
Introduction
Chronic obstructive pulmonary disease (COPD) is a major global health burden, characterized by persistent airflow limitation and progressive decline in lung function. According to the Global Initiative for Chronic Obstructive Lung Disease (GOLD 2024), COPD affects approximately 400 million people worldwide and remains the third leading cause of death globally [1]. In recent years, it has become increasingly evident that COPD extends beyond the respiratory system, acting as a systemic disease, frequently accompanied by a wide range of comorbidities [2].
The presence of comorbidities in COPD patients – such as cardiovascular disease, diabetes mellitus, metabolic syndrome, osteoporosis, anxiety, depression, gastrointestinal disorders, and respiratory comorbidities [3] – not only complicates disease management, but is also associated with increased frequency of exacerbations and hospitalizations, accelerated disease progression, reduced quality of life, and higher morbidity [4-6]. Many of these conditions interact pathophysiologically with COPD, amplifying systemic inflammation, altering therapeutic response, and complicating disease management [7].
Recent clinical guidelines recommend a multidimensional approach to COPD assessment that includes both respiratory and non-respiratory factors. Several composite indices have been developed to quantify the burden of comorbidities and facilitate prognostic evaluation. Among them, the Charlson Comorbidity Index (CCI), the COPD-specific Co-morbidity Test (COTE), the COPD Co-morbidity Risk Index (COPDCoRi), the CODEX Index (which integrates comorbidity, dyspnea, and exacerbation history), and the COMCOLD Index are increasingly used in both clinical practice and research [8-10].
The aim of this study was to assess the impact of comorbidities on COPD severity by analyzing their association with functional parameters (FEV1), clinical outcomes, and High-Resolution Computed Tomography (HRCT) findings. We further explored the predictive value of composite indices in stratifying disease severity based on the GOLD classification, with the goal of supporting a more personalized and evidence-based approach to patient management.
Material and methods
This was an analytical, observational, cross-sectional study conducted on a representative sample of patients diagnosed with COPD and associated comorbidities. The study was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes No. 30 dated 31.03.2022). Patients were stratified into two comparable subgroups based on the severity of airflow limitation, according to the current GOLD spirometric classification: GOLD stages 1-2 versus GOLD stages 3-4.
Study population. A total of 80 patients with confirmed COPD were enrolled from two tertiary medical institutions in the Republic of Moldova: Chiril Draganiuc Institute of Pneumology and the Saint Archangel Michael Municipal Clinical Hospital. The study was conducted between 2022 and 2025.
Inclusion and exclusion criteria. Eligible participants were aged over 40 years with a confirmed diagnosis of COPD based on spirometry (post-bronchodilator FEV1/FVC < 0.70) and at least one clinically or paraclinically documented comorbidity. Additional criteria included availability of complete medical documentation (clinical history, spirometry, and imaging), and a recent spirometry (performed within the last 12 months) during a period of respiratory stability. All participants provided written informed consent.
Patients were excluded if they were under 40 years old, had no relevant comorbidities, incomplete medical records, or alternative diagnoses such as asthma (FEV1/FVC > 0.70), idiopathic pulmonary fibrosis, advanced severe primary bronchiectasis, or active lung cancer. Patients with terminal chronic illnesses (e.g., NYHA IV heart failure), active tuberculosis, and severe post- COVID-19 pulmonary fibrosis were also excluded. Refusal to participate in the study was considered a definitive exclusion criterion.
Statistical data. Data were collected through direct patients’ interviews and medical records review, including demographic, anthropometric, clinical, functional and imaging parameters. Five validated composite indices were used to assess comorbidity burden: Charlson Comorbidity Index (CCI), the COPD-specific Co-morbidity Test (COTE), COPD Co-morbidity Risk Index (COPDCoRi), CODEX Index, and COMCOLD Index.
Statistical methods. Statistical analysis was performed using Microsoft Excel 2016, IBM SPSS Statistics (version 22.0), and MedCalc. Data normality was assessed using the Kolmogorov-Smirnov test. Continuous variables with normal distribution were reported as mean±standard deviation (SD), while non-normally distributed variables were presented as medians and interquartile range (IQR). Categorical variables were expressed as absolute and relative frequencies (%). To assess the association between composite indices and clinical, functional, and imaging parameters, Pearson correlation was used for continuous variables with normal distribution, while Spearman’s rank correlation was applied for ordinal or non-normally distributed data. Discriminative capacity was assessed via Receiver Operating Characteristic (ROC) curve analysis and area under the curve (AUC) interpretation.
