
Introduction
Aortic stenosis is the most common severe degenerative valvular disease requiring interventional or surgical treatment, characterized by a progressive reduction in the aortic valve area below 1 cm² from the normal values of 2–3 cm² [1, 2]. The prevalence of aortic stenosis is estimated at approximately 0.4% in the general population; however, this figure underestimates the reality in older age groups, where the incidence is significantly higher [3]. For the population over 60 years of age, studies report the following prevalence rates: 1.3% in the sixth decade of life, 3.9% in the seventh decade, and 9.8% among patients aged 80–89 years [4]. Another important epidemiological aspect is the frequent coexistence of ischemic heart disease (IHD) with aortic stenosis. Data on the prevalence of coronary artery disease among patients undergoing TAVI vary considerably, ranging from 15% to 82% [5–8]. Nevertheless, coronary revascularization is performed in only 10–20% of patients undergoing TAVI [5].
Coronary blood flow dynamics depends on a balance between ventricular, arterial, and neurohumoral mechanisms, in which the aortic valve plays a key role. In aortic stenosis, impaired valvular function reduces coronary flow reserve (CFR) and promotes myocardial ischemia [6]. Coronary blood flow is affected both proximally, by factors such as hypotension, left ventricular dysfunction, and aortic pathology, and distally, through microcirculatory dysfunction, ventricular hypertrophy, and diastolic dysfunction. In aortic stenosis, perfusion is reduced due to decreased perfusion pressure and microcirculatory remodeling associated with hypertrophy [6-8].
Coronary perfusion is regulated by the interaction between diastolic backward expansion waves (dBEW) and systolic forward compression waves (sFCW) [6]. The dynamics of these waves ensure adequate myocardial blood flow, particularly under the altered hemodynamic conditions associated with aortic stenosis. The reduction in stroke volume through the narrowed aortic valve leads to a decrease in mean arterial pressure. As a result, the pressure gradient between the aorta and the coronary arteries, as well as coronary perfusion pressure, decreases, thereby reducing oxygen delivery to the myocardium [9].
Left ventricular hypertrophy, although initially compensatory by reducing wall stress, decreases myocardial capillary density, increasing oxygen diffusion distance and creating an imbalance between increased oxygen demand and reduced coronary supply [9]. Under conditions of increased metabolic demand, coronary blood flow becomes dependent on the relative duration of diastole, which shortens as heart rate increases—a frequent finding in aortic stenosis. Consequently, tachycardia reduces subendocardial perfusion time, exacerbating the risk of ischemia [1,6]. In addition, diffuse fibrosis and left ventricular diastolic dysfunction—present in approximately 62% of patients with aortic stenosis [10], further contribute to symptom burden. Studies have demonstrated a strong correlation between the severity of dyspnea and the presence of myocardial fibrosis associated with diastolic dysfunction [10,11].
In patients with severe aortic stenosis and coronary artery disease, valve selection must consider coronary anatomy, post-implantation access, and the possibility of future coronary interventions, as the design of the transcatheter valve influences coronary ostia accessibility. [12].
Our study aims to contribute to the understanding of the complex interplay between severe aortic stenosis, diastolic dysfunction, and ischemic coronary artery disease, with the goal of identifying the implications of this triple impact on preprocedural assessment and post-TAVI prognosis in elderly patients with advanced cardiac pathology.
