed (JIA) group: P1 = a/a+b
Risk in unexposed (control) group: P0 =c/c+d
Relative Risk (RR): RR=P1/P10=a/a+b/c/c+d= a(c+d)/ c(a+b)
Confidence intervals (CI) for the relative risk (RR) were calculated using the formula:
CI=RR×(1±z⋅SE)
where:
- RR= relative risk,
- z=1.96 for 95% confidence,
- SE = standard error of the RR, which was derived from the chi-square distribution or 2×2 table counts.
Interpretation criteria were:
RR > 1 with CI excluding 1 indicates a positive association (risk factor),
RR = 1 suggests no effect,
RR < 1 with CI excluding 1 indicates a protective factor,
If CI includes 1, the factor is considered indifferent.
Odds ratios were interpreted as follows:
OR ≈ 1 indicates no association,
OR > 1 indicates a positive correlation, suggesting causality,
OR < 1 indicates a protective effect.
The required sample size was calculated using the formula incorporating expected prevalence rates (Po = 45% from literature, P1 = 80% anticipated in study), power (90%), significance level (95%), and an estimated 10% attrition rate.
Results
Participant demographics. The study population of children with juvenile idiopathic arthritis (JIA) was stratified by age and gender to better characterize the sample distribution. Among the 90 children with JIA, the following distribution was observed:
Ages 6-8 years: 2 girls (4.4%) and 3 boys (6.6%),
Ages 9-11 years: 4 girls (9%) and 4 boys (9%),
Ages 12-17 years: 24 girls (53.3%) and 8 boys (17.7%).
This indicates a higher prevalence of older girls (12-17 years) in the JIA cohort, consistent with known gender and age patterns in autoimmune diseases, where adolescent females are often more affected.
Dyslipidemia as a cardiovascular risk factor in JIA. Dyslipidemia, characterized by abnormalities in lipid metabolism, is a well-recognized cardiovascular risk factor and was assessed through comprehensive lipid profiling (lipidogram) in all participants. The lipidogram included measurements of total cholesterol (TC) and triglycerides (TG), performed on both the JIA group (n = 90) and the control group (n = 125).
Total cholesterol levels. Children diagnosed with JIA exhibited significantly elevated total cholesterol levels compared to control group:
The mean total cholesterol concentration in the JIA group was 5.3 ± 0.11 mmol/L, with values ranging from 3.2 mmol/L to 7.9 mmol/L.
In contrast, the control group had a mean total cholesterol level of 4.7 ± 0.05 mmol/L, with a range of 3.47 mmol/L to 6.10 mmol/L.
The difference between these groups was statistically significant (F = 28.286, p < 0.001), indicating that children with JIA have a higher burden of hypercholesterolemia. The threshold for elevated cholesterol was set at >5.2 mmol/L, consistent with clinical guidelines for cardiovascular risk.
Triglyceride levels. In contrast to total cholesterol, no statistically significant difference was observed in triglyceride levels between children with JIA and the control group:
The mean triglyceride level in the JIA group was 1.38 ± 0.05 mmol/L, with individual values ranging from 0.57 mmol/L to 3.97 mmol/L.
The control group had a mean triglyceride level of 1.41 ± 0.02 mmol/L, ranging from 0.75 mmol/L to 2.15 mmol/L (Tab.1).
Statistical analysis yielded a non-significant p-value (p > 0.05), indicating comparable triglyceride levels between the two groups.
