
Introduction
Because the Earth turns on its axis every 24 hours, almost all life on the planet has a mechanism – circadian rhythmicity – to anticipate the daily changes caused by this rotation. The molecular clocks that control circadian rhythms are being revealed as important regulators of physiology and disease. In humans, circadian rhythms have been studied extensively in the cardiovascular system. Many cardiovascular functions, such as endothelial function, thrombus formation, blood pressure, and heart rate, are now known to be regulated by the circadian clock. Additionally, the onset of acute myocardial infarction, stroke, arrhythmias and other adverse cardiovascular events shows circadian rhythmicity [1].
The circadian clock evolved in diverse organisms to integrate external environmental changes with internal physiology. The clock endows the host with temporal precision and robust adaptation to the surrounding environment. When circadian rhythms are perturbed or misaligned–as a result of jet lag, shift work, or other lifestyle factors–adverse health consequences arise, and the risks of diseases such as cancer, cardiovascular diseases, or metabolic disorders increase. Although the negative impact of circadian rhythm disruption is now well established, how to take advantage of biological timing, or correct it for health benefits, remains underappreciated [2].
The circadian clock is an evolutionarily conserved biological system that coordinates physiological and behavioral processes in a 24-hour rhythm, enabling organisms to anticipate and adapt to daily environmental changes, such as the light-dark cycle [3, 4]. At its core, the circadian rhythm is governed by a network of molecular clocks, with the suprachiasmatic nucleus (SCN) in the hypothalamus serving as the central pacemaker that synchronizes peripheral clocks located in virtually all tissues, including the heart, blood vessels, and kidneys [5-7]. The circadian rhythm, orchestrated by the SCN, synchronizes body-wide clocks through neural and hormonal pathways. Light signals, detected by specialized retinal cells, travel via the retinohypothalamic tract to the SCN, initiating a cascade through the paraventricular nucleus (PVN), brainstem, and spinal cord to the pineal gland. The molecular machinery of the circadian clock involves a set of core clock genes, including CLOCK, which operate via transcriptional-translational feedback loops (TTFLs) to regulate the expression of clock-controlled genes (CCGs) that influence diverse physiological processes [3, 8]. This intricate system ensures temporal coordination of cardiovascular functions, such as blood pressure, heart rate, and endothelial function, which exhibit robust diurnal variations [9, 10-12]. For instance, blood pressure typically dips during sleep and rises in the early morning, a pattern regulated by the interplay between the SCN and peripheral clocks in the cardiovascular system (CVS) [13, 14-16]. Disruption of these rhythms, as seen in shift workers or individuals with sleep disorders, has been epidemiologically linked to an increased risk of cardiovascular disease (CVD), including hypertension, myocardial infarction (MI), and atherosclerosis [17, 18]. Studies have shown that circadian misalignment can lead to dysregulation of the autonomic nervous system (ANS), impaired glucose metabolism, and increased systemic inflammation, all of which contribute to CVD pathogenesis [19, 20-22]. Evidently, the circadian rhythm is a crucial conduit between the brain and the heart.
The objective of this narrative review is to synthesize the current scientific evidence on the regulation of cardiovascular physiology by circadian rhythms and the consequences of their disruption in disease states. Specifically, we aim to: (1) delineate the molecular and physiological mechanisms linking central and peripheral circadian clocks to key cardiovascular functions (blood pressure, heart rate, endothelial function, coagulation, and autonomic tone); (2) analyze the contributions of extrinsic (e.g., shift work, irregular light exposure, altered feeding schedules) and intrinsic (e.g., aging, inflammation, genetic clock-gene variants) factors to circadian misalignment and its associated cardiovascular morbidity and mortality; and (3) discuss the clinical implications of these disruptions for critically ill patients in intensive care, including the potential value of chronotherapeutic strategies and circadian-aligned environmental interventions.
Materials and methods
A comprehensive bibliographic search was initiated to conduct a narrative literature review synthesizing current scientific evidence regarding circadian rhythm disruption and its effects on cardiovascular regulation in critically ill patients. The review followed the general principles of systematic literature analysis to identify, select, and evaluate relevant studies addressing circadian mechanisms and their clinical implications in intensive care settings. The search was performed across electronic databases, including PubMed, Scopus, and Web of Science, and was limited to studies published between 2000 and 2025. The following keywords and their combinations were used: circadian rhythm, circadian disruption, blood pressure variability, cardiovascular regulation, critical illness, intensive care unit, chronobiology, and hemodynamic instability. Additionally, the reference lists of relevant publications were manually screened to identify further studies that met the inclusion criteria. Studies were considered eligible if they addressed circadian rhythm physiology, mechanisms of circadian regulation, circadian disruption in intensive care environments, or the relationship between circadian rhythms and cardiovascular function.
The following types of publications were included:
clinical studies
experimental studies
observational studies
relevant review articles
Studies were excluded if they:
were not published in English
lacked relevance to the topic of circadian rhythm and cardiovascular regulation
did not include data or discussion related to critically ill patients or cardiovascular physiology.
The identified articles were initially screened based on their titles and abstracts. Publications that appeared relevant were further assessed through full-text evaluation. Studies meeting the eligibility criteria were included in the final analysis. Relevant information from the selected studies was extracted, including:
study objectives
study design
investigated circadian parameters
cardiovascular outcomes
major findings related to circadian rhythm disturbances.
The extracted data were organized and analyzed to identify key themes related to circadian regulation and cardiovascular instability in critically ill patients. The findings from the selected studies were qualitatively synthesized to provide an integrated overview of the current understanding of circadian rhythm disruption and its clinical implications in intensive care medicine. As this study represents a review of previously published literature, no original statistical analyses were performed; instead, the results from the included studies were analyzed descriptively. Because this study is based exclusively on previously published scientific literature, ethical approval and informed consent were not required.
The literature search identified 276 records through database searching across PubMed, Scopus, and Web of Science. After screening titles and abstracts, 197 studies were excluded due to a lack of relevance, insufficient data, or non-English language. A total of 82 full-text articles were assessed for eligibility and included in the final review (Fig. 1).