Material and methods
The observational analytical cohort study (both retrospective and prospective) included 85 elderly patients with severe aortic stenosis who underwent transcatheter aortic valve implantation (TAVI) between 2019 and 2023. The patients were selected from the interventional cardiology database of the Institute of Cardiology in Chisinau, Republic of Moldova. The inclusion criteria were: age ≥70 years, severe or pseudo-severe “low-flow, low-gradient” aortic stenosis, coronary artery disease eligible for percutaneous coronary intervention (PCI), and a minimum follow-up period of 1 year. The exclusion criteria were: age <70 years, mild or moderate aortic stenosis, non-PCI-eligible coronary lesions, myocardial infarction within the previous 90 days, previous coronary artery bypass grafting, and lack of informed consent. All patients included in the study met the eligibility criteria and signed informed consent forms. The study was approved by the Ethics Committee of the State University of Medicine and Pharmacy “Nicolae Testemitanu” (approval number 3/4.3/2024-03-19). Subsequently, patients were divided into two groups based on the myocardial revascularization strategy adopted before TAVI:
TAVI group (n = 56) – patients who underwent TAVI alone, without percutaneous coronary intervention.
TAVI+PCI group (n = 29) – patients who underwent both TAVI and PCI for the revascularization of significant coronary lesions.
The decision regarding the management of coronary artery disease (medical therapy versus coronary angioplasty) was made by the Heart Team based on national and international guideline recommendations, as well as individual patient characteristics. The primary indication for performing PCI was the presence of at least one stenosis ≥50% of the left main coronary artery trunk or a stenosis ≥70% of major coronary branches.
Diastolic function was evaluated echocardiographically according to the 2016 guidelines of the European Association of Cardiovascular Imaging (EACVI) [13], using a standardized multiparametric algorithm. Key parameters obtained from pulsed-wave Doppler included the transmitral inflow velocities: the E wave, representing early diastolic filling, and the A wave, corresponding to atrial contraction. The E/A ratio was analyzed for initial insight into the filling pattern. Tissue Doppler imaging (TDI) of the septal and lateral mitral annulus was used to measure early diastolic myocardial velocities (e’), providing information on active myocardial relaxation. The E/e’ ratio was calculated as a surrogate marker of left ventricular filling pressures, with values >14 generally indicating elevated filling pressures. Additional structural parameters included the left atrial volume index (LAVI), measured by the biplane area-length method, which serves as a chronic marker of diastolic burden. A LAVI >34 mL/m² was considered abnormal. The peak tricuspid regurgitation velocity was assessed using continuous-wave Doppler to estimate pulmonary artery systolic pressure, a secondary indicator of increased left-sided filling pressures. Where image quality permitted, pulmonary venous flow and mitral deceleration time were also evaluated. Diastolic dysfunction was classified as: grade I (impaired relaxation with normal filling pressures), grade II (pseudonormal pattern indicating moderate elevation of filling pressures), and grade III (restrictive filling, associated with severe elevation of left atrial pressure and poor prognosis). All echocardiographic measurements were performed at end-expiration, with the patient in left lateral decubitus, using apical four-chamber views. To ensure reproducibility, each value was averaged over at least three cardiac cycles in sinus rhythm and five in the presence of atrial fibrillation. The classification of diastolic dysfunction required concordance between at least three out of four principal parameters, as per guideline recommendations. Cases with discordant or borderline values were categorized as “indeterminate diastolic function.”
Statistical analyses were performed using SPSS version 25.0 (2017). Due to non-normal data distribution, non-parametric tests were applied. Continuous variables were presented as median and interquartile range (IQR) and compared using the Mann–Whitney U test. Categorical variables were analyzed with Chi-square or Fisher’s exact test, as appropriate. A p-value <0.05 was considered statistically significant.
Results
To assess the impact of coronary revascularization on postprocedural outcomes following TAVI, the preprocedural characteristics of the two patient groups were compared, as presented in Table 1.