Results
The study included 80 patients diagnosed with COPD, as indicated in Table 1. The majority were male (n = 59; 73.7%), while females constituted a smaller proportion (n = 21; 26.2%). Mean age = 65.6 years, SD = 8.28 years.
Table 1. Demographic and baseline data of participants (n = 80) | ||
Variable | Category | N (%) |
Gender
| Male Female | 59 (73.75%) 21 (26.25%) |
Age (years) | Mean = 65.6, SD = 8.28, Median = 66, IQR = 44-89 |
|
Environment | Urban Rural | 41 (51.25%) 39 (48.75%) |
Smoking status | Non-smoker Smoker Ex-smoker Passive smoker | 10 (12%) 38 (47.5%) 31 (38.75%) 1 (1.25%) |
Occupational exposure
| Non-exposed Exposed | 52 (65%) 28 (35%) |
Socioeconomic status
| Satisfactory Unsatisfactory | 65 (81.25%) 15 (18.75%) |
Note: Values are expressed as mean±SD for continuous variables (independent t-test) and n (%) for categorical variables (Chi-square test/Fisher’s exact test); SD – standard deviation; IQR- interquartile range. | ||
According to spirometric staging, 13.7% (n = 11) of patients were classified as GOLD 1, 36.2% (n = 29) as GOLD 2, 35% (n = 28) as GOLD 3, and 15% (n = 12) as GOLD 4. The mean post-bronchodilator FEV1 was 52.86% (SD = 19.12), ranging from 16.0% to 86.0%. Based on GOLD ABE classification, 11.2% of patients (n = 9) were in group A, 36.2% (n = 29) in group B, and 52.5% (n = 42) in group E. Details are summarized in Table 2.
Table 2. Functional and clinical parameters | ||
Variable | Category | n (%) |
GOLD stage | GOLD 1 GOLD 2 GOLD 3 GOLD 4 | 11 (13.75%) 29 (36.25%) 28 (35%) 12 (15%) |
FEV1 (%) Mean ±SD | 52.86 ± 19.12 |
|
Group | Group A Group B Group E | 9 (11.25%) 29 (36.25%) 42 (52.5%) |
Disease duration (years) | <10 years 10-20 years >20 years | 34 (42.5%) 37 (46.25%) 9 (11.25%) |
mMRC Dyspnea scale | Grade 1 Grade 2 Grade 3 Grade 4 | 4 (5%) 15 (18.75%) 37 (46.25%) 24 (30%) |
Number of exacerbation (in last years) | 1 exacerbation 2 exacerbations 3 exacerbations 4 exacerbations | 38 (47.5%) 28 (35%) 12 (15%) 2 (2.5%) |
SaO2
| <92% 93%-95% >95% | 30 (37.5%) 26 (32.5%) 24 (30.0%) |
Note: Values are expressed as mean ± SD for continuous variables (independent t-test) and n (%) for categorical variables (Chi-square test/Fisher’s exact test). GOLD – Global Initiative for Obstructive Lung Disease; FEV1 – forced expiratory volume in 1 second; SD – standard deviation; mMRC – modified Medical Research Council scale; SaO2 – Oxygen saturation; IQR- interquartile range. | ||
According to Table 3, a substantial burden of comorbidities was observed. Respiratory comorbidities – including recurrent pneumonia, bronchiectasis, bronchial asthma, lung cancer, and obstructive sleep apnea syndrome (OSAS) – were present in 75% of patients (n = 60). Cardiovascular diseases were highly prevalent (93.7%, n = 75) comprising ischemic heart disease, heart failure, arterial hypertension, arrhythmias, and peripheral arterial disease. Metabolic disorders (diabetes mellitus, dyslipidemia, and metabolic syndrome) affected 56.2% (n = 45). Osteoarticular conditions, such as osteoporosis or a history of vertebral fractures, were observed in 32.5% (n = 26). Cerebrovascular events (stroke) were reported in 2 cases (2.5%). Neuropsychiatric comorbidities – including depression, anxiety, and cognitive impairment – were present in 58.7% (n = 47). Gastrointestinal disorders were identified in 32.5% (n = 26). Other comorbidities, such as anemia, polycythemia, and non-pulmonary malignancies, were found in 47.5% (n = 38).