Results
It is undeniable that the circadian orchestration of biological processes is fundamental for both health and disease. During pathological conditions, circadian orchestration is often perturbed, and the disruption of normal rhythms in healthy organisms leads to pathology. Acknowledgment of these principles has led to the concept that perhaps circadian clocks and biology might be targeted for cardiovascular disease treatment [23]. Disruption of normal circadian rhythms, whether through behavioral, environmental, or genetic means, is detrimental in both humans and animal models, leading to an increased risk of pathologies, including cardiovascular disease. Similarly, whole-body circadian rhythmicity is attenuated with age, in association with increased disease risk [24]. Taken together, such observations suggest that the maintenance of normal circadian biology is critical for prevention of disease and maximizing longevity [23]. The master biological clock, known as the central clock, is located in the suprachiasmatic nucleus (SCN) in the hypothalamus [25].The central clock is essentially involved in adjusting circadian variations in physiological function by regulating the autonomic nervous system, humoral mediators, and other systemic signals. In addition to the central clock in the SCN, each peripheral organ and cell also possesses circadian expression of core clock genes; these are referred to as peripheral clocks. The molecular mechanisms of peripheral clocks are believed to be identical to those of the central clock [26]. The factors that can reset and affect the phase of the internal clock are called zeitgebers (timekeepers). Light is established as the main zeitgeber for the central clock. In contrast, the specific zeitgebers for peripheral clocks are not yet fully elucidated. The discovery of the appropriate zeitgeber for each organ is required to establish novel therapeutic approaches considering time-of-day treatment, namely chronotherapy [27].
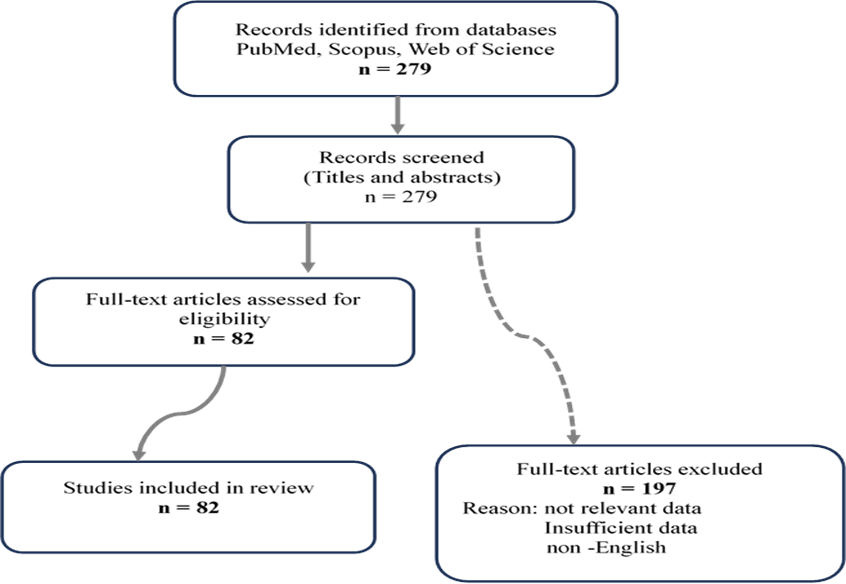 |
Fig. 1 PRISMA 2020 flow diagram of the literature search and study selection process Note: The literature search identified 276 records through database searching (PubMed, Scopus, and Web of Science). After screening titles and abstracts, 197 studies were excluded due to a lack of relevance, insufficient data, or non-English language. A total of 82 full-text articles were assessed for eligibility and included in the final review. |
The circadian mechanism underlies daily rhythms in cardiovascular physiology, and rhythm disruption is a major risk factor for heart disease and worse outcomes. However, the role of circadian rhythms is generally clinically unappreciated [28]. These rhythms drive daily variations in key parameters, including heart rate [29], blood pressure [30], and cardiac contractility [31]. Circadian rhythm disruption is a major risk factor for cardiovascular disease and is associated with severe health consequences. [32, 33]. Recently, there have been major advances in our understanding of daily rhythmicity and its relevance to the pathogenesis and treatment of cardiac hypertrophy and heart failure [31, 34, 35].
Because circadian rhythms display oscillating patterns, developing treatments that can take advantage of this biological governance holds great therapeutic value. Hence, a crucial therapeutic approach involves mitigating risks during periods of highest vulnerability in the circadian cycle, or reinstating typical circadian phase and amplitude patterns [36].
Circadian rhythms, regulated by the suprachiasmatic nucleus in the brain, profoundly influence cardiovascular health through intricate neurobiological mechanisms. These rhythms regulate gene expression in cardiomyocytes, modulate autonomic nervous system (ANS) activity, and synchronize cardiovascular functions with environmental cues, ultimately impacting heart rate, blood pressure, and susceptibility to cardiac events. The intricate relationship between circadian rhythms and cardiovascular health emphasizes the critical role of brain-heart communication in physiological processes [37].