Table 1. Mean lipidogram values in children with JIA (group 1), compared to the control group (group 2) | ||||||
Indices
| Group 1 (90 children) | Group 2 (125 children) | F | p | ||
Mean value ± SD | Variation intervals | Mean value ± SD | Variation intervals | |||
Total cholesterol, mmol/l | 5.34 ± 0.11 | 3.20-7.90 | 4.70 ± 0.05 | 3.47-6.10 | 28.286 | <0.001** |
Triglycerides, mmol/l | 1.38 ± 0.05 | 0.57-3.97 | 1.41 ± 0.02 | 0.75 – 2.15 | 0.169 | > 0.05 |
Note: JIA – Juvenile Idiopathic Arthritis, Values are presented as mean ± standard deviation for numerical data; SD – standard deviation; **- p<0.001 – considered significant; p>0.05 – considered insignificant | ||||||
These findings suggest that total cholesterol, but not triglycerides, is significantly elevated in children with JIA compared to healthy peers, highlighting hypercholesterolemia as an important cardiovascular risk factor in this population. This elevation may contribute to the increased cardiovascular morbidity associated with chronic inflammation in JIA, necessitating regular lipid monitoring and early interventions targeting cholesterol management.
The prevalence of hypercholesterolemia was significantly higher in in children with JIA than in the control group: 58 children (64.4%) vs. 36 children (28.8%), χ2 = 27.019, gl = 1, p<0.001 (Fig.1).
Increased TG values (TG > 1.9 mmol/l) were observed in 13 children (14.4%) from the JIA group and in 9 children (7.2%) from the control group (p > 0.05).
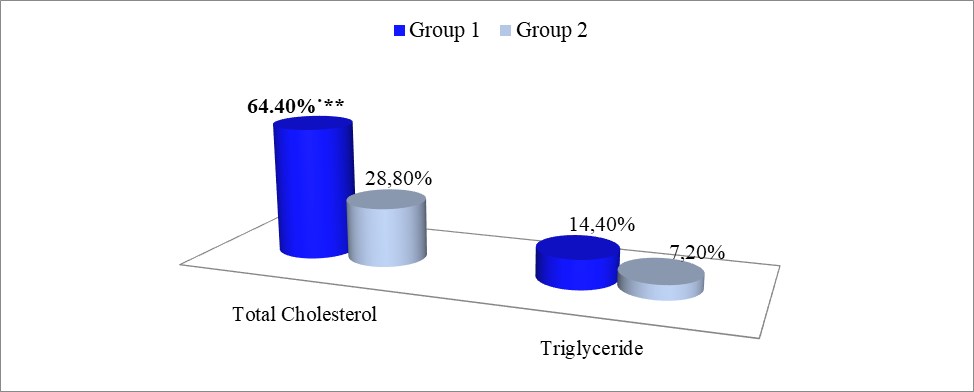 |
Fig. 1 Lipidogram results in children with JIA compared to the control group Note: JIA – Juvenile Idiopathic Arthritis Group 1 – children with juvenile idiopathic arthritis; Group 2 – children from the control group; **- p<0.01, statistically significant value |
Approximately 50% of patients with cardiovascular disease exhibit hyperhomocysteinemia [37]. Therefore, the study aimed to analyze homocysteine as a non-traditional cardiovascular risk factor. Hcy levels were assessed in 90 children with JIA and in 95 children from the control group. The mean value of hyperhomocysteinemia in children with JIA was 14.69 ± 0.61 mmol/l (minimum value – 2.50 mmol/l, maximum value – 29.50 mmol/l) and 9.43 ± 0.29 mmol/l (minimum value – 2.50 mmol/l, maximum value – 16.20 mmol/l) in control group (Tab. 2).
Table 2. Mean values of homocysteine in children with JIA compared to the control group | ||||||
Parameter | Group 1 (90 children) | Group 2 (95 children) | F | p | ||
Mean value ± SD | Variation intervals | Mean value ± SD | Variation intervals | |||
Homocysteine, mmol/l | 14.69 ± 0.61
| 2.50-29.50 | 9.43 ± 0.29 | 2.50-16.20 | 61.889 | < 0.001** |
Note: JIA – Juvenile Idiopathic Arthritis, values are presented as mean ± standard deviation for numerical data; ** - p<0.01, considered statistically significant; SD – standard deviation; Group 1 – children with juvenile idiopathic arthritis; Group 2 – children from the control group | ||||||
In children with JIA, significantly increased values of homocysteine (Hcy > 12 mmol/l) were found in 61 children (67.7%), compared to only in 15 children (15.78%) from the control group (where χ2 = 51.328, gl = 1, p< 0.001).
