
Introduction
Heart failure (HF) is a complex clinical syndrome defined by the heart’s inability to maintain an adequate cardiac output to meet the body’s metabolic demands, in the presence of elevated filling pressures [1]. The modern classification of HF is based on the left ventricular ejection fraction (LVEF), an echocardiographic indicator of systolic function: heart failure with reduced ejection fraction (HFrEF, ≤40%), heart failure with mildly reduced ejection fraction (HFmrEF, 41–49%), and heart failure with preserved ejection fraction (HFpEF, ≥50%) [1, 2]. HFpEF accounts for approximately half of all HF cases and represents a major diagnostic and therapeutic challenge. The condition predominantly affects women, especially after menopause, due to increased ventricular stiffness, hormonal changes, endothelial dysfunction, and the accumulation of metabolic risk factors [3]. Although patients with HFpEF may have a normal ejection fraction, they typically exhibit elevated filling pressures, diastolic dysfunction, concentric hypertrophy, and reduced ventricular compliance, which limit exercise capacity and cause the characteristic symptoms [4].
A key aspect in the management of HFpEF is the presence of cardiovascular comorbidities, which contribute to the onset and progression of cardiac dysfunction through hemodynamic, inflammatory, and neurohormonal mechanisms. Among these, arterial hypertension, atrial fibrillation, and coronary artery disease are the most significant and frequently encountered [5-7].
Arterial hypertension (HTN) is the most prevalent comorbidity in HFpEF, being identified in over 80% of patients [5, 8]. Chronic exposure to pressure overload leads to concentric left ventricular hypertrophy, myocardial stiffness, impaired active relaxation, and increased diastolic filling pressures [8, 9]. Moreover, endothelial dysfunction and altered vascular reactivity contribute to increased afterload, creating a vicious cycle between arterial and ventricular stiffness [9]. These changes explain why strict blood pressure control plays a crucial role in preventing HFpEF progression and improving symptoms.
Atrial fibrillation (AF) is present in 30–40% of patients with HFpEF and has a bidirectional relationship with diastolic dysfunction [7]. On one hand, the loss of atrial contraction and an inappropriate ventricular rate reduce diastolic filling and cardiac output; on the other hand, elevated filling pressures and atrial remodeling secondary to diastolic dysfunction promote the development and maintenance of AF [6, 10]. The presence of AF is associated with reduced exercise capacity, lower Kansas City Cardiomyopathy Questionnaire (KCCQ) scores, and higher mortality, particularly in elderly patients [10].
Coronary artery disease (CAD) is highly prevalent in HFpEF and manifests in two major forms: obstructive, characterized by significant stenosis or occlusion of the epicardial coronary arteries, and non-obstructive, in which microvascular mechanisms and endothelial dysfunction predominate [11, 12]. The obstructive form leads to chronic myocardial ischemia, ventricular remodeling, and interstitial fibrosis, contributing to increased stiffness and impaired diastolic relaxation [12]. Conversely, non-obstructive CAD, present in a substantial proportion of HFpEF patients (up to 50%), is associated with coronary microvascular dysfunction (CMD), characterized by reduced coronary flow reserve, endothelial inflammation, and oxidative stress [13]. These microvascular alterations impair myocardial perfusion during exercise, increase diastolic stiffness, and limit functional capacity [13, 14]. Microvascular endothelial dysfunction, through reduced nitric oxide (NO) bioavailability and activation of the renin–angiotensin system, promotes chronic inflammation and interstitial remodeling characteristic of HFpEF [14]. Thus, CAD — regardless of its obstructive or non-obstructive nature — represents a central determinant of the ischemic phenotype in HFpEF, influencing both prognosis and treatment response.
Obesity, metabolic syndrome, sleep apnea, and type 2 diabetes mellitus are key elements in the pathogenesis of HFpEF, forming the so-called “cardiometabolic phenotype” [9, 15, 16]. Epicardial adipose tissue (EAT) acts as an active endocrine organ, releasing proinflammatory cytokines (IL-6, TNF-α) that induce local inflammation, oxidative stress, and myocardial fibrosis [9, 15, 17]. Diabetes further contributes through endothelial dysfunction, vascular stiffening, myocardial protein glycosylation, and activation of systemic inflammatory pathways [9]. These processes create a profibrotic and prooxidative milieu that amplifies diastolic dysfunction and reduces the energetic efficiency of cardiomyocytes. Moreover, obesity alters thoracic mechanics, increases intrathoracic pressure, and exacerbates pulmonary congestion, leading to exercise intolerance [9, 15, 16].