Peripheral clocks in cardiovascular tissues. Peripheral clocks in cardiovascular tissues play a crucial role in regulating circadian rhythms of cardiovascular function, working in concert with the central clock in the SCN [3, 38, 39]. In the heart, cardiomyocytes exhibit rhythmic expression of core clock genes and CCGs, with up to 10 % of the cardiac transcriptome showing circadian oscillations [40]. These oscillations regulate critical cardiac functions, such as the expression of ion channels like Kv1.5, Kv4.2, and Scn5a, which are involved in cardiac electrophysiology [41, 42]. The peripheral clock in blood vessels also demonstrates circadian rhythmicity, with smooth muscle BMAL1 participating in blood pressure regulation [13, 43]. Beesley et al. conducted an intriguing study to explore how circadian rhythms affect heart function in mice cardiomyocytes. They found that the circadian clock gene expression of PER2 in cardiomyocytes is cell-autonomous and can be amplified by β-adrenergic signaling, suggesting how circadian rhythms are regulated in cardiomyocytes and their potential implications for cardiac function [44]. Endothelial cells, crucial for vascular homeostasis, exhibit circadian control over coagulation factors like plasminogen activator inhibitor-1 (PAI-1) and thrombomodulin, as well as cell cycle regulators Ccna1 and Cdk1 [40, 45, 46]. The interaction between central and peripheral clocks is complex, with the SCN playing a central role in the synchronization of peripheral clocks through neural and humoral signals [47, 48]. However, peripheral clocks can also be affected by local zeitgebers, such as food intake and physical activity, allowing for tissue-specific temporal organization [46, 49, 50]. This intricate network of central and peripheral clocks enables the CVS to anticipate and adapt to daily environmental changes. The SCN affects peripheral clocks via the SNS, while hormones like T3 and neurotransmitters such as VIP fine-tune cardiac rhythms. Voltage-gated calcium channels (VGCCs) play a crucial role in translating circadian signals into functional cardiac outputs [40, 51]. Disruption of this synchronization, either between the central clock and peripheral clocks or among different peripheral clocks, can lead to cardiovascular dysfunction [52]. For instance, cardiomyocyte-specific deletion of the Bmal1 gene results in a slower heart rate and increased susceptibility to arrhythmias [41, 53, 54]. Moreover, desynchronization between internal clocks and the external environment, as seen in shift work or irregular social schedules, has been associated with an increased risk of cardiovascular diseases [20, 46]. Understanding the molecular mechanisms underlying these peripheral clocks and their interaction with the central clock is crucial for developing novel therapeutic approaches to manage cardiovascular disorders and optimize treatment timing, a concept known as chronotherapy [41, 46, 55, 56].
Mechanism of circadian disruption causing cardiovascular diseases. Studies have shown that major cardiovascular events, such as acute myocardial infarction, sudden cardiac death, and stroke, occur more frequently at certain times of the day – particularly in the early morning – suggesting a dysfunctional circadian regulation. Disruption of circadian rhythms has been associated with resistant hypertension, endothelial dysfunction, and chronic vascular inflammation, all of which contribute to the progression of cardiovascular disease.
Circadian disruption broadly refers to multiple types of circadian clock disturbances, including circadian misalignment [57] and circadian desynchrony [58] or desynchronization [59]. These disturbances can manifest across various biological levels, from cellular and tissue scales to organismal and systemic scales. Circadian misalignment is a mismatch between an individual’s internal circadian clock and their external environment or social schedule. Circadian desynchrony or desynchronization both refer to a variance in the cycles of 2 or more rhythms. Both concepts can be quantified by measuring the phase angle differences and comparing the estimated durations of the rhythms [60].
Circadian disruption significantly impacts cardiovascular health through multiple interconnected mechanisms (Table 1). Dysregulation of ANS activity is a key factor, as evidenced by altered heart rate variability and blood pressure patterns in individuals experiencing circadian misalignment [20, 41, 46]. This disruption can lead to prolonged QTc intervals (the time from the start of the Q wave to the end of the T wave on an electrocardiogram (ECG), measuring ventricular depolarization and repolarization) and increased susceptibility to arrhythmias, particularly in shift workers [38, 46]. Impaired metabolic and hormonal rhythms also play a crucial role in associating circadian disruption with CVD. Cortisol and melatonin, two hormones with strong circadian patterns, are particularly affected. Disrupted cortisol rhythms can lead to increased inflammation and metabolic dysfunction, while altered melatonin secretion due to light exposure at night can impact sleep quality and cardiovascular function [50, 61, 62].
Table 1. Effects of circadian clock gene dysregulation on cardiovascular function | ||
Clock gene manipulation | Cardiovascular effects | References |
| Bmal1 knockout | Arrhythmic behaviour, loss of circadian rhythms in peripheral tissues, reduced lifespan | Haque et al., 2019 |
| Per2 mutation | Impaired endothelium-dependent relaxation, decreased nitric oxide production | Viswambharan et al., 2007 |
| SCN-specific Bmal1 knockout | Loss of circadian behavioural rhythms while peripheral clocks remain rhythmic | Haque et al., 2019 |
| Astrocyte-specific Bmal1 knockout | Delayed activity onset and slower entrainment to new light–dark cycles | Haque et al., 2019 |
| Ventral forebrain Bmal1 knockout | Altered timing of circadian behavioural patterns | Haque et al., 2019 |
| Per2 knockout in cardiomyocytes | Increased cell death and mitochondrial dysfunction under stress | Bhaskara et al., 2024 |
| VSMC Bmal1 knockout | Aggravated atherosclerotic lesions, increased VSMC migration, ROS levels, and apoptosis | Lin et al., 2022 |
| Postnatal cardiomyocyte Bmal1 knockout | Increased cardiac hypertrophy and fibrosis; pressure overload-induced cardiac remodeling | Liang et al., 2022 |
| Per1 knockout | Circadian rhythm desynchronization and increased salt-sensitive hypertension | Zietara et al., 2022 |
| Note: VSMC – vascular smooth muscle cells; ROS – reactive oxygen species; SCN – suprachiasmatic nucleus; BMAL1 – Brain and Muscle ARNT-Like 1, a core component of the circadian clock transcription–translation feedback loop; PER1 / PER2 – Period genes (Period Circadian Regulator 1 and 2), essential components of the negative feedback loop regulating circadian rhythms. | ||
Oxidative stress and inflammation are exacerbated by circadian disruption, contributing significantly to CVD risk. Studies have shown that circadian rhythm disruption impairs tissue homeostasis and exacerbates chronic inflammation [39, 50, 63, 64]. Circadian dysregulation is intricately correlated to various cardio-vascular conditions, highlighting the critical role of the body’s internal clock in maintaining cardiovascular health. The onset of cardiovascular disease (CVD) exhibits a diurnal oscillation; for example, acute coronary syndrome or atrial fibrillation often occurs in the early morning (Table 2).