Among the children included in the study, hyperhomocysteinemia was observed in 67.8% of cases (61 children), with 40 (65.6%) being girls and 21 (34.4%) being boys, compared to 32.2% of cases (29 children) with normal homocysteine values (Fig. 2).
Following this analysis, it can be concluded that patients with JIA exhibit an increased risk of hyperhomocysteinemia compared to the control group.
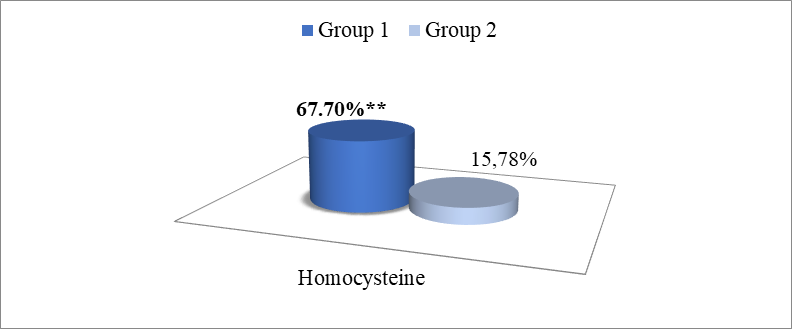 |
Fig. 2 Comparative analysis of homocysteine in children with JIA and the control group Note: JIA – Juvenile Idiopathic Arthritis, Group 1 – children with juvenile idiopathic arthritis; Group 2 – children from the control group; ** - p<0.001, statistically significant value |
The relative risk (RR) was calculated for the following parameters: homocysteine, total cholesterol, and triglycerides, using the "2x2 Table" and calculating the required indicators with the interpretation of the obtained results.
According to the study results, a relative risk (RR) of 3.0 was obtained. When the relative risk has values greater than 1, it indicates a correlation between the risk factor and the occurrence of the disease. This suggests that the risk factor could be a cause of the disease onset in those exposed rather than in unexposed individuals. Therefore, it can be concluded that patients with juvenile idiopathic arthritis have a threefold increased risk of hyperhomocysteinemia compared to subjects in the control group (Tab. 3).
It was also essential to calculate the Odds Ratio (OR) between the rate of disease in those exposed (children with JIA) and the rate of disease in unexposed ones (healthy children). In this case, OR was 11.2, indicating that children's exposure to JIA influences hyperhomocysteinemia. An OR value significantly greater than 1 suggests a strong association between the exposure and the outcome.
Table 3. Assessment of the risk of hyperhomocysteinemia in children with JIA compared to unexposed children | |||
| Children with JIA | Children from the control group | Total |
Exposed | 61 | 15 | 76 |
Unexposed | 29 | 80 | 109 |
Total | 90 | 95 | 185 |
Note: JIA – Juvenile Idiopathic Arthritis, exposed, unexposed, increased risk identified | |||
The relative risk (RR) was also calculated for hypercholesterolemia. Based on the obtained results, patients with JIA, have a 2.3-fold increased risk of developing hypercholesterolemia compared to the unexposed ones (RR = 2.3).
The Odds Ratio (OR) between the odds of disease in exposed children (JIA patients) and the odds of disease in unexposed individuals was found to be 4.5. Thus, it can be concluded that children's exposure to JIA influences the increase in total cholesterol (hypercholesterolemia), showing a moderate correlation trend between them (Tab. 4).
Table 4. Assessment of the relative risk of hypercholesterolemia in children with JIA vs. unexposed children. | |||
| Children with JIA | Children from the control group | Total |
Exposed | 58 | 36 | 94 |
Unexposed | 32 | 89 | 121 |
Total | 90 | 125 | 215 |
Note: JIA – Juvenile Idiopathic Arthritis, exposed, unexposed, increased risk identified | |||
The relative risk (RR) was also calculated for hypertriglyceridemia for the exposed subjects (children with JIA) and unexposed subjects (control group). The calculations yielded a relative risk of 1.5, indicating that patients with JIA have a relatively low risk of developing hypertriglyceridemia compared to unexposed subjects. However, there is a slight trend of correlation between JIA and increased triglyceride values.