Chronic kidney disease (CKD) is another major comorbidity, present in over one-third of HFpEF patients, and is associated with significantly increased mortality [5]. Renal dysfunction activates neurohormonal systems — the Renin-Angiotensin-Aldosterone System (RAAS) and the sympathetic nervous system (SNS) — leading to sodium retention, vasoconstriction, and cardiac remodeling [5, 6]. Cardiorenal syndrome type 2 describes the progressive deterioration of renal function secondary to chronic cardiac dysfunction, perpetuating hemodynamic decompensation and systemic inflammation [5].
The heterogeneity of HFpEF patients arises from the complex interaction between cardiometabolic comorbidities, systemic inflammation, and endothelial dysfunction. Recent studies using cluster or machine learning analyses have identified distinct phenotypic subgroups combining various patterns of HTN, CAD, AF, obesity, and CKD, each with different pathogenic mechanisms and risks for mortality and functional impairment [13-15].
Modern, holistic approaches provide an integrated perspective on these complex interactions, linking molecular, clinical, and functional dimensions of comorbidities in HFpEF [14, 16]. This holistic view enhances understanding of clinical variability and supports the development of personalized treatment strategies.
Therefore, detailed analysis of cardiovascular, metabolic, and renal comorbidities in patients with HFpEF is essential for identifying key prognostic determinants and defining targeted therapeutic strategies. The present study aims to characterize these complex interactions, evaluate the impact of comorbidities on functional status and prognosis, and contribute to the development of an integrated management model for HFpEF.
Materials and methods
This study represents a cross-sectional observational analysis of patients with heart failure with preserved ejection fraction (HFpEF), defined by a left ventricular ejection fraction (LVEF) ≥50%, the presence of signs and symptoms of heart failure, and objective evidence of structural and/or functional cardiac abnormalities consistent with left ventricular diastolic dysfunction and/or elevated left ventricular filling pressures, including elevated natriuretic peptide levels [1]. The main objective was to characterize the clinical, functional, and comorbidity phenotype of patients and to assess the impact of these factors on hemodynamic biomarkers and functional status.
The study cohort included 206 consecutive patients diagnosed with HFpEF, recruited from the General Cardiology Department of the Institute of Cardiology. Inclusion criteria were: age ≥18 years, diagnosis of HFpEF according to the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure [1], availability for complete clinical and paraclinical assessments, and written informed consent. Exclusion criteria included acute heart failure, significant loss of clinical data, presence of severe comorbidities that could interfere with functional evaluation, or inability to participate in standardized testing.
For each patient, demographic data (age, sex), anthropometric data (weight, height, body mass index – BMI), and the medical history of cardiovascular and non-cardiovascular diseases were recorded. BMI was calculated as weight (kg)/height (m²). Sex distribution was coded according to the dataset as follows: 1 = male, 2 = female.
The etiology of HFpEF was classified as follows: documented coronary artery disease, undocumented coronary disease, arterial hypertension, significant valvular disease, tachycardia-induced, idiopathic dilated cardiomyopathy, hereditary/genetic, alcoholic, infectious, pulmonary hypertension without left heart disease, and other rare causes.
Functional class was assessed using the New York Heart Association (NYHA) classification. The biomarker NT-proBNP was measured to evaluate hemodynamic stress and ventricular filling pressures, using standardized laboratory techniques.
Cardiovascular comorbidities included arterial hypertension, atrial fibrillation, myocardial infarction, coronary artery disease, prior revascularization procedures, valvular disease, peripheral vascular disease, stroke/transient ischemic attack, and venous thromboembolism. Non-cardiac comorbidities included diabetes mellitus, chronic obstructive pulmonary disease (COPD), thyroid dysfunction, hepatic dysfunction, sleep apnea, depression, cognitive impairment, active malignancy, and rheumatoid arthritis.
All patients underwent standardized clinical, paraclinical, and functional evaluations, including anthropometric measurements, functional testing (NYHA), NT-proBNP assessment, and detailed medical history collection. No experimental therapeutic interventions were applied, as the study was purely observational.