In addition to disease onset, several cardiac functions also show circadian variation, including heart rate (HR) and blood pressure (BP). Recent evidence supports the idea that the diurnal variation of cardiovascular physiology and pathology is tightly related to an intrinsic biological rhythm, named the circadian clock [27].
| Table 2. Common onset time of cardiovascular events. | |
| Disease | Onset time |
Acute myocardial infarction Cerebral infarction Subarachnoid hemorrhage Atrial fibrillation Ventricular tachycardia/fibrillation | Early morning Morning Daytime Morning/night Morning |
Diurnal variation and chronotherapy in blood pressure/hypertension. It is well known that there is a 24-hour variation in BP with a distinct peak in the morning. This daily variation in BP is considered representative of both intrinsic and exogenous factors. Intrinsic factors include autonomic nervous system activity and humoral factors such as cortisol, renin, aldosterone, vasoactive intestinal peptide, and ANP [65]. Conversely, exogeneous factors such as physical activity, emotional state, meals, and sleep-wake states also profoundly affect BP variations. In normal subjects, the nocturnal BP decline of less than 10-20%, and these individuals are termed “normal dippers”. Persons with a nocturnal decline of less than 10% are classified as “non-dippers”. Some subjects can be classified as “extreme dippers” (a decline greater than 20%), while others present as “inverse dippers” or “risers” (a decline less than 0%), indicating that their asleep BP is higher than their awake BP (Table 3) [27].
| Table 3. Indices of diurnal blood pressure (BP) decline. | |
| BP Dipping Classification | Nocturnal BP decline ratio |
Normal dipper Non-dipper Extreme dipper Inverse dipper/ riser | 10—20% <10% >20% <0% |
Note: [(Mean SBP awake − Mean SBP asleep)/Mean SBP awake] × 100. | |
Loss of adequate BP decline during the sleep period may be a significant risk factor for cardiovascular organ damage. Hypertensive patients with the non-dipper BP pattern are found to be more susceptible to heart and kidney damage [66]. Patients with a non-dipper BP profile have a higher risk than dipper patients for left ventricular hypertrophy, heart failure, myocardial infarction, stroke, albuminuria, and progression to end-stage renal disease [65]. Non-dipper normotensive patients exhibit an equivalent hazard ratio for cardiovascular mortality compared to dipper hypertensive patients [66]. Inverse-dipper or riser patients also demonstrate a significantly higher incidence of stroke compared with those with other patterns of BP variation, suggesting that patients with this BP profile carry the highest overall risk for cardiovascular events [67, 68]. Considering the heterogeneity of BP profiles, it is clinically inappropriate to treat all hypertensive patients with the same regimen. Currently, more than 80% of hypertensive patients take all of their anti-hypertensive medications in the morning. Therefore, it is becoming a physician’s responsibility personalize treatment according to a patient’s specific diurnal BP profile. Chronotherapy aims to provide treatment with maximum beneficial effects and minimal adverse effects by aligning drug delivery with the intrinsic circadian rhythm of disease processes or symptoms. Chronotherapy with antihypertensive medication can be successfully achieved by adjusting the administration time within a 24-hour cycle [27, 69].
Circadian rhythm in acute coronary syndrome. The onset of acute myocardial infarction (AMI) or pulmonary embolism demonstrates a clear circadian variation with a peak in the early morning [70, 71]. A number of cardiac functions related to the pathogenesis of myocardial infarction are known to exhibit circadian variation. Even the shift to daylight saving time in the spring could influence the onset of AMI; during the first 3 weeks after this seasonal transition, the incidence of AMI significantly increases [72].
The diurnal variation in autonomic nervous system activity could account for the circadian onset of AMI. In the early morning, systolic BP and HR increase, resulting in an elevated myocardial oxygen demand. Conversely, the vascular tone of the coronary arteries rises, and coronary blood flow decreases during morning hours. This mismatch between myocardial oxygen demand and supply in the morning appears to trigger the circadian onset of AMI. Interestingly, of the morning peak in AMI onset is blunted in patients receiving β-blockers, as well as in diabetic patients with autonomic neuropathy, highlighting the central role of autonomic nervous system signaling in driving this diurnal variation [73]. In addition, a state of hypercoagulability in the morning may underlie the circadian onset of AMI. Circulating platelet counts and platelet aggregation pathways fluctuate in a circadian fashion [74]. Because platelets are activated by catecholamines, the rhythmic activation of the autonomic nervous system can induce corresponding oscillations in platelet activity. The coagulation activity also has a circadian variation. The plasma concentration of factor VII, the elevation of which is known as a risk factor for coronary artery disease, exhibits a diurnal oscillation [75]. Other coagulation-related factors, such as fibrinogen, prothrombin, factor VIII, and tissue factor pathway inhibitor also exert circadian activation [76]. The coagulation process can be counterbalanced by activation of the fibrinolytic pathway, which attenuates the coagulation processes and prevents thrombosis. The fibrinolytic function, however, decreases in the morning. Tissue plasminogen activator inhibitor-1 (PAI-1) regulates the activity of tissue plasminogen activator (t-PA), thus strongly influencing fibrinolytic activity. The concentration and activity of PAI-1 were noted to oscillate in a circadian pattern with a peak in the morning, resulting in lower t-PA activity during the morning. Therefore, the efficacy of t-PA therapy to restore the patency of occluded vessels in AMI patients is time-dependent [77]. As such, the circadian variation of PAI-1 activity seems to be strongly related to the morning decrease in fibrinolytic activity [27].
Sudden cardiac arrest is a malfunction of the heart’s electrical system, typically caused by ventricular arrhythmias, that can lead to sudden cardiac death (SCD) within minutes. Epidemiological studies have shown that SCD and ventricular arrhythmias are more likely to occur in the morning than in the evening, and laboratory studies indicate that these daily rhythms in adverse cardiovascular events are at least partially under the control of the endogenous circadian timekeeping system. However, the biophysical mechanisms linking molecular circadian clocks to cardiac arrhythmogenesis are not fully understood [78].
The biophysical mechanisms underlying these daily rhythms in adverse cardiovascular events are not fully understood. The master circadian (24-hour) pacemaker in the hypothalamus, the suprachiasmatic nucleus (SCN), influences a variety of cardiovascular phenomena by coordinating daily rhythms in the release of hormones and other circulating molecules. Recently, it has been demonstrated that circadian clocks within heart muscle cells (cardiomyocytes) also regulate rhythms in cardiac electrophysiology [79].