Furthermore, similar results were also obtained after calculating the Odds Ratio between the rate of disease in exposed children (JIA patients) and the rate of disease in unexposed individuals, where the Odds Ratio was found to be 4.5. Thus, it can be concluded that children’s exposure to JIA slightly influences the increase in triglycerides (hypertriglyceridemia), showing a slight correlation tendency between them (Tab. 5).
Table 5. The relative risk of hypertriglyceridemia in children with JIA versus unexposed children | |||
| Children with JIA | Children from the control group | Total |
Exposed | 13 | 9 | 22 |
Unexposed | 77 | 115 | 192 |
Total | 90 | 124 | 214 |
Note: JIA – JIA – Juvenile Idiopathic Arthritis, exposed, unexposed, slight correlation | |||
Discussion
The present study contributes to the growing body of evidence indicating that children with juvenile idiopathic arthritis (JIA) may present with dysregulation of lipid metabolism. Our results demonstrated elevated levels of total cholesterol (TC) and a trend toward increased triglycerides (TG) in JIA patients compared to healthy controls. These findings are consistent with previous studies, such as those by Urban et al. [34] and Goncalves et al. [27], which also reported increased concentrations of TC and TG in children with JIA at disease onset. These alterations in lipid profile occurred despite the absence of clinical signs of obesity, suggesting that systemic inflammation may independently influence lipid metabolism in pediatric rheumatic diseases.
Conversely, not all studies have reported consistent findings. Bakkaloglu et al. [35] identified elevated TC levels without a corresponding increase in TG, while Maher et al. [11] did not observe significant lipid abnormalities in JIA patients. These discrepancies could be attributed to heterogeneity in study populations, disease duration, treatment regimens, or methodological differences. Moreover, Semb et al. and Skare et al. [36, 37] reported that lipid profile changes may be modulated by disease activity, highlighting the importance of considering inflammatory status when interpreting metabolic parameters.
The study also assessed plasma homocysteine (Hcy) levels, given the well-documented role of hyperhomocysteinemia as an independent cardiovascular risk factor. Our findings revealed elevated Hcy levels in children with JIA compared to controls, supporting earlier observations by Huemer et al. [31]. Elevated plasma Hcy concentrations have been associated with endothelial dysfunction, smooth muscle cell proliferation, oxidative stress, and thrombogenesis – all of which contribute to the pathogenesis of atherosclerosis [25, 38]. Meta-analyses have shown that a 5 μmol/L increase in plasma Hcy may result in a 60-80% increased risk of coronary heart disease [39, 40].
Despite the clear association between Hcy and cardiovascular risk in adults, its relevance in pediatric autoimmune diseases remains under investigation. In our study, no significant correlations were found between Hcy and inflammatory markers, disease activity, or lipid parameters – findings that align with those of Goncalves et al. [27] and Friso et al. [41]. However, other studies have reported differing associations; for instance, Chiang et al. [42] found a positive correlation between erythrocyte sedimentation rate (ESR) and Hcy, while Annan et al. [43] reported an association between Hcy and TG, but not TC. These inconsistencies underscore the multifactorial etiology of hyperhomocysteinemia, which is influenced by genetic predisposition (e.g., MTHFR polymorphisms), drug therapy (notably methotrexate), diet, and systemic inflammation [18, 32].
Treatment with methotrexate (MTX), a cornerstone in JIA management, has been implicated in elevated Hcy levels. Van Ede et al. [44] demonstrated that MTX therapy may increase plasma Hcy concentrations, and Goncalves et al. [27] observed elevated Hcy in four out of five children undergoing MTX treatment. These findings raise important considerations regarding the balance between therapeutic efficacy and cardiovascular risk, especially in long-term treatment regimens.