Data were centralized and validated for consistency and completeness. Continuous variables were described as mean ± standard deviation (SD), median, and interquartile range (IQR). Categorical variables were expressed as frequencies and percentages. The distribution of variables was tested for normality using the Shapiro–Wilk test. Group comparisons were performed using parametric tests (independent t-test) or nonparametric tests (Mann–Whitney U), as appropriate. Relationships between comorbidities, biomarkers, and functional status were analyzed using linear and logistic regression models, with statistical significance set at P < 0.05.
All patients provided written informed consent, and the study protocol was approved by the institutional ethics committee (Approval No. 25/1, May 13, 2025). The study was conducted in accordance with the principles of the Declaration of Helsinki on biomedical research involving human subjects.
Results
The study cohort included 206 patients with HFpEF. The mean age was 65.5 years (SD 9.6), with a median of 66.0 and an interquartile range (IQR) of 59.0–71.0; the age range was 39–94 years, reflecting a typical age profile for heart failure with preserved ejection fraction. Body mass index (BMI) confirmed a phenotype marked by overweight/obesity: mean BMI 29.7 kg/m² (SD 5.1), median 29.22, IQR 26.23–32.74, with extremes ranging from 19.44–54.53 kg/m². Sex distribution, according to dataset coding, was approximately 44.2% male (91/206) and 55.8% female (115/206), showing a slightly female-predominant structure consistent with HFpEF epidemiology.
The etiologic profile was dominated by chronic coronary artery disease and pressure overload (Figure 1). “Undocumented coronary disease (no coronary angiography)” accounted for 32.0% (66/206), followed by “documented coronary disease” 29.1% (60/206), and “arterial hypertension (etiology)” 19.4% (40/206). “Significant valvular disease” occurred in 10.7% (22/206), while other causes (tachycardia-induced, hereditary/genetic, alcoholic, infectious, pulmonary hypertension without left heart disease, idiopathic dilated cardiomyopathy, other rare causes) individually accounted for ≤2.4%.
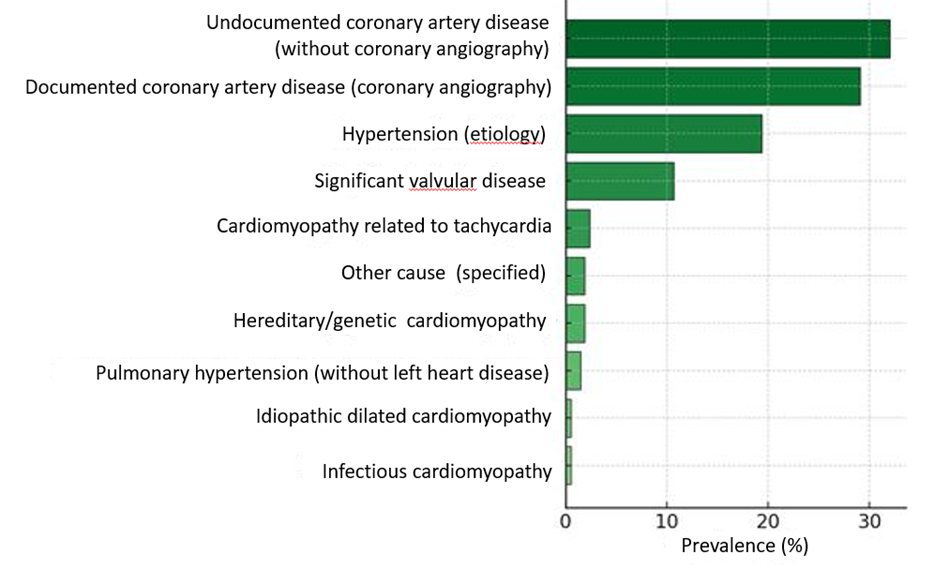 |
Fig. 1 Distribution of HFpEF etiologies. Note: The figure illustrates the prevalence (%) of etiological conditions identified in patients with heart failure with preserved ejection fraction (HFpEF). Data are presented as percentages of the overall study population. The figure presents descriptive data only; no inferential statistical tests were applied. |
This distribution reinforces a phenotype in which “pressure–overload” mechanisms and chronic coronary disease are central, while acute myocardial necrosis is less frequent than in reduced ejection fraction phenotypes.