Table 1. Preprocedural characteristics of the “TAVI” and “TAVI+PCI” groups. | |||
Parameter | TAVI (n = 56) | TAVI+ PCI (n = 29) | p |
Age (years, mean ± SD) | 77.2 ± 4.6 | 76.9 ± 5.0 | 0.82 |
Male sex, n (%) | 15 (26.3%) | 14 (48.2%) | 0.04 |
BMI (kg/m², mean ± SD) | 30.7 ± 5.1 | 28.9 ± 4.7 | 0.14 |
Hypertension, n (%) | 56 (100%) | 28 (96.5%) | 0.33 |
Diabetes mellitus, n (%) | 18 (31.5%) | 12 (41.3%) | 0.40 |
Atrial fibrillation, n (%) | 22 (38.6%) | 5 (20.58%) | 0.04 |
Dyslipidemia, n (%) | 44 (77.2%) | 27 (93.1%) | 0.07 |
AVA (cm², mean ± SD) | 0.55 ± 0.17 | 0.69 ± 0.16 | 0.57 |
Mean gradient (mm Hg, mean ± DS) | 55.1 ± 14.8 | 53.4 ± 14.5 | 0.53 |
Peak gradient (mm Hg, mean ± DS) | 89.1 ± 21.8 | 85.1 ± 22.2 | 0.43 |
Vmax (m/s, mean ± DS) | 4.6 ± 0.6 | 4.64 ± 0.7 | 0.54 |
LVEF (%, mean ± DS) | 59.2 ± 7.6 | 57.4 ± 7.9 | 0.10 |
Pulmonary hypertension, n (%) | 47 (82.4%) | 21 (72.4%) | 0.58 |
Angina pectoris (FC II-III), n (%) | 38 (66.6%) | 27 (93.1%) | 0.008 |
NYHA III-IV, n (%) | 43 (75.4%) | 24 (88.8%) | 0.24 |
EuroSCORE II (%, mean ± DS) | 4.4 ± 2.6 | 3.7 ± 2.5 | 0.17 |
STS score (%, valoarea medie ± SD) | 4.5 ± 1.8 | 3.1 ± 3.6 | 0.96 |
Note: BMI – body mass index, AVA – aortic valve area, Vmax – maximum velocity across the aortic valve, LVEF – left ventricle ejection fraction, STS score - the Society of Thoracic Surgeons risk score. n – number of patients; mean (SD), Wilcoxon rank-sum test, Pearson Chi-Square test with estimated p-value. | |||
In the study, among the 85 evaluated patients, 80% (n = 68) reported retrosternal pain, confirming the high frequency of anginal symptoms in severe aortic stenosis. In 12.9% of patients (n = 11), chest pain was the dominant symptom and the primary reason for cardiologic evaluation. Regarding triggering factors, chest pain was induced by physical exertion in 71.7% of patients (n = 61). Only one patient (1.17%) attributed the pain onset to emotional factors, and 2.35% (n = 2) reported an association with exposure to low temperatures. In 4.7% of cases (n = 4), chest pain could not be correlated with any evident trigger. According to the functional class (FC) of angina pectoris based on the Canadian Cardiovascular Society (CCS) classification, symptom severity was distributed as follows: 3 patients (4.4%) were classified as FC I, presenting occasional pain episodes during strenuous exertion; 33 patients (48.5%) were in FC II, reporting chest pain during moderate effort; and 32 patients (47.1%) were in FC III, experiencing pain during minimal effort. This distribution indicates a predominance of effort angina with moderate to severe severity.
Following the correlation of angina pectoris with ischemic coronary artery disease, an uneven distribution of symptoms was observed according to the severity of coronary lesions. Among the 32 patients with severe angina (FC III), 62.5% (n = 20) presented coronary lesions with >50% stenosis, while 37.5% (n = 12) had minimal coronary lesions, suggesting a non-atherosclerotic ischemic mechanism of chest pain, likely due to impaired coronary flow secondary to severe aortic stenosis. In patients with moderate angina (FC II), 33.3% (n = 11) had coronary artery disease, whereas 66.7% (n = 22) did not exhibit significant coronary lesions. All patients with FC I (n = 3) had patent coronary arteries (Table 2).