While some studies suggest that hyperhomocysteinemia may be a consequence of chronic inflammation, others propose that it may actively contribute to the inflammatory process [45, 46]. This bidirectional relationship could account for the complex and often contradictory findings in the literature. Furthermore, the role of exogenous factors such as reduced mobility, nutritional deficiencies, and prolonged disease course cannot be overlooked.
Importantly, several interventional studies have demonstrated that folic acid supplementation can effectively reduce plasma Hcy levels and improve endothelial function in patients with hyperhomocysteinemia [47, 48]. This positions folic acid as a potential preventive strategy in JIA patients at elevated cardiovascular risk, although large-scale, longitudinal trials are required to establish definitive clinical guidelines.
This study has several limitations that should be acknowledged. First, its cross-sectional design precludes conclusions regarding causality or temporal relationships between inflammation, lipid metabolism, and homocysteine levels. Second, genetic factors such as MTHFR polymorphisms were not assessed, which may influence individual susceptibility to hyperhomocysteinemia. Third, dietary intake, physical activity, and nutritional status were not controlled, potentially introducing confounding variables. Furthermore, the sample size may have limited the statistical power to detect subtle associations or stratify findings by disease subtype or treatment exposure.
Future research should aim to address these limitations through well-designed, multicenter, longitudinal studies that include genetic profiling, dietary assessments, and standardized disease activity scores. Investigations into the impact of folic acid and vitamin B supplementation on cardiovascular markers in JIA are also warranted. Additionally, advanced imaging techniques, such as carotid intima-media thickness and endothelial function testing, may offer further insight into the subclinical cardiovascular changes associated with hyperhomocysteinemia and dyslipidemia in this population.
The present study adds to the growing evidence that children with JIA are at increased risk for metabolic alterations, including dyslipidemia and hyperhomocysteinemia, which may contribute to long-term cardiovascular morbidity. Although some inconsistencies exist in the literature, the findings support the need for early cardiovascular risk assessment and consideration of nutritional interventions. Further research is needed to clarify the mechanisms linking chronic inflammation, homocysteine metabolism, and lipid abnormalities, and to develop evidence-based strategies for cardiovascular risk reduction in pediatric rheumatology.
Conclusions
This study reinforces the association between juvenile idiopathic arthritis (JIA) and alterations in lipid metabolism and homocysteine levels, underscoring the potential cardiovascular risk in affected children. While variability exists across published findings, our results support the hypothesis that systemic inflammation and treatment-related factors may contribute to metabolic disturbances in JIA. The added value of this research lies in its integrated evaluation of both lipid profile and homocysteine levels in a pediatric inflammatory context, highlighting the importance of early cardiovascular risk assessment and the need for tailored preventive strategies in clinical practice.
Competing interests
None declared.
Authors’ contributions
LB was responsible for data collection, questionnaire administration, and statistical analysis. AC contributed to data collection and manuscript drafting. NR served as the project coordinator and supervised the overall research. All authors read and approved the final manuscript.
Ethics approval
The research project was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes no. 49 from 08.06.2015).
Patient consent
Obtained.
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer reviewed.
Authors’ ORCID IDs
Livia Bogonovschi – https://orcid.org/0000-0001-9713-5566
Angela Cracea – https://orcid.org/0000-0002-5283-1178
Ninel Revenco – https://orcid.org/0000-0002-5229-7841
References
Thomson W, Barrett JH, Donn R, et al. Juvenile idiopathic arthritis classified by the ILAR criteria: HLA associations in UK patients. Rheumatology (Oxford). 2002;41(10):1183-1189. doi: 10.1093/rheumatology/41.10.1183.
Sule S, Fontaine K. Metabolic syndrome in adults with a history of juvenile arthritis. Open Access Rheumatol. 2018;10:67-72. doi: 10.2147/OARRR.S157229.