Table 3. Distribution of comorbidities by GOLD stage | ||
Comorbidities | GOLD 1-2 (n = 40) | GOLD 3-4 (n = 40) |
Cardiovascular disease | 37 | 38 |
Metabolic disorders | 23 | 22 |
Neuropsychiatric conditions | 25 | 22 |
Osteoarticular conditions | 11 | 15 |
Gastrointestinal disorders | 12 | 14 |
Respiratory comorbidities | 30 | 30 |
Other (anemia, polycythemia, malignancies) | 12 | 19 |
Note: Values represent the number of patients with each comorbidity in GOLD subgroups; GOLD – Global Initiative for Chronic Obstructive Lung Disease. | ||
HRCT identified a variety of structural abnormalities. Centrilobular emphysema was present in 40.0% of patients, cylindrical bronchiectasis in 35.0%, and radiological signs of pulmonary hypertension (PH) in 42.5%. Coronary artery calcifications were found in 27.5%, and radiological signs of vertebral fractures or osteoporosis in 20.0%. When comparing GOLD subgroups, patients with GOLD 3-4 had a significantly higher prevalence of structural lung damage. Cylindrical bronchiectasis (p = 0.016), centrilobular emphysema (p = 0.004), signs of PH (p = 0.001), coronary artery calcifications (p = 0.036), and osteoporosis (p = 0.044) were more frequently observed in the GOLD 3-4 group.
Correlation analysis showed a strong positive relationship between the number of exacerbations and hospitalizations (r = 0.483). Additionally, the number of exacerbations was positively correlated with the dyspnea score (mMRC) (r = 0.393), GOLD stage (r = 0.273), and ABE classification (r = 0.271). The mMRC score also showed significant positive correlations with disease duration (r = 0.258), GOLD stage (r = 0.301), ABE group (r = 0.354), and the Charlson Index (r = 0.306).
HRCT findings were also significantly correlated with clinical and functional variables. Cylindrical bronchiectasis showed a positive correlation with the number of exacerbations (r = 0.41, p < 0.01), while centrilobular emphysema exhibited a moderate negative correlation with post-bronchodilator FEV1 (r = –0.53, p < 0.001). Signs of PH were moderately associated with lower oxygen saturation (r = –0.48, p <0 .01) and higher dyspnea scores (r = 0.46), both statistically significant (p < 0.001).
As shown in Table 4, the Charlson Comorbidity Index was significantly correlated with several parameters, including frequency of hospitalizations (r = 0.255), number of exacerbations (r = 0.213), GOLD stage (r = 0.301), and mMRC score (r = 0.306). Among all indices, the CODEX score showed the strongest correlations with multiple clinical severity markers. Specifically, it showed a strong positive correlation with post-bronchodilator FEV1 severity classified by GOLD 2024 (r = 0.59). Additionally, the CODEX index was positively associated with the mMRC dyspnea scale (r = 0.46), number of exacerbations (r = 0.41), and ABE classification (r = 0.47). The COMCOLD score showed strong correlations with other comorbidity indices, including CCI (r = 0.57), CODEX (r = 0.34), and COTE (r = 0.32). It also exhibited weak-to-moderate associations with dyspnea severity (mMRC, r = 0.16) and BMI (r = 0.09). The COTE index was modestly correlated with disease duration (r = 0.26), number of exacerbations (r = 0.15), and gender (r = 0.20). Lastly, the COPDCoRi index showed modest associations with COTE (r = 0.41), COMCOLD (r = 0.33), and CCI (r = 0.32). Notably, it also showed a negative correlation with peripheral oxygen saturation (SaO2, r = –0.15).