Normal circadian organization is critical for maintaining homeostasis, and a disturbance of this rhythm can induce the progression of organ damage. Therefore, the dysregulation of the circadian rhythm can induce the development of cardiac diseases. Moreover, reversal of the deregulated circadian rhythm or resynchronization of individual tissue clocks may become a promising therapeutic target to prevent disease progression [27].
Discussion
The present review highlights the role of circadian regulation in cardiovascular physiology and its clinical implications in critically ill patients. Our findings support the concept that circadian blood pressure variability represents not only a physiological phenomenon but also a potential marker of systemic integrity and adaptive capacity. At the molecular level, circadian clock genes regulate myocardial metabolism, electrophysiological stability, endothelial function, and vascular tone. Disruption of these mechanisms contributes to autonomic imbalance, oxidative stress, inflammatory activation, and prothrombotic states. These pathophysiological pathways provide a biological explanation for the well-documented morning predominance of acute myocardial infarction, stroke, and malignant arrhythmias. Chronotherapeutic strategies, including time-adjusted antihypertensive administration and structured environmental light management, have demonstrated benefits in non-ICU populations. However, evidence in critically ill patients remains limited. Prospective, multicenter studies are required to determine whether modulation of circadian patterns can improve survival and reduce cardiovascular complications in this vulnerable group [67, 72].
Several limitations should be acknowledged. The design of the reviewed studies restricts causal inference, and circadian assessment was limited to hemodynamic parameters without biochemical phase markers such as melatonin or cortisol. Additionally, standardized protocols for circadian monitoring in ICU practice are not yet established. Despite these limitations, the results support the hypothesis that preserved circadian variability reflects better physiological regulation and an improved prognosis.
The extrinsic and intrinsic factors discussed above acquire particular relevance in the intensive care environment, where multiple timers are simultaneously disrupted [79].
The study selection process, illustrated in the PRISMA 2020 flow diagram (Figure 1), enhances transparency and methodological rigor in the identification and inclusion of relevant studies. Several limitations should be acknowledged. The design of the reviewed studies restricts causal inference, and circadian assessment was limited to hemodynamic parameters without the inclusion of biochemical phase markers such as melatonin or cortisol. Additionally, standardized protocols for circadian monitoring in ICU practice are not yet established. Furthermore, although a comprehensive literature search was performed using major databases, along with language and full-text availability filters, no formal risk-of-bias assessment was conducted. Therefore, potential selection and publication biases cannot be fully excluded. The heterogeneity of the included studies in terms of design, patient populations, and outcome measures may also limit the generalizability of the findings.
Conclusions
The circadian system plays a vital role in regulating various physiologic processes. The way the body responds to injury is often dependent on the interaction of the injury with the circadian machinery. Circadian rhythms are frequently disrupted in patients in the ICU, and there are a number of factors that likely contribute to this breakdown. Practices leading to circadian rhythm optimization may improve patient outcomes, and the implementation of these practices should be incorporated into ICU care. Circadian rhythm disruption plays a significant role in cardiovascular pathology and is particularly relevant in critically ill patients. Incorporating circadian assessment into clinical evaluation may enhance prognostic accuracy and open new perspectives for individualized therapeutic timing in intensive care medicine.
Competing interests
None declared.
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer reviewed.
Author’s ORCID ID
Iraida Camerzan – https://orcid.org/0000-0002-1831-6180
References
Crnko S, Du Pré BC, Sluijter JPG, Van Laake LW. Circadian rhythms and the molecular clock in cardiovascular biology and disease. Nat Rev Cardiol. 2019;16(7):437-447. doi: 10.1038/s41569-019-0167-4.
Wei R, Yuan X, Eltzschig HK. Circadian rhythm as a therapeutic target. Nat Rev Drug Discov. 2021;20(4):287-307. doi: 10.1038/s41573-020-00109-w.
Bass J, Lazar MA. Circadian time signatures of fitness and disease. Science. 2016;354(6315):994-999. doi: 10.1126/science.aah4965.
Takahashi JS. Transcriptional architecture of the mammalian circadian clock. Nat Rev Genet. 2017;18(3):164-179. doi: 10.1038/nrg.2016.150.
Koronowski KB, Sassone-Corsi P. Communicating clocks shape circadian homeostasis. Science. 2021;371(6530): eabd0951. doi: 10.1126/science.abd0951.
Hastings MH, Maywood ES, Brancaccio M. Generation of circadian rhythms in the suprachiasmatic nucleus. Nat Rev Neurosci. 2018;19(8):453-469. doi: 10.1038/s41583-018-0026-z.
Mohawk JA, Green CB, Takahashi JS. Central and peripheral circadian clocks in mammals. Annu Rev Neurosci. 2012;35(1):445-462. doi: 10.1146/annurev-neuro-060909-153128.
Pilorz V, Helfrich-Forster C, Oster H. The role of the circadian clock system in physiology. Pflugers Arch Eur J Physiol. 2018;470(2):227-239. doi: 10.1007/s00424-017-2103-y.
Martino TA, Sole MJ. Molecular time : an often overlooked dimension to cardiovascular disease. Circ Res. 2009;105(11):1047-1061. doi: 10.1161/CIRCRESAHA.109.206201.
Monfredi O, Lakatta EG. Complexities in cardiovascular rhythmicity: perspectives on circadian normality, ageing and disease. Cardiovasc Res. 2019;115(11):1576-1595. doi: 10.1093/cvr/cvz112.
Atkinson G, Jones H, Ainslie PN. Circadian variation in the circulatory responses to exercise: relevance to the morning peaks in strokes and cardiac events. Eur J Appl Physiol. 2010;108(1):15-29. doi: 10.1007/s00421-009-1243-y.
Curtis AM, Cheng Y, Kapoor S, Reilly D, Price TS, Fitzgerald GA. Circadian variation of blood pressure and the vascular response to asynchronous stress. Proc Natl Acad Sci USA. 2007;104(9):3450-3455.doi: 10.1073/pnas.0611680104.