Table 2. Association between angina severity and coronary artery disease CAD. | |||
CCS Functional Class of Angina Pectoris | Patients with CAD | Patients without CAD | Total Patients |
Class I, 3 (4.41%) | 0 (0%) | 3 (100%) | 3 |
Class II, 33 (48.53%) | 11 (33.33%) | 22 (66.67%) | 33 |
Class III, 32 (47.06%) | 20 (62.5%) | 12 (37.5%) | 32 |
Total | 31 | 37 | 68 |
Note: CCS – Canadian Cardiovascular Society; CAD – Coronary Artery Disease;. n – number of patients; mean (SD), Wilcoxon rank-sum test, Pearson Chi-Square test with estimated p-value. | |||
Although there are some differences between the groups, the overall patient profile is similar in terms of comorbidities, aortic stenosis severity, preoperative surgical risk, and left ventricular function.
Left ventricular diastolic dysfunction (LVDD) was significantly more frequent in Group II—patients undergoing concomitant TAVI and PCI. This difference supports the hypothesis that significant coronary artery disease, even when treated percutaneously, is frequently associated with persistent diastolic dysfunction, reflecting pre-existing myocardial remodeling. From a clinical perspective, Group II patients may represent a subgroup with greater functional vulnerability after TAVI, requiring closer echocardiographic monitoring during follow-up.
The distribution of LVDD grades according to the 2016 EACVI guidelines was as follows: Grade I (impaired relaxation) – 17.5% in Group I vs. 24.1% in Group II; Grade II (pseudonormal) – 47.4% in Group I vs. 41.3% in Group II; Grade III (restrictive) – 35.1% in Group I vs. 13.8% in Group II. Although the overall differences did not reach statistical significance (p = 0.063), the presence of a restrictive pattern in more than one-third of Group II patients has major clinical implications. These patients may have an increased risk of post-TAVI decompensation and could benefit from more aggressive diuretic optimization and serial echocardiographic follow-up.
In our study, the median values of the E/A ratio were significantly different between the group of patients treated with TAVI+PCI and the group undergoing TAVI alone, suggesting more severe diastolic dysfunction in the former group. The median E/A in Group II (TAVI+PCI) was 1.9 (IQR = 0.4), indicating a trend toward a restrictive filling pattern, compared to 1.6 (IQR = 0.3) in group I (TAVI only) , reflecting more preserved diastolic function with a less severe dysfunction pattern (Fig. 1).
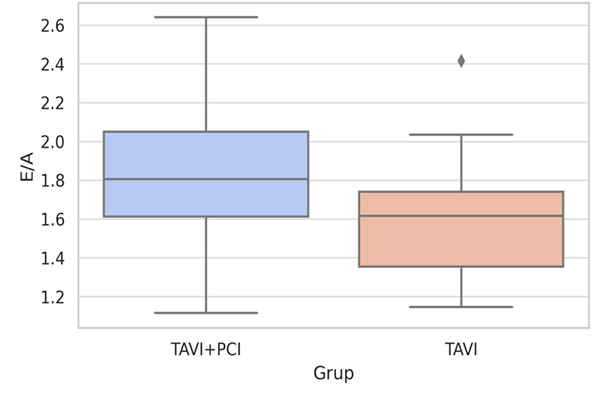 |
Fig. 1 Distribution of the E/A ratio in the both groups Note: The blue box represents patients TAVI+PCI, while the orange box represents patients undergoing TAVI alone. |
The velocity of the E wave was significantly lower in Group II: 152.4 cm/s (IQR = 43.0) compared to 173.0 cm/s (IQR = 32.0) in Group I (p = 0.014), suggesting more pronounced impairment of active myocardial relaxation. This finding is frequently observed in the presence of chronic ischemia or fibrodegenerative infiltration—both common features in TAVI-eligible patients with concomitant coronary artery disease. An E/A ratio ≥2, indicative of a restrictive filling pattern, was more frequently observed in Group II. This difference reached statistical significance (p = 0.04) and, clinically, is often associated with severe heart failure symptoms and reduced tolerance to hemodynamic changes after the procedure.