The hemodynamic stress biomarker showed an expected HFpEF profile. NT-proBNP had a mean of 1,388 pg/mL (SD 2,111), median 863.5 pg/mL, and IQR 562.5–1,454.5 pg/mL (n analyzed = 190, range 50–18,802 pg/mL), indicating elevated filling pressures and significant heterogeneity of load. Functionally, the NYHA distribution (Table 1) was centered on class III, with 88.8% (183/206) in class III and 11.2% (23/206) in class II, reflecting moderate functional limitation in the majority of HFpEF patients.
Table 1. Functional class (NYHA) distribution in HFpEF patients | ||
NYHA class | N | % |
II | 23 | 11.2% |
III | 183 | 88.8% |
Note: Data are presented as absolute numbers (N) and percentages (%). NYHA = New York Heart Association; HFpEF = heart failure with preserved ejection fraction. This table presents descriptive statistics only; no inferential statistical tests were applied. | ||
Cardiovascular comorbidities reflected the pathophysiology of the phenotype (Figure 2). Arterial hypertension was quasi-ubiquitous at 87.9% (181/206), confirming the role of pressure overload in maintaining symptoms and decompensation. Chronic coronary artery disease was frequent (62.1%, stable angina 128/206), whereas myocardial infarction was less common (18.4%, 38/206), distinguishing HFpEF from the reduced ejection fraction phenotype. The burden of atrial fibrillation remained substantial at 47.6% (98/206), with direct implications for thromboembolic protection and rate/rhythm control. A history of revascularization was present in a relevant subgroup: PCI 12.6% (26/206) and bypass 11.7% (24/206), with treated valvular disease contributing additionally (surgery 10.7%, 22/206; percutaneous intervention 1.0%, 2/206). The extent of extra-coronary atherosclerosis was moderate, with peripheral vascular disease 5.8% (12/206), stroke/TIA 8.7% (18/206), and venous thromboembolism 1.5% (3/206); these values support the need for multi-territorial secondary prevention without altering the dominant pressure–overload profile.
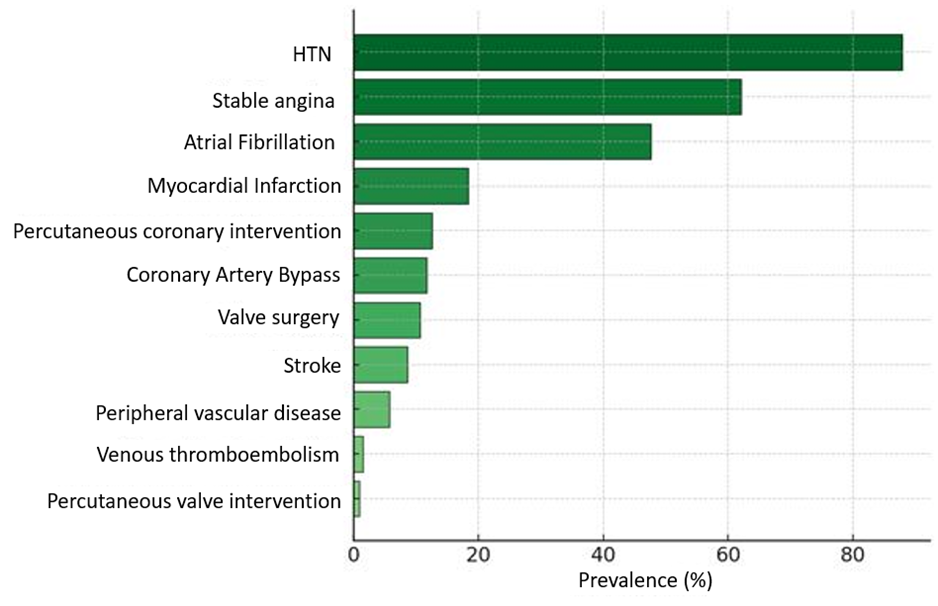 |
Fig. 2 Prevalence of cardiovascular comorbidities in patients with HFpEF Note: Bars indicate the percentage (%) of patients presenting each comorbidity or with a history of cardiovascular procedures. HTN = hypertension; HFpEF = heart failure with preserved ejection fraction; PCI = percutaneous coronary intervention. Data are presented as percentages of the study population. Descriptive statistics are shown; no inferential statistical tests were applied. |
Non-cardiovascular comorbidities completed a moderately metabolic–endocrine profile, with less systemic congestion than in HFrEF (Figure 3). Diabetes (current/history) was present in 26.2% (54/206), representing a transversal risk factor complicating vascular stiffness and diastolic function, justifying preferential use of cardiometabolic therapies with event-related benefits. COPD occurred in 9.2% (19/206), affecting dyspnea and exercise tolerance, requiring careful differentiation from congestion. Thyroid dysfunction (current/history) was reported in 9.2% (19/206), consistent with higher prevalence in patients with LVEF ≥40% and potentially affecting heart rate, arrhythmias, and symptom perception. Hepatic dysfunction was relatively rare at 3.9% (8/206), suggesting less systemic congestion than in reduced EF. Other comorbidities were infrequent: sleep apnea 2.4% (5/206), depression 1.9% (4/206), cognitive dysfunction 1.0% (2/206), active malignancy 0.5% (1/206), rheumatoid arthritis 0.5% (1/206), but remain relevant for adherence, quality of life, and care planning.