Aranda-Valera IC, De la Rosa IA, Roldán-Molina R, et al. Subclinical cardiovascular risk signs in adults with juvenile idiopathic arthritis in sustained remission. Paediatr Rheumatol. 2020;18:1-12. doi: 10.1186/s12969-020-00448-3.
Momin M, Jia J, Fan F, et al. Relationship between plasma homocysteine level and lipid profiles in a community-based Chinese population. Lipids Health Dis. 2017;16:54. doi: 10.1186/s12944-017-0441-6.
Del Giudice E, Dilillo A, Tromba L, et al. Aortic, carotid intima-media thickness and flow- mediated dilation as markers of early atherosclerosis in a cohort of paediatric patients with rheumatic diseases. Clin Rheumatol. 2018;37(6):1675-1682. doi: 10.1007/s10067-017-3705-7.
Boyer JF, Bongard V, Cantagrel A, et al. Link between traditional cardiovascular risk factors and inflammation in patients with early arthritis: results from a French multicentre cohort. Arthritis Care Res (Hoboken). 2012;64(6):872-880. doi: 10.1002/acr.21623.
Panfile E, Ivanov V, Ştirbul A. Ateroscleroza şi procesul inflamator imun [Atherosclerosis and the immune inflammatory process]. Bull Acad Sci Mold. Med Sci. 2010;(2):132-136. Romanian.
Toms TE, Panoulas VF, Douglas KMJ, et al. Are lipid ratios less susceptible to change with systemic inflammation than individual lipid components in patients with rheumatoid arthritis? Angiology. 2011;62(2):167-175. doi: 10.1177/0003319710373749.
Ahmed S, Jacob B, Carsons SE, et al. Treatment of cardiovascular disease in rheumatoid arthritis: a complex challenge with increased atherosclerotic risk. Pharmaceuticals (Basel). 2021;15(1):11. doi: 10.3390/ph15010011.
Liao KP, Solomon DH. Inflammation, disease-modifying antirheumatic drugs, lipids, and cardiovascular risk in rheumatoid arthritis. Arthritis Rheumatol. 2015;67(2):327-329. doi: 10.1002/art.38925.
Maher SE, Abdel Raheem M, Moness HM. Subclinical atherosclerosis in children with rheumatologic diseases in Minia Children University Hospital, Egypt. Int J Pediatr. 2019;7(3):9159-9167. https://doi.org/10.22038/ijp.2018.36402.3174.
Liao KP, Cai T, Gainer VS, et al. Lipid and lipoprotein levels and trend in rheumatoid arthritis compared to the general population. Arthritis Care Res (Hoboken). 2013;65(12):2046-2050. doi: 10.1002/acr.22091.
Liao KP, Liu J, Lu B, et al. Association between lipid levels and major adverse cardiovascular events in rheumatoid arthritis compared to non-rheumatoid arthritis patients. Arthritis Rheumatol. 2015;67(8):2004-2010. doi: 10.1002/art.39165.
Marangoni RG, Hayata AL, Borba EF, et al. Decreased high-density lipoprotein cholesterol levels in polyarticular juvenile idiopathic arthritis. Clinics. 2011;66(9):1549-52. doi: 10.1590/s1807-59322011000900007.
Zota I, Lîsîi L, Munteanu A. Corelaţia patogenetică între sindromul metabolic şi ateroscleroza [Pathogenetic correlation between metabolic syndrome and atherosclerosis]. In: Scientific Annals of Nicolae Testemițanu SUMPh. Chisinau; 2009. Vol. 1. p. 41-48. Romanian.
Alam MF, Islam MM, Haque M, et al. Serum homocysteine level in children with Juvenile Idiopathic Arthritis. Bangladesh Med Res Counc Bull. 2020;46:12-16. doi: 10.3329/bmrcb.v46i1.47463
Anestiadi V, Zota E, Groppa S, et al. Unele aspecte în patogenia aterosclerozei [Some aspects in the pathogenesis of atherosclerosis]. Bull Acad Sci Mold. Med Sci. 2005;(2):37-43. Romanian.