The velocity of the A wave was slightly lower in Group II—70.3 cm/s (IQR = 18.6) compared to 75.9 cm/s (IQR = 21.2) in Group I, without statistical significance (p = 0.13). However, this contributes to the picture of passive ventricular filling dominated by elevated pressures, especially when correlated with increased E wave velocity and decreased e’ wave velocity.
The E/e′ ratio, used to estimate left ventricular filling pressure, was significantly higher in Group II—9.2 (IQR = 5.4) compared to 6.4 (IQR = 4.2) in Group I (p = 0.003). Values close to or exceeding 10 in the TAVI+PCI subset suggest elevated end-diastolic pressure, which may clinically manifest as residual pulmonary congestion post-procedure despite correction of the stenosis (Fig. 2). Additionally, 42.1% of patients in Group II had an E/e′ ≥10, compared to only 13.8% in Group I (p = 0.012). This observation may indicate the need for early reassessment of diuretic therapy post-TAVI in patients undergoing concomitant revascularization.
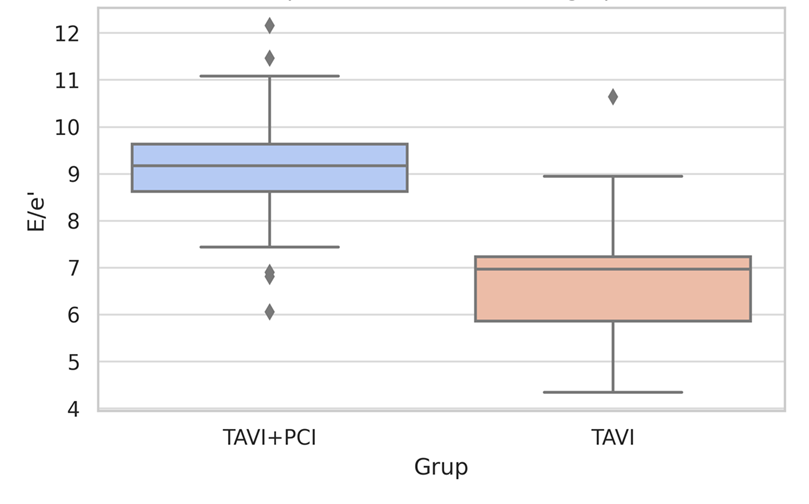 |
Fig. 2 Comparison of the E/e′ ratio Note: The blue box represents patients TAVI+PCI, while the orange box represents patients undergoing TAVI alone. |
The E/Vp ratio was significantly higher in Group II: 1.2 (IQR = 0.4) versus 0.8 (IQR = 0.5) in Group I (p < 0.001). E/Vp is a robust parameter for estimating filling pressure, independent of sinus rhythm, making it especially valuable in the context of the frequent atrial fibrillation observed in these patients.
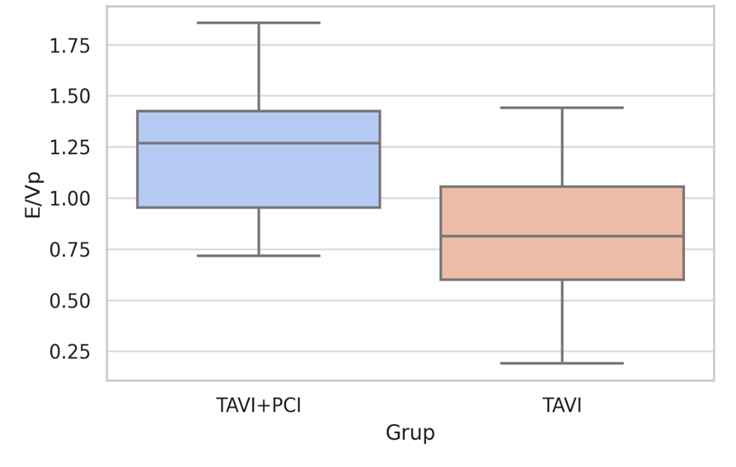 |
Fig. 3 Distribution of the E/Vp ratio Note: The blue box represents patients TAVI+PCI, while the orange box represents patients undergoing TAVI alone. |
The median isovolumetric relaxation time (IVRT) was shorter in Group II—72 ms (IQR = 14) compared to 78 ms (IQR = 17) in Group I (p = 0.082). A reduced IVRT reflects a stiff left ventricle that rapidly enters passive filling—typical for pseudo normal or restrictive filling patterns.