Table 4. Correlation of composite indices and clinical variables | |||||
Clinical Variable | Charlson | CODEX | COMCOLD | COTE | COPDCoRi |
Hospitalizations | r = 0.255** | r = 0.34** | - | - | - |
Exacerbations | r = 0.21* | r = 0.41*** | - | r = 0.15* | - |
GOLD (FEV1) | r = 0.30** | r = 0.59*** | - | - | r=0.41** |
mMRC | r = 0.30** | r = 0.46*** | r = 0.16* | - | - |
Disease duration | - | - | - | r = 0.26** | - |
ABE type | - | r = 0.47*** | - | - | - |
Smoking status | - | - | - | r = 0.20* | r = 0.33* |
BMI | - | - | r = 0.09 | - | - |
Charlson | - | - | r = 0.57*** | - | r = 0.32* |
CODEX | - | - | r = 0.34** | - | - |
COTE | - | - | r = 0.32* | - | r = 0.41** |
COMCOLD | r = 0.57*** | r = 0.34** | - | r = 0.32*** | r = 0.33* |
COPDCoRi | r = 0.32** | - | r = 0.33* | r = 0.41*** | - |
Note: Values represent correlation coefficients (r) between composite indices and clinical variables. Pearson or Spearman correlation coefficients were used depending on data distribution; * p < 0.05; ** p < 0.01; *** p < 0.001; - No analysis or non-significant correlation; GOLD – Global Initiative for Chronic Obstructive Lung Disease; FEV1 – forced expiratory volume in 1 second; mMRC – modified Medical Research Council scale; ABE – GOLD 2024 classification; BMI – body mass index; CCI – Charlson Comorbidity Index; CODEX – Comorbidity, Obstruction, Dyspnea, and Exacerbation risk index; COMCOLD – COPD Comorbidity and Depression index; COTE - COPD –specific Comorbidity test; COPDCoRi – Comorbidity Risk Index. | |||||
To evaluate the predictive performance of selected composite comorbidity indices in distinguishing severe forms of COPD (GOLD 3-4), we performed binary logistic regression analyses followed by ROC curve assessment. Logistic regression analysis revealed that the Charlson Comorbidity Index (CCI) alone had limited predictive ability for advanced COPD (AUC = 0.63), indicating modest discriminatory ability. However, when a combination of composite indices – the COTE index, the CODEX index, and the COPDCoRi index – was included as predictors, the multivariable logistic model demonstrated substantially higher discriminative power, with an AUC = 0.86. All three indices showed positive regression coefficients, suggesting that elevated scores are significantly associated with advanced GOLD classification (Fig. 1).
To further assess the predictive value of HRCT findings, logistic regression models were built. In the GOLD 3-4 group, HRCT variables such as centrilobular emphysema and PH signs emerged as significant predictors. ROC curve analysis demonstrated good discrimination for severe COPD (AUC = 0.81), and moderate discrimination for GOLD 1-2 (AUC = 0.71).
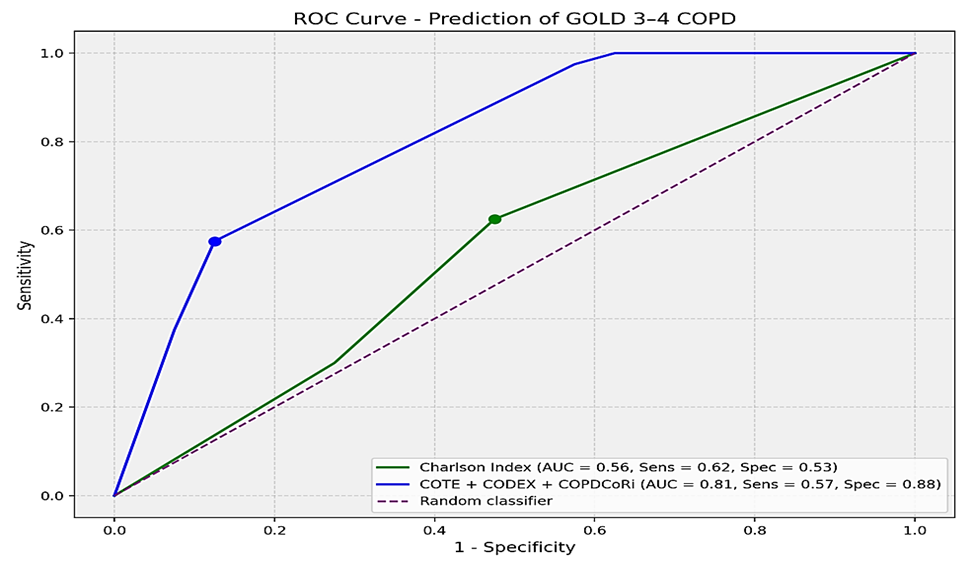 |
Fig. 1 Receiver Operating Characteristic (ROC) curve for prediction of GOLD 3-4 COPD Note: The ROC curve compares the predictive performance of the Charlson Index (green line) and a combined model incorporating COTE, CODEX, and COPDCoRi scores (blue line) in identifying patients with GOLD 3-4 COPD. The Charlson Comorbidity Index showed poor discriminative performance, with an AUC = 0.56 (p = 0.355), Sensitivity = 0.62, Specificity = 0.53. These results were not statistically significant, and further studies with larger cohorts are needed to confirm its predictive value in COPD severity. In contrast, the combined model including COTE, CODEX, and COPDCoRi scores demonstrated a significantly higher discriminative capacity (AUC = 0.81, p < 0.001), Sensitivity = 0.57, Specificity = 0.88. Among predictors, CODEX was statistically significant (p < 0.001), COTE showed a trend (p = 0.099), and COPDCoRi did not reach statistical significance (p = 0.214); however, its potential clinical relevance warrants further investigation in larger cohorts. AUC – Area Under the Curve. |
Discussion
This study underscores the multidimensional nature of COPD, reaffirming prior findings that comorbidities substantially impact disease burden and prognosis [11-13]. In agreement with earlier observations, our results confirm the high prevalence of cardiovascular and metabolic comorbidities, especially in patients with advanced stages of COPD.