Ganguly P, Alam SF. Role of homocysteine in the development of cardiovascular disease. Nutr J. 2015;14:6. doi: 10.1186/1475-2891-14-6.
McCully KS. Homocysteine, vitamins, and vascular disease prevention. Am J Clin Nutr. 2007;86(5):1563-1568. doi: 10.1093/ajcn/86.5.1563S.
Bivol D. Afectarea sistemului cardiovascular la pacienții cu artrită reumatoidă = Cardiovascular disease in rheumatoid arthritis pacients. In: Scientific abstracts of students, residents and young researchers of Nicolae Testemițanu SUMPh. Chisinau: Medicina; 2018. p. 126.
Holven KB, Aukrust P, Retterstol K, et al. Increased levels of C-reactive protein and interleukin-6 in hyperhomocysteinemic subjects. Scand J Clin Lab Invest. 2006;66(1):45-54. doi: 10.1080/00335510500429821.
Du Plessis JP, Nienaber-Rousseau C, Lammertyn L, et al. The relationship of circulating homocysteine with fibrinogen, blood pressure, and other cardiovascular measures in African adolescents. J Pediatr. 2021;234:158-163. doi: 10.1016/j.jpeds.2021.03.034.
Chori BS, Danladi B, Inyang BA, et al. Hyperhomocysteinemia and its relations to conventional risk factors for cardiovascular diseases in adult Nigerians: the REMAH study. BMC Cardiovasc Disord. 2021;21(1):102. doi: 10.1186/s12872-021-01913-x.
Dutca G, Groppa S. Homocisteina – factor de risc în apariţia accidentului vascular cerebral acut şi corecţia ei medicamentoasă [Homocysteine - the risk factors in the apperance of acute cerebral vascular stroke]. In: Scientific Annals of Nicolae Testemițanu SUMPh. Chisinau; 2008. Vol. 3. p. 354-356. Romanian.
Lazzerini PE, Capecchi PL, Selvi E, et al. Hyperhomocysteinemia, inflammation and autoimmunity. Autoimmun Rev. 2007;6(7):503-509. doi: 10.1016/j.autrev.2007.03.008.
Wu H, Wang B, Ban Q, et al. Association of total homocysteine with blood pressure in a general population of Chinese adults: a cross-sectional study in Jiangsu province, China. BMJ Open. 2018;8(6):e021103. doi: 10.1136/bmjopen-2017-021103.
Gonçalves M, D’Almeida V, Guerra-Shinohara EM, et al. Homocysteine and lipid profile in children with Juvenile Idiopathic Arthritis. Pediatr Rheumatol. 2007;5:2. doi: 10.1186/1546-0096-5-2.
Drînga E. Factorii de risc minori pentru ateroscleroză = Minor risk factors for atherosclerosis. In: Scientific abstracts of students, residents and young researchers of Nicolae Testemițanu SUMPh. Chisinau: Medicina; 2019. p. 22.
Bichir-Thoreac L. Homocisteina factor de risc independent în hipertensiunea arterială la copii [Homocysteine as an independent risk factor in arterial hypertension at children]. Bull Acad Sci Mold. Med Sci. 2016;(2):169-171. Romanian.
Lai WKC, Kan MY. Homocysteine-induced endothelial dysfunction. Ann Nutr Metab. 2015;67(1):1-12. doi: 10.1159/000437098.
Huemer M, Fodinger M, Huemer C, et al. Hyperhomocysteinemia in children with juvenile idiopathic arthritis is not influenced by methotrexate treatment and folic acid supplementation: a pilot study. Clin Exp Rheumatol. 2003;21(2):249-55.
de Oliveira Leite L, Costa Dias Pitangueira J, Ferreira Damascena N, et al. Homocysteine levels and cardiovascular risk factors in children and adolescents: systematic review and meta-analysis. Nutr Rev. 2021;79(9):1067-1078. doi: 10.1093/nutrit/nuaa116.