The deceleration time of the E wave (DTE) was significantly shorter in Group II—184 ms (IQR = 38) versus 207 ms (IQR = 41) in Group I (p = 0.033). A DTE <160 ms is considered an indirect marker of elevated end-diastolic pressure and decreased left ventricular compliance. In Group II, over one-third of patients had a DTE <160 ms.
Discussion
Aortic stenosis is the leading cause of valvular heart disease in the Western world and is associated with increased morbidity and mortality [14]. Progressive narrowing of the valve results in pressure overload of the left ventricle (LV), leading to hypertrophy and fibrosis, which can ultimately cause systolic and/or diastolic dysfunction of the LV [15]. The severity of diastolic dysfunction correlates with the severity of postprocedural hemodynamic parameters and the clinical course of the patient.
Percutaneous coronary revascularization (PCI) before TAVI is traditionally recommended to optimize coronary blood flow and reduce the risk of ischemic events during the hemodynamic stress generated by transcatheter aortic valve implantation [16]. This approach is consistent with current guidelines, which recommend prioritizing PCI for coronary artery lesions with >70% stenosis in proximal segments or >50% in the left main coronary artery, in order to ensure adequate myocardial perfusion, thereby reducing the risk of perioperative myocardial infarction and improving overall outcomes [2]. However, our results show that patients undergoing concomitant TAVI and PCI exhibit a more severe degree of diastolic dysfunction despite revascularization, compared with those treated with TAVI alone. Echocardiographic parameters (E, E/A, E/e′, E/Vp, DTE) indicated elevated end-diastolic pressures and a predominant restrictive diastolic pattern in the TAVI+PCI group, suggesting persistent subendocardial myocardial impairment, likely reflecting fibrotic remodeling or residual microvascular dysfunction.
This observation supports the hypothesis of a bidirectional mechanism between chronic myocardial ischemia and diastolic dysfunction: on one hand, coronary artery disease contributes to impaired ventricular filling through subendocardial ischemia, while on the other hand, elevated filling pressures and reduced ventricular compliance further compromise subendocardial coronary flow, especially in the context of reduced coronary flow reserve in severe aortic stenosis [17-19].
The presence of a restrictive diastolic pattern in one-third of revascularized patients highlights the importance of diastolic function assessment as a prognostic parameter. Moreover, the higher E/e′ and E/Vp ratios in the TAVI+PCI group are correlated with elevated filling pressures and more fragile hemodynamic tolerance, suggesting the need for rigorous postprocedural echocardiographic monitoring [20-21].
Recent literature supports the use of diastolic echocardiography not only as a diagnostic tool but also for guiding post-TAVI therapy. Studies such as PARTNER 3 and subanalyses from the TVT registry have shown that diastolic dysfunction correlates with cardiovascular mortality and rehospitalizations for heart failure [22]. In this context, patients undergoing TAVI+PCI may represent a functionally vulnerable subgroup requiring a personalized therapeutic strategy, including optimization of volume status, BNP/NT-proBNP assessment, and serial echocardiographic follow-up.
Our data support integrating diastolic dysfunction assessment into the pre-TAVI evaluation algorithm and postprocedural monitoring, particularly in patients with concomitant coronary artery disease. Evaluating diastolic function can guide patient selection and therapeutic adjustments, with potential independent prognostic value. In an increasingly complex clinical setting marked by comorbidities and multidimensional therapeutic decisions, a thorough understanding of the interplay between ischemia and diastolic function becomes essential for treatment individualization and optimization of post-TAVI outcomes.