The radiological presence of bronchiectasis and emphysema in more severe GOLD stages is consistent with previous CT-based classifications. Lynch et al. and Martinez et al. have emphasized that structural abnormalities correlate with both functional impairment and exacerbation risk, which aligns with our data showing an inverse relationship between emphysema scores and FEV1 values [14, 15]. Furthermore, the co-occurrence of bronchiectasis and exacerbations supports findings by Martinez-Garcia et al., reinforcing their clinical significance [16].
Among the composite indices assessed, CODEX exhibited the strongest correlation with clinical severity markers [17, 18], corroborating its multidimensional nature. The COPDCoRi index also demonstrated robust associations, in line with recent efforts to integrate comorbidity burden into COPD phenotyping [19]. While the COTE index was originally designed to predict mortality [20], our findings show that it retains relevance for stratifying patients by disease characteristics.
ROC analysis confirmed that disease-specific indices such as CODEX and COPDCoRi yielded higher AUCs for GOLD stage prediction, outperforming general indices like the Charlson. These results support earlier validations of these indices in stratifying COPD risk and outcomes [21]. Moreover, HRCT features such as emphysema extent and pulmonary hypertension added prognostic value, underscoring the importance of imaging biomarkers. Taken together, these findings support the GOLD 2024 recommendations for multidimensional evaluation of COPD patients. By combining functional, clinical, and imaging variables, more accurate risk stratification becomes feasible.
Limitations of the study include its cross-sectional design and moderate sample size, potentially limiting generalizability. Additionally, some comorbidities may have been underreported due to retrospective data collection.
Future research should investigate the longitudinal predictive value of composite indices and HRCT biomarkers, as suggested by studies on disease progression and mortality prediction in COPD.
Conclusions
This study reinforces the central role of comorbidities and structural lung changes in defining COPD severity. By integrating validated composite indices (Charlson, CODEX, COTE, COPDCoRi, COMCOLD) and HRCT findings, we demonstrate that a multidimensional assessment better reflects disease complexity and prognosis than conventional measures alone. The findings support the use of COPD-specific tools and imaging biomarkers in routine evaluation, promoting a more personalized and evidence-based management approach in line with GOLD 2024 recommendations.
Competing interest
None declared.
Contribution of authors
AC – research coordinator, conceived the research idea, developed the aim and objectives, and supervised data interpretation. EI performed data collection, analysis, and manuscript drafting. Both authors critically reviewed and approved the final manuscript.
Ethics approval
The study was conducted as part of a doctoral research project approved by the Research Ethics Committee of the Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes No. 30 dated 31.03.2022).
Patient consent
Obtained.
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned; externally peer-reviewed.