Douma LG, Gumz ML. Circadian clock-mediated regulation of blood pressure. Free Radic Biol Med. 2018;119: 108-114. doi: 10.1016/j.freeradbiomed.2017.11.024.
Smolensky MH, Hermida RC, Portaluppi F. Circadian mechanisms of 24-hour blood pressure regulation and patterning. Sleep Med Rev. 2017; 33:4-16. doi: 10.1016/j.smrv.2016.02.003.
Faraci FM, Scheer FAJL. Hypertension: causes and consequences of circadian rhythms in blood pressure. Circ Res. 2024;134(6):810-832. doi: 10.1161/CIRCRESAHA.124.323515.
Hermida RC, Ayala DE, Fernandez JR, Portaluppi F, Fabbian F, Smolensky MH. Circadian rhythms in blood pressure regulation and optimization of hypertension treatment with ACE inhibitor and ARB medications. Am J Hypertens. 2011;24(4):383-391. doi: 10.1038/ajh.2010.217.
Wong R, Crane A, Sheth J, Mayrovitz HN. Shift work as a cardiovascular disease risk factor: a narrative review. Cureus. 2023;15(6): e41186. doi: 10.7759/cureus.41186.
Vyas MV, Garg AX, Iansavichus AV, Costella J, Donner A, Laugsand LE, Janszky I, Mrkobrada M, Parraga G, Hackam DG. Shift work and vascular events: systematic review and meta-analysis. BMJ. 2012;345: e4800. doi: 10.1136/bmj.e4800.
Chellappa SL, Vujovic N, Williams JS, Scheer FAJL. Impact of circadian disruption on cardiovascular function and disease. Trends Endocrinol Metabol. 2019;30(10):767-779. doi: 10.1016/j.tem.2019.07.008.
Young MJ, Heanue S, Kanki M, Moneghetti KJ. Circadian disruption and its impact on the cardiovascular system. Trends Endocrinol Metabol. 2025;36(9):842-854. doi: 10.1016/j.tem.2024.11.010.
Morris CJ, Purvis TE, Hu K, Scheer FAJL. Circadian misalignment increases cardiovascular disease risk factors in humans. Proc Natl Acad Sci USA. 2016;113(10): E1402-11. doi: 10.1073/pnas.1516953113.
Scheer FAJL, Hilton MF, Mantzoros CS, Shea SA. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc Natl Acad Sci USA. 2009;106(11):4453-4458. doi: 10.1073/pnas.0808180106.
Young ME. The cardiac circadian clock: implications for cardiovascular disease and its treatment. JACC Basic Transl Sci. 2023;8(12):1613-1628. doi: 10.1016/j.jacbts.2023.03.024.
Hood S, Amir S. The aging clock: circadian rhythms and later life. J Clin Invest. 2017;127(2):437-446. doi: 10.1172/JCI90328.
Schibler U. The daily rhythms of genes, cells and organs. Biological clocks and circadian timing in cells. EMBO Rep. 2005;6(Suppl 1): S9-13. doi: 10.1038/sj.embor.7400424.
Oishi K, Sakamoto K, Okada T, Nagase T, Ishida N. Antiphase circadian expression between BMAL1 and period homologue mRNA in the suprachiasmatic nucleus and peripheral tissues of rats. Biochem Biophys Res Commun. 1998;253(2):199-203. doi: 10.1006/bbrc.1998.9779.
Takeda N, Maemura K. Circadian clock and cardiovascular disease. J Cardiol. 2011;57(3):249-56. doi: 10.1016/j.jjcc.2011.02.006.
Alibhai FJ, LaMarre J, Reitz CJ, Tsimakouridze EV, Kroetsch JT, Bolz SS, Shulman A, Steinberg S, Burris TP, Oudit GY, Martino TA. Disrupting the key circadian regulator CLOCK leads to age-dependent cardiovascular disease. J Mol Cell Cardiol. 2017; 105:24-37. doi: 10.1016/j.yjmcc.2017.01.008.
Bray MS, Shaw CA, Moore MW, Garcia RA, Zanquetta MM, Durgan DJ, et al. Disruption of the circadian clock within the cardiomyocyte influences myocardial contractile function, metabolism, and gene expression. Am J Physiol Heart Circ Physiol. 2008;294(2):H1036-H1047. doi: 10.1152/ajpheart.01291.2007.
Podobed P, Pyle WG, Ackloo S, Alibhai FJ, Tsimakouridze EV, Ratcliffe WF, et al. The day/night proteome in the murine heart. Am J Physiol Regul Integr Comp Physiol. 2014;307(2): R121-R137. doi: 10.1152/ajpregu.00011.2014.
Alibhai FJ, Tsimakouridze EV, Reitz CJ, Pyle WG, Martino TA. Consequences of circadian and sleep disturbances for the cardiovascular system. Can J Cardiol. 2015;31(7):860-872. doi: 10.1016/j.cjca.2015.01.015.
Ruger M, Scheer FA. Effects of circadian disruption on the cardiometabolic system. Rev Endocr Metab Disord. 2009;10(4):245-260. doi: 10.1007/s11154-009-9122-8.
Martino TA, Tata N, Simpson JA, Vanderlaan R, Dawood F, Kabir MG, et al. The primary benefits of angiotensin-converting enzyme inhibition on cardiac remodeling occur during sleep time in murine pressure overload hypertrophy. J Am Coll Cardiol. 2011;57(20): 2020-2028. doi: 10.1016/j.jacc.2010.11.022.
Sachan N, Dey A, Rotter D, Grinsfelder DB, Battiprolu PK, Sikder D, et al. Sustained hemodynamic stress disrupts normal circadian rhythms in calcineurin dependent signaling and protein phosphorylation in the heart. Circ Res. 2011; 108(4): 437-445. doi: 10.1161/CIRCRESAHA.110.235309.