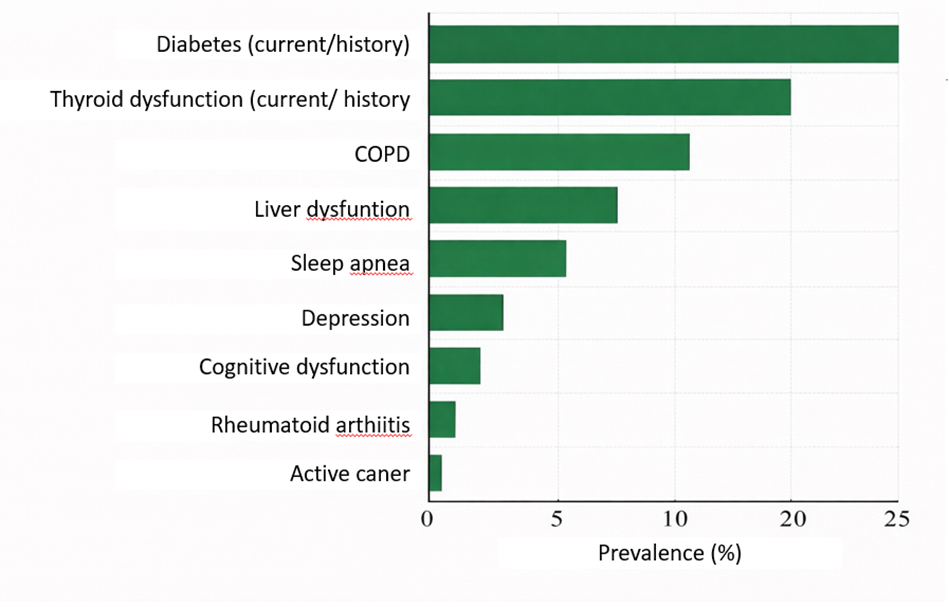 |
Fig. 3 Prevalence of non-cardiovascular comorbidities in patients with HFpEF Note: Data are presented as percentages of the total study population. Abbreviations: HFpEF = heart failure with preserved ejection fraction; COPD = chronic obstructive pulmonary disease. The figure presents descriptive statistics only; no inferential statistical tests were applied. |
Overall, our typical HFpEF patient is middle-aged to elderly, slightly more often female, with a BMI ≈30 kg/m², predominantly hypertensive, chronic coronary disease in over half, atrial fibrillation in nearly half, diabetes in about a quarter, and NT-proBNP values indicative of elevated filling pressures. This profile calls for aggressive blood pressure control, systematic AF management (anticoagulation, rate/rhythm control), ischemic secondary prevention where indicated, cardiometabolic optimization (including weight loss and cardiovascular-beneficial therapies), screening for thyroid dysfunction and sleep apnea, and consistent lifestyle and adherence interventions.
Study limitations include the relatively small sample size and observational design, which precludes establishing causality. Additionally, biological variability of NT-proBNP and the absence of advanced imaging or functional assessments (e.g., strain echocardiography, invasive filling pressure measurements) may influence the interpretation of correlations between comorbidities and cardiac function.