Authors’ ORCID IDs
Ecaterina Iavrumov – https://orcid.org/0000-0001-7332-6587
Alexandru Corlateanu – https://orcid.org/0000-0002-3278-436X
References
1. Venkatesan P. GOLD COPD report: 2024 update. Lancet Respir Med. 2024;(1):15-6. doi: 10.1016/S2213-2600(23)00461-7
2. Agustí A, Celli BR, Criner GJ, Halpin D, Anzueto A, Barnes P, et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD executive summary. Eur Respir J. 2023 Apr 1;61(4). https://doi.org/10.1183/13993003.00239-2023
3. Natali D, Cloatre G, Hovette P, Cochrane B. Screening for comorbidities in COPD. Breathe (Sheff). 2020;16(1):190315. https://doi.org/10.1183/20734735.0315-2019
4. Divo M, Cote C, de Torres JP, Casanova C, Marin JM, Pinto-Plata V, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012 Apr 19;186(2):155-61. doi: 10.1164/rccm.201201-0034OC
5. Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008 Sep 30;32(4):962-9. https://doi.org/10.1183/09031936.00012408
6. Corlateanu A, Covantev S, Scutaru E, Rusu D, Botnaru V, Corlateanu O, Siafakas N. COPD and comorbidities in the Republic of Moldova. Eurasian J Pulmonol. 2022 Feb 08;24(1):9-17. doi: 10.14744/ejop_78_21
7. Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009 Jan 05;33(5):1165-85. https://doi.org/10.1183/09031936.00128008
8. Ly K, Wakefield D, ZuWallack R. The usefulness of Charlson Comorbidity Index (CCI) scoring in predicting all-cause mortality in Outpatients with Clinical Diagnoses of COPD. J Multimorb Comorb. 2025 Jan 25;15:1-7. https://doi.org/10.1177/26335565251315876
9. Divo MJ, Casanova C, Marin JM, Pinto-Plata VM, De-Torres JP, Zulueta JJ, et al. COPD comorbidities network. Eur Respir J. 2015 Aug 31;46(3):640-50. https://doi.org/10.1183/09031936.00171614
10. Frei A, Muggensturm P, Putcha N, Siebeling L, Zoller M, Boyd CM, et al. Five comorbidities reflected the health status in patients with chronic obstructive pulmonary disease: the newly developed COMCOLD index. J Clin Epidemiol. 2014 Apr 29;67(8):904-11. https://doi.org/10.1016/j.jclinepi.2014.03.005
11. Smith MC, Wrobel JP. Epidemiology and clinical impact of major comorbidities in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2014 Aug 27;9:871-88. https://doi.org/10.2147/COPD.S49621
12. dos Santos NC, Miravitlles M, Camelier AA, de Almeida VDC, Tosta Maciel RRB, Rosa Camelier FW. Prevalence and impact of comorbidities in individuals with chronic obstructive pulmonary disease: a systematic review. Tuberc Respir Dis (Seoul). 2022 May 27;85(3):205-20. https://doi.org/10.4046/trd.2021.0179
13. Negewo NA, Gibson PG, McDonald VM. COPD and its comorbidities: impact, measurement and mechanisms. Respirology. 2015 Sep 16;20(8):1160-71. https://doi.org/10.1111/resp.12642
14. Dou S, Zheng C, Cui L, Xie M, Wang W, Tian H, et al. High prevalence of bronchiectasis in emphysema-predominant COPD patients. Int J Chron Obstruct Pulmon Dis. 2018 Jun 27;13:2041-7. https://doi.org/10.2147/COPD.S163243
15. Mets OM, De Jong PA, Van Ginneken B, Gietema HA, Lammers JWJ. Quantitative computed tomography in COPD: possibilities and limitations. Lung. 2012 Dec 17;190(2):133-45. https://doi.org/10.1007/s00408-011-9353-9
16. Miravitlles M, Calle M, Soler-Cataluña JJ. Clinical phenotypes of COPD: identification, definition and implications for guidelines. Arch Bronconeumol. 2012 Feb 1;48(3):86-98. doi: 10.1016/j.arbr.2012.01.003
17. Deng D, Zhou A, Chen P, Shuang Q. CODEXS: a new multidimensional index to better predict frequent COPD exacerbators with inclusion of depression score. Int J Chron Obstruct Pulmon Dis. 2020 Feb 3;15:249-59. https://doi.org/10.2147/COPD.S237545
18. Corlateanu A, Plahotniuc A, Corlateanu O, Botnaru V, Bikov A, Mathioudakis AG, et al. Multidimensional indices in the assessment of chronic obstructive pulmonary disease. Respir Med. 2021 Jun 22;185:106519. https://doi.org/10.1016/j.rmed.2021.106519
19. Cazzola M, Calzetta L, Matera MG, Muscoli S, Rogliani P, Romeo F. Chronic obstructive pulmonary disease and coronary disease: COPDCoRi, a simple and effective algorithm for predicting the risk of coronary artery disease in COPD patients. Respir Med. 2015 May 25;109(8):1019-25. https://doi.org/10.1016/j.rmed.2015.05.021
20. Chen Q, Wang X, Yao X, Zhang L, Liu X. COTE and pulmonary comorbidities predict moderate-to-severe acute exacerbation and hospitalization in COPD. Int J Chron Obstruct Pulmon Dis. 2025 Jun 11;20:1893-913. https://doi.org/10.2147/COPD.S518218
21. Kotlyarov S. The role of multidimensional indices for mortality prediction in chronic obstructive pulmonary disease. Diagnostics (Basel). 2023 Apr 4;13(7):1344. https://doi.org/10.3390/diagnostics13071344