Pinotti M, Bertolucci C, Portaluppi F, Colognesi I, Frigato E, Foa A, Bernardi F. Daily and circadian rhythms of tissue factor pathway inhibitor and factor VII activity. Arterioscler Thromb Vasc Biol 2005;25(3):646-9. doi: 10.1161/01.ATV.0000153140.13148.e0.
Thakur A, Kishore R. Neurobiology of the circadian clock and its role in cardiovascular disease:Mechanisms, biomarkers, and chronotherapy. Neurobiol Sleep Circadian Rhythms. 2025;19:100131. doi: 10.1016/j.nbscr.2025.100131.
Meloni M, Setzu D, Del Rio A, Campagna M, Cocco P. QTc interval and electrocardiographic changes by type of shift work. Am J Ind Med. 2013;56(10):1174-1179. doi: 10.1002/ajim.22207.
Csoma B, Bikov A. The role of the circadian rhythm in dyslipidaemia and vascular inflammation leading to atherosclerosis. Int J Mol Sci. 2023;24(18):14145. doi: 10.3390/ijms241814145.
Lecacheur M, Ammerlaan DJM, Dierickx P. Circadian rhythms in cardiovascular (dys)function: approaches for future therapeutics. NPJ Cardiovasc Health. 2024;1(1):21. doi: 10.1038/s44325-024-00024-8.
Richards J, Gumz ML. Mechanism of the circadian clock in physiology. Am J Physiol Regul Integr Comp Physiol. 2013;304(12): R1053-R1064. doi: 10.1152/ajpregu.00066.2013.
Diekman CO, Wei N. Circadian rhythms of early afterdepolarizations and ventricular arrhythmias in a cardiomyocyte model. Biophys J. 2021;120(2):319-333. doi: 10.1016/j.bpj.2020.11.2264.
Crnko S, Cour M, Van Laake LW, Lecour S. Vasculature on the clock: circadian rhythm and vascular dysfunction. Vasc Pharmacol. 2018;108: 1-7. doi: 10.1016/j.vph.2018.05.003.
Xie Z, Su W, Liu S, Zhao G, Esser K, Schroder EA, Lefta M, Stauss HM, Guo Z, Gong MC. Smooth-muscle BMAL1 participates in blood pressure circadian rhythm regulation. J Clin Invest. 2015;125(1):324-336.doi: 10.1172/JCI76881.
Beesley S, Noguchi T, Welsh DK. Cardiomyocyte circadian oscillations are cellautonomous, amplified by β-adrenergic signaling, and synchronized in cardiac ventricle tissue. PLoS One 2016;11(7):e0159618. doi: 10.1371/journal.pone.0159618.
Mieda M. The central circadian clock of the suprachiasmatic nucleus as an ensemble of multiple oscillatory neurons. Neurosci Res. 2020;156:24-31. doi: 10.1016/j.neures.2019.08.003.
Barclay JL, Tsang AH, Oster H. Interaction of central and peripheral clocks in physiological regulation. Prog Brain Res. 2012;199:163-181. doi: 10.1016/B978-0-444-59427-3.00030-7.
Ramkisoensing A, Meijer JH. Synchronization of biological clock neurons by light and peripheral feedback systems promotes circadian rhythms and health. Front Neurol. 2015;6:128. doi: 10.3389/fneur.2015.00128.
Hower IM, Harper SA, Buford TW. Circadian rhythms, exercise, and cardiovascular health. J Circadian Rhythms. 2018;16(1):7. doi: 10.5334/jcr.164.
Xu W, Jain MK, Zhang L. Molecular link between circadian clocks and cardiac function: a network of core clock, slave clock, and effectors. Curr Opin Pharmacol. 2021;57:28-40. doi: 10.1016/j.coph.2020.10.006.
Young ME, Bray MS. Potential role for peripheral circadian clock dyssynchrony in the pathogenesis of cardiovascular dysfunction. Sleep Med. 2007;8(6):656-667. doi: 10.1016/j.sleep.2006.12.010.
Lefta M, Campbell KS, Feng HZ, Jin JP, Esser KA. Development of dilated cardiomyopathy in Bmal1-deficient mice. Am J Physiol Heart Circ Physiol. 2012;303(4):H475-H485. doi: 10.1152/ajpheart.00238.2012.
Schroder EA, Lefta M, Zhang X, Bartos DC, Feng HZ, Zhao Y, Patwardhan A, Jin JP, Esser KA, Delisle BP. The cardiomyocyte molecular clock, regulation of Scn5a and arrhythmia susceptibility. Am J Physiol Cell Physiol. 2013;304(10):C954-C965. doi: 10.1152/ajpcell.00383.2012.
Festus ID, Spilberg J, Young ME, Cain S, Khoshnevis S, Smolensky MH, Zaheer F, Descalzi G, Martino TA. Pioneering new frontiers in circadian medicine chronotherapies for cardiovascular health. Trends Endocrinol Metabol. 2024;35(7):607-623. doi: 10.1016/j.tem.2024.02.011.
Lee Y, Field JM, Sehgal A. Circadian rhythms, disease and chronotherapy. J Biol Rhythm. 2021;36(6):503-531. doi: 10.1177/07487304211044301.
Baron KG, Reid KJ. Circadian misalignment and health. Int Rev Psychiatry. 2014;26(2):139-54. doi: 10.3109/09540261.2014.911149.
Lewy AJ, Sack RL. Exogenous melatonin’s phase-shifting effects on the endogenous melatonin profile in sighted humans: a brief review and critique of the literature. J Biol Rhythms. 1997;12(6):588-94. doi: 10.1177/074873049701200614.
Aschoff J. Circadian rhythms in man. Science. 1965;148(3676):1427-32. doi: 10.1126/science.148.3676.1427.
Lin J, Kuang H, Jiang J, Zhou H, Peng L, Yan X, Kuang J. Circadian rhythms in cardiovascular function: implications for cardiac diseases and therapeutic opportunities. Med Sci Monit. 2023;29:e942215. doi: 10.12659/MSM.942215.