Discussion
This study provides a detailed phenotypic characterization of HFpEF patients, emphasizing the central role of comorbidities in shaping functional status and clinical outcomes. The predominance of older women with elevated BMI highlights the typical demographic and metabolic profile associated with HFpEF, consistent with prior reports. Our findings reinforce the concept that chronic coronary disease and hypertension are key drivers of disease pathophysiology, contributing to diastolic dysfunction, elevated filling pressures, and exercise limitation.
The observed heterogeneity in NT-proBNP levels and functional NYHA classes underscores the complexity of HFpEF, where biomarker variability and multiple comorbidities influence symptom burden and prognosis.
Cardiovascular comorbidities such as atrial fibrillation, coronary artery disease, and hypertension, alongside non-cardiovascular conditions including diabetes, COPD, and thyroid dysfunction, further modulate the clinical phenotype. These results align with recent cluster and phenotyping studies, emphasizing the importance of individualized evaluation and management.
Our study highlights practical implications for HFpEF management. Multidisciplinary approaches targeting blood pressure control, atrial fibrillation management, cardiometabolic optimization, and secondary prevention of ischemic events are critical. Screening for thyroid dysfunction, sleep apnea, and implementing lifestyle interventions can further improve functional capacity and quality of life. The identification of comorbidity clusters may guide precision therapy and optimize response to interventions, including aerobic exercise and pharmacologic strategies.
Study limitations include the relatively small sample size and the observational design, which preclude establishing causality. Furthermore, biological variability of NT-proBNP and the absence of advanced imaging or functional assessments (e.g., strain echocardiography, invasive measurements of ventricular filling pressures) may have influenced the interpretation of correlations between comorbidities and cardiac function. Selection bias is also possible, as patients were recruited from a single tertiary center.
Conclusions
This study shows that HFpEF is a complex and diverse condition influenced by many comorbidities. It highlights the need for a comprehensive, phenotype-based approach to care that combines comorbidity assessment, clinical evaluation, and biomarker analysis to personalize treatment. Identifying groups of comorbidities helps clinicians choose more targeted interventions and improve outcomes through a multidisciplinary approach, including cardiometabolic management, lifestyle changes, and screening for non-cardiac diseases. The findings support the move toward precision medicine in HFpEF, promoting individualized strategies to improve treatment response. Although causality cannot be confirmed, the study offers a useful framework for future research on phenotype-guided therapies and emphasizes the importance of personalized and integrated care to improve prognosis.
Competing interests
None declared.
Authors’ contributions
The study was conceived and designed by C-PI. Data collection and analysis were performed by C-PI, SA, and RV. Drafting of the manuscript was done by C-PI and SA. All authors critically reviewed and approved the final version of the manuscript.
Ethics approval
The study protocol was approved by the institutional ethics committee (Approval No. 25/1, May 13, 2025). The study was conducted in accordance with the principles of the Declaration of Helsinki on biomedical research involving human subjects.
Informed consent
Obtained.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Authors’ ORCID IDs
Irina Cabac-Pogorevici – https://orcid.org/0000-0001-9813-6763
Adriana Scalețchi – https://orcid.org/0009-0006-0327-3444
Valeriu Revenco – https://orcid.org/0000-0002-9419-025X
References
McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599-3726. doi: 10.1093/eurheartj/ehab368.
Li L, Li Z, Xu P, Huang L, Peng X, Yue J, Ge N. Comorbidities and incidence of heart failure with preserved ejection fraction: a systematic review and meta-analysis of cohort studies. BMJ Open. 2025;15(7):e093306. doi: 10.1136/bmjopen-2024-093306.
Ambardekar AV, Thielen SC. Comorbidities in heart failure: expect and embrace the complexity. J Am Coll Cardiol Heart Fail. 2023;11(11):1504-1506. doi: 10.1016/j.jchf.2023.06.025.
Wong B, Dodd JD, Gallagher J, Dyer B, Ryan C, McDonald K, Ledwidge M. Sex-related pathophysiological mechanisms may be present before symptoms of HFpEF develop. ESC Heart Fail. 2025;12(3):2387-2390. doi: 10.1002/ehf2.15228.