The main limitation of our study is the relatively small sample size, explained by the limited number of procedures performed and the low prevalence of significant coronary stenoses; however, the findings remain clinically relevant and provide valuable hypothesis-generating insights.
Conclusion
Left ventricular diastolic dysfunction was more frequent and more severe in patients undergoing concomitant TAVI and PCI compared to those treated with TAVI alone. Echocardiographic parameters (E/A, E/e′, E/Vp, DTE, IVRT) demonstrated a more impaired diastolic profile, with elevated end-diastolic pressures and a prevalent restrictive pattern in the TAVI+PCI group. These results suggest that significant coronary artery disease, even when treated, is associated with persistent myocardial remodeling and compromised diastolic function. Clinically, patients undergoing TAVI+PCI represent a vulnerable subgroup requiring more frequent echocardiographic follow-up and careful adjustment of postprocedural therapy.
Competing interests
None declared.
Authors’ contributions
Substantial contribution to conception and design of the work, MA; substantial contribution to acquisition of data, DB, EP, CC; substantial contribution to analysis and interpretation of data, DB; drafting the article, M-MV, EP; critically reviewing the article for important intellectual content; MA; final approval of the version to be published, MA; taking responsibility and being accountable for all aspects of the work, MA, EP, M-MV. All the authors have read and agreed with the final version of the article.
Patient consent
Obtained.
Ethics approval
The study was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (approval number 3/4.3/2024-03-19).
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Authors’ ORCID IDs
Marcel Abraș – https://orcid.org/0000-0003-2640-978X
Ecaterina Pasat - https://orcid.org/0000-0002-7737-9077
Maria-Magdalena Vicol - https://orcid.org/0009-0007-8126-6140
Cătălina Ciorici - https://orcid.org/0009-0003-7022-6857
Daniela Bursacovscihi - https://orcid.org/0000-0001-7530-3012
References
McConkey HZR, Marber M, Chiribiri A, Pibarot P, Redwood SR, Prendergast BD. Coronary microcirculation in aortic stenosis: a physiological hornets’ nest. Circ Cardiovasc Interv. 2019;12(8):e007470. doi: 10.1161/CIRCINTERVENTIONS.118.007547.
Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 2022;43(7):561-632. doi: 10.1093/eurheartj/ehab395.
Bottaro G, Zappulla P, Deste W, Famà F, Agnello F, Trovato D, et al. Severe aortic valve stenosis: symptoms, biochemical markers, and global longitudinal strain. J Cardiovasc Echogr. 2020;30(3):154-61. doi: 10.4103/jcecho.jcecho_13_20.
Ancona R, Comenale Pinto S. Epidemiology of aortic valve stenosis (AS) and of aortic valve incompetence (AI): is the prevalence of AS/AI similar in different parts of the world? e-J Cardiol Pract. [Internet] 2020;18(10) [cited 2025 May 23]. Available from: https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volu…
Lønborg J, Jabbari R, Sabbah M, Veien KT, Niemelä M, Freeman P, et al. PCI in patients undergoing transcatheter aortic-valve implantation. N Engl J Med. 2024;391(23):2189-200. doi: 10.1056/NEJMoa2401513.
Michail M, Davies JE, Cameron JD, Parker KH, Brown AJ. Pathophysiological coronary and microcirculatory flow alterations in aortic stenosis. Nat Rev Cardiol. 2018;15(7):420-31. doi: 10.1038/s41569-018-0011-2.
Ahn JH, Kim SM, Park SJ, Jeong DS, Woo MA, Jung SH, et al. Coronary microvascular dysfunction as a mechanism of angina in severe aortic stenosis. J Am Coll Cardiol. 2016;67(12):1412-22. doi: 10.1016/j.jacc.2016.01.013
Zelis JM, Tonino PAL, Pijls NHJ, De Bruyne B, Kirkeeide RL, Gould KL, et al. Coronary microcirculation in aortic stenosis: pathophysiology, invasive assessment, and future directions. J Interv Cardiol. 2020;2020:1-13. doi: 10.1155/2020/4603169.