Myung J, Schmal C, Hong S, Tsukizawa Y, Rose P, Zhang Y, Holtzman MJ, De Schutter E, Herzel H, Bordyugov G, Takumi T. The choroid plexus is an important circadian clock component. Nat Commun. 2018;9(1);1062. doi: 10.1038/s41467-018-03507-2.
Ansu Baidoo V, Knutson KL. Associations between circadian disruption and cardiometabolic disease risk: a review. Obesity (Silver Spring). 2023;31(3):615-624. doi: 10.1002/oby.23666.
Orozco-Solis R, Aguilar-Arnal L. Circadian regulation of immunity through epigenetic mechanisms. Front Cell Infect Microbiol. 2020;10:96. doi: 10.3389/fcimb.2020.00096.
Fanjul-Moles ML, Lopez-Riquelme GO. Relationship between oxidative stress, circadian rhythms, and AMD. Oxid Med Cell Longev. 2016;2016(1):7420637. doi: 10.1155/2016/7420637.
Takeda N, Maemura K. Cardiovascular disease, chronopharmacotherapy, and the molecular clock. Adv Drug Deliv Rev. 2010;62:956-66. doi: 10.1016/j.addr.2010.04.011.
Verdecchia P, Porcellati C, Schillaci G, Borgioni C, Ciucci A, Battistelli M, Guerrieri M, Gatteschi C, Zampi I, Santucci A, Reboldi G. Ambulatory blood pressure: an independent predictor of prognosis in essential hypertension. Hypertension. 1994;24(6):793-801. doi: 10.1161/01.hyp.24.6.793.
Ohkubo T, Hozawa A, Yamaguchi J, Kikuya M, Ohmori K, Michimata M, Matsubara M, Hashimoto J, Hoshi H, Araki T, Tsuji I, Satoh H, Hisamichi S, Imai Y. Prognostic significance of the nocturnal decline in blood pressure in individuals with and without high 24-h blood pressure: the Ohasama study. J Hypertens. 2002;20(11):2183-9. doi: 10.1097/00004872-200211000-00017.
Kario K, Pickering TG, Matsuo T, Hoshide S, Schwartz JE, Shimada K. Stroke prognosis and abnormal nocturnal blood pressure falls in older hypertensives. Hypertension. 2001;38(4):852-7. doi: 10.1161/hy1001.092640.
Hermida RC, Ayala DE, Calvo C, Portaluppi F, Smolensky MH. Chronotherapy of hypertension: administration-timedependent effects of treatment on the circadian pattern of blood pressure. Adv Drug Deliv Rev. 2007;59(9-10):923-39. doi: 10.1016/j.addr.2006.09.021.
Staessen JA, Thijs L, Fagard R, O’Brien ET, Clement D, de Leeuw PW, Mancia G, Nachev C, Palatini P, Parati G, Tuomilehto J, Webster J. Predicting cardiovascular risk using conventional vs ambulatory blood pressure in older patients with systolic hypertension. Systolic Hypertension in Europe Trial Investigators. JAMA. 1999;282(6):539-46. doi: 10.1001/jama.282.6.539.
Muller JE, Stone PH, Turi ZG, Rutherford JD, Czeisler CA, Parker C, et al. Circadian variation in the frequency of onset of acute myocardial infarction. N Engl J Med. 1985;313(21):1315-22. doi: 10.1056/NEJM198511213132103.
Janszky I, Ljung R. Shifts to and from daylight saving time and incidence of myocardial infarction. N Engl J Med. 2008;359(18):1966-8. doi: 10.1056/NEJMc0807104.
Willich SN, Linderer T, Wegscheider K, Leizorovicz A, Alamercery I, Schroder R. Increased morning incidence of myocardial infarction in the ISAM Study: absence with prior beta-adrenergic blockade. ISAM Study Group. Circulation. 1989;80(4):853-8. doi: 10.1161/01.cir.80.4.853.
Manfredini R, Boari B, Smolensky MH, Salmi R, la Cecilia O, Maria Malagoni A, Haus E, Manfredini F. Circadian variation in stroke onset: identical temporal pattern in ischemic and hemorrhagic events. Chronobiol Int. 2005;22(3):417-53. doi: 10.1081/CBI-200062927.
Kurnik PB. Circadian variation in the efficacy of tissue-type plasminogen activator. Circulation. 1995;91(5):1341-6. doi: 10.1161/01.cir.91.5.1341.
Muller JE, Ludmer PL, Willich SN, Tofler GH, Aylmer G, Klangos I, Stone PH. Circadian variation in the frequency of sudden cardiac death. Circulation. 1987;75(1):131-138. doi: 10.1161/01.cir.75.1.131.
Willich SN, Levy D, Rocco MB, Tofler GH, Stone PH, Muller JE. Circadian variation in the incidence of sudden cardiac death in the Framingham Heart Study population. Am J Cardiol. 1987;60(10):801-806.doi: 10.1016/0002-9149(87)91027-7.
Kozak M, Krivan L, Semrad B. Circadian variations in the occurrence of ventricular tachyarrhythmias in patients with implantable cardioverter defibrillators. Pacing Clin Electrophysiol. 2003;26(3):731-735. doi: 10.1046/j.1460-9592.2003.00124.x.
Ruwald MH, Moss AJ, Zareba W, Jons C, Ruwald AC, McNitt S, Polonsky B, Kutyifa V. Circadian distribution of ventricular tachyarrhythmias and association with mortality in the MADIT-CRT trial. J Cardiovasc Electrophysiol. 2015;26(3):291-9. doi: 10.1111/jce.12592.
Black N, D'Souza A, Wang Y, Piggins H, Dobrzynski H, Morris G, Boyett MR. Circadian rhythm of cardiac electrophysiology, arrhythmogenesis, and the underlying mechanisms. Heart Rhythm. 2019;16(2):298-307. doi: 10.1016/j.hrthm.2018.08.026.
Jiménez-Pastor JM, Rodríguez-Cortés F, López-Soto P, López-Coleto L, Cruz MME. Cardiorespiratory and circadian clock markers in intensive care unit patients. Dent Med Probl. 2024;61(5):797-801. doi: 10.17219/dmp/191537.