Aronov A, Kim YJ, Sweiss NJ, et al. Cardiovascular disease risk evaluation impact in patients with rheumatoid arthritis. Am J Prev Cardiol. 2022;12:100380. doi: 10.1016/j.ajpc.2022.100380.
Urban M, Pietrewicz E, Górska A, Głowińska B. [Lipids and homocysteine level in juvenile idiopathic arthritis]. Pol Merkur Lekarski. 2004;17(99)235-238. Polish.
Bakkaloglu A, Kirel B, Ozen S, et al. Plasma lipids and lipoproteins in juvenile chronic arthritis. Clin Rheumatol. 1996;15(4):341-345. doi: 10.1007/BF02230355.
Semb AG, Holme I, Kvien TK, et al. Intensive lipid lowering in patients with rheumatoid arthritis and previous myocardial infarction: An explorative analysis from the incremental decrease in endpoints through aggressive lipid lowering (IDEAL) trial. Rheumatology (Oxford). 2011;50(2):324-329. doi: 10.1093/rheumatology/keq295.
Skare TL, Silva MB, Negreiros P. Lipid profile in adult patients with idiopathic juvenile arthritis. Rev Bras Rheumatol. 2013;53(4):371-374.
McCully KS. Vascular pathology of homocysteinemia: implications for the pathogenesis of arteriosclerosis. Am J Pathol. 1969;56(1):111-28.
Dinavahi R, Falkner B. Relationship of homocysteine with cardiovascular disease and blood pressure. J Clinical Hypertension. 2004;6(9):494-8. doi: 10.1111/j.1524-6175.2004.03643.x.
Fan R, Zhang A, Zhong F. Association between homocysteine levels and all-cause mortality: a dose-response meta-analysis of prospective studies. Sci Rep. 2017;7(1):4769. doi: 10.1038/s41598-017-05205-3.
Friso S, Jacques PF, Wilson PW, et al. Low circulating vitamin B6 is associated with elevation of the inflammation marker C-reactive protein independently of plasma homocysteine levels. Circulation. 2001;103(23):2788-2791. doi: 10.1161/01.cir.103.23.2788.
Chiang PK, Gordon RK, Tal J, et al. S-Adenosylmethionine and methylation. FASEB J. 1996;10(4):471-480.
Anan F, Masaki T, Umeno Y, et al. Correlations between homocysteine levels and atherosclerosis in Japanese type 2 diabetic patients. Metabolism. 2007;56(10):1390-1395. doi: 10.1016/j.metabol.2007.05.010.
Van Ede AE, Laan RFJM, Blom HJ, et al. Methotrexate in rheumatoid arthritis: An update with focus on mechanisms involved in toxicity. Semin Arthritis Rheum. 1998;27(5):277-292. doi: 10.1016/s0049-0172(98)80049-8.
Mansoor MA, Seljeflot I, Arnesen H, et al. Endothelial cell adhesion molecules in healthy adults during acute hyperhomocysteinemia and mild hypertriglyceridemia. Clin Biochem. 2004;37(5):408-414. doi: 10.1016/j.clinbiochem.2004.01.003.
Li M, Chen J, Li YS, et al. Folic acid reduces adhesion molecules VCAM-1 expression in aortic of rats with hyperhomocysteinemia. Int J Cardiol. 2006;106(2):285-288. doi: 10.1016/j.ijcard.2005.07.006.
Yi X, Zhou Y, Jiang D, et al. Efficacy of folic acid supplementation on endothelial function and plasma homocysteine concentration in coronary artery disease: a meta- analysis of randomized controlled trials. Exp Ther Med. 2014;7(5):1100-10. doi: 10.3892/etm.2014.1553.
Balkarli A, Tekintürk S, Kaptanoğlu B, et al. Relationship between plasma levels of homocysteine and pro-inflammatory cytokines in patients with rheumatoid arthritis. J Clin Exp Invest. 2016;7(2):163-167. doi: 10.5799/ahinjs.01.2016.02.0590.