Morgen CS, Haase CL, Oral TK, Schnecke V, Varbo A, Borlaug BA. Obesity, cardiorenal comorbidities, and risk of hospitalization in patients with heart failure with preserved ejection fraction. Mayo Clin Proc. 2023 Oct;98(10):1458-1468. doi: 10.1016/j.mayocp.2023.07.008.
Szlagor M, Dybiec J, Młynarska E, Rysz J, Franczyk B. Chronic kidney disease as a comorbidity in heart failure. Int J Mol Sci. 2023;24(3):2988. doi: 10.3390/ijms24032988.
Kallistratos E, Konstantinidis D, Triantafillidi H, Grassos Ch, Maragkoudakis S, Bostanitis I, et al. Epidemiology and clinical characteristics of heart failure with preserved ejection fraction in hypertensive patients over 60 years old (HFpEF-Hypertension). J Hypertens. 2025 May;43(Suppl 1):e157. doi: 10.1097/01.hjh.0001116764.68064.09.
Hobbach AJ, Brix TJ, Weyer-Elberich V, Varghese J, Reinecke H, Linke WA. Obesity and comorbidities in HFpEF: a retrospective cohort analysis in a University Hospital Setting. J Clin Med. 2025 May 12;14(10):3348. doi: 10.3390/jcm14103348.
Savic L, Mrdovic I, Asanin M, Stankovic S, Lasica R, Matic D, Simic D, Krljanac G. Prognostic impact of non-cardiac comorbidities on long-term prognosis in patients with reduced and preserved ejection fraction following acute myocardial infarction. J Pers Med. 2023;13(7):1110. doi: 10.3390/jpm13071110.
Martens P, Augusto SN Jr, Finet JE, Tang WHW. Distinct impact of noncardiac comorbidities on exercise capacity and functional status in chronic heart failure. JACC Heart Fail. 2023;11(10):1365-1376. doi: 10.1016/j.jchf.2023.05.018.
Ono R, Falcão LM. Primary heart failure with preserved ejection fraction: the intertwined pathophysiology and treatment of some of the most relevant phenotypes. Rev Port Cardiol. 2025 Jul;44(7):445-456. doi: 10.1016/j.repc.2025.02.007.
Savarese G, Settergren C, Schrage B, Thorvaldsen T, Löfman I, Sartipy U, et al. Comorbidities, quality of life and cause-specific outcomes in heart failure across the ejection fraction spectrum: a blueprint for clinical trial design. Int J Cardiol. 2020;313:76-82. doi: 10.1016/j.ijcard.2020.04.068.
Menghoum N, Badii MC, Leroy M, Parra M, Roy C, Lejeune S, et al. Exploring the impact of metabolic comorbidities on epicardial adipose tissue in heart failure with preserved ejection fraction. Cardiovasc Diabetol. 2025;24(1):134. doi: 10.1186/s12933-025-02688-7.
Zatsarinnyy A, Miyerbekov Y, Uvaliyeva S, Sugurbayev M, Musrepov N, Rakisheva A. Pathophysiology and phenotypes of heart failure: current concepts and future directions. Heart Fail J India. 2025;3(2):124. doi: 10.4103/HFJI.HFJI_19_25.
Lanzer JD, Valdeolivas A, Pepin M, Hund H, Backs J, Frey N, et al. A network medicine approach to study comorbidities in heart failure with preserved ejection fraction. BMC Med. 2023 Jul 24;21(1):267. doi: 10.1186/s12916-023-02922-7.
Cabac-Pogorevici I, Revenco V. Heart failure and central sleep apnea in the era of implantable recorders. Anatol J Cardiol. 2021;25(4):216-224. doi: 10.5152/AnatolJCardiol.2021.63668.
Jitari I, Savca D, Ochișor V, Revenco V, Cabac-Pogorevici I. Abordarea individualizată în insuficiența cardiacă cu fracția de ejecție păstrată – de la practica clinică la inteligență artificială [The individualized approach in heart failure with preserved ejection fraction. From clinical practice to Artificial Intelligence]. Bull Acad Sci Mold. Med Sci (Chisinau). 2024;78(1):205-211. Romanian. doi: 10.52692/1857-0011.2024.1-78.22.