Libby P, Bonow RO. Braunwald’s heart disease: a textbook of cardiovascular medicine. 11th ed. Philadelphia: Elsevier; 2022.
Lee HJ, Lee H, Kim SM, Park JB, Kim EK, Chang SA, et al. Diffuse myocardial fibrosis and diastolic function in aortic stenosis. JACC Cardiovasc Imaging. 2020;13(12):2561-72. doi: 10.1016/j.jcmg.2020.07.007.
Canty JM, Weil BR. Interstitial fibrosis and diastolic dysfunction in aortic stenosis. JACC Basic Transl Sci. 2020;5(5):481-3. doi: 10.1016/j.jacbts.2020.03.014.
Valvo R, Costa G, Tamburino C, Barbanti M. Coronary artery cannulation after transcatheter aortic valve implantation. EuroIntervention. 2021;17(10):835-47. doi: 10.4244/EIJ-D-21-00158.
Nagueh SF, Smiseth OA, Appleton CP, Byrd BF, Dokainish H, Edvardsen T, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update. J Am Soc Echocardiogr. 2016;29(4):277-314. doi: 10.1016/j.echo.2016.01.011.
Otto CM, Prendergast B. Aortic-valve stenosis: from patients at risk to severe valve obstruction. N Engl J Med. 2014;371(8):744-56. doi: 10.1056/NEJMra1313875.
Klein AL, Ramchand J, Nagueh SF. Aortic stenosis and diastolic dysfunction: partners in crime. J Am Coll Cardiol. 2020;76(24):2952-5. doi: 10.1016/j.jacc.2020.10.034.
Wenaweser P, Pilgrim T, Guerios E, Stortecky S, Huber C, Khattab AA, et al. Impact of coronary artery disease and PCI on outcomes in patients with severe aortic stenosis undergoing TAVI. EuroIntervention. 2011;7(5):541-8. doi: 10.4244/EIJV7I5A89.
Hong D, Lee SH, Shin D, Choi KH, Kim HK, Ha SJ, et al. Prognostic impact of cardiac diastolic function and coronary microvascular function on cardiovascular death. J Am Heart Assoc. 2023;12(3):e027690. doi: 10.1161/JAHA.122.027690.
Wada T, Shiono Y, Honda K, Higashioka D, Taruya A, Takahata M, et al. Serial changes of coronary flow reserve over one year after transcatheter aortic valve implantation in patients with severe aortic stenosis. Int J Cardiol Heart Vasc. 2022;42:101090. doi: 10.1016/j.ijcha.2022.101090.
Suzuki W, Nakano Y, Ando H, Fujimoto M, Sakurai H, Suzuki M, et al. Association between coronary flow and aortic stenosis during transcatheter aortic valve implantation. ESC Heart Fail. 2023;10(3):2031-41. doi: 10.1002/ehf2.14316.
Takagi H, Hari Y, Nakashima K, Yokoyama Y, Ueyama H, Kuno T, et al. Baseline left ventricular diastolic dysfunction affects midterm mortality after transcatheter aortic valve implantation. J Card Surg. 2020;35(3):536-43. doi: 10.1111/jocs.14409.
Angellotti D, Manzo R, Castiello DS, Immobile Molaro M, Mariani A, Iapicca C, et al. Echocardiographic evaluation after transcatheter aortic valve implantation: a comprehensive review. Life (Basel). 2023;13(5):1079. doi: 10.3390/life13051079.
ElGuindy A. PARTNER 2A & SAPIEN 3: TAVI for intermediate-risk patients. Glob Cardiol Sci Pract. 2016;2016(4):e201633. doi: 10.21542/gcsp.2016.33.