
Introduction
Pulmonary thromboembolism (PTE) is a major cardiovascular condition associated with high mortality, particularly in patients with hemodynamic instability [1]. Systemic inflammation plays a key role in the pathogenesis of thrombosis and disease progression, and inflammatory hematological indices derived from the complete blood count, such as the neutrophil-to-lymphocyte ratio (NLR) and the platelet-to-lymphocyte ratio (PLR), have been identified as predictors of disease severity and mortality [2], although evidence for PLR remains limited, with some studies failing to demonstrate an independent prognostic role [3]. The purpose of the study was to evaluate the correlation of NLR and PLR with CT pulmonary angiography findings, echocardiographic parameters, Pulmonary Embolism Severity Index (PESI) severity score, and mortality in patients with pulmonary thromboembolism.
Material and methods
This prospective observational study was conducted on a cohort of 182 consecutive patients admitted with clinical suspicion of PTE to two hospital institutions between 2021 and 2025: Holy Trinity Municipal Clinical Hospital and the Institute of Cardiology.
Participant Selection. The study included adult patients (≥18 years) with clinical suspicion of acute PTE. The diagnosis was confirmed by CT pulmonary angiography (CTPA), which is considered the standard of care for this condition and allows exclusion of relevant differential diagnoses [1, 4].
For each patient, demographic data (age, sex), clinical presentation at admission, comorbidities, laboratory parameters, and imaging findings were collected. Laboratory analyses included a complete blood count, from which the NLR and PLR were calculated, as well as D-dimer and NT-proBNP levels,Wells score, revised Geneva score. All patients underwent echocardiographic evaluation, including assessment of right ventricular function parameters such as right ventricular diameter and tricuspid annular plane systolic excursion (TAPSE), and TAPSE/PSAP index. Disease severity was assessed using the Pulmonary Embolism Severity Index (PESI) score. Patients were followed up for clinical outcomes and mortality during the course of inpatient care. Exclusion criteria were: patients with symptoms attributable to other acute conditions, such as acute or chronic coronary syndrome, dissecting aortic aneurysm, acute abdomen, or acute heart or respiratory failure, as well as patients who used drugs that may affect laboratory parameters (steroids, antibiotics, cytotoxic agents, immunosuppressants, antiplatelet drugs, anticoagulants, epinephrine).
Statistical analysis. Categorical variables were summarized as frequencies and percentages. The predictive value of NLR and PLR for mortality was assessed using Receiver Operating Characteristic (ROC) curve analysis, calculating the area under the curve (AUC), sensitivity, and specificity. A p-value <0.05 was considered statistically significant.
Results
The prospective study included a total of 182 patients with clinical suspicion of PTE, of whom 99 were men (54.4%; 95% CI [47.2, 61.6]) and 83 were women (45.6%; 95% CI [38.4, 52.8]). Age distribution showed a predominance of elderly patients, with the most frequent age group being 60–69 years, comprising 64 cases (35.2%; 95% CI [28.2, 42.1]), followed by the 70–79 years group with 48 patients (26.4%; 95% CI [20.0, 32.8]), 50–59 years with 27 patients (14.8%; 95% CI [9.7, 20.0]), patients over 80 years with 16 cases (8.8%; 95% CI [4.7, 12.9]), 40–49 years with 18 cases (9.9%; 95% CI [5.6, 14.2]), and patients under 40 years, who accounted for 9 cases (4.9%; 95% CI [1.8, 8.1]).
Clinically, dyspnea was the main symptom present in 181 patients (99.5%; 95% CI [98.4, 100]). Other manifestations included cough in 68 patients (37.4%; 95% CI [30.3, 44.4]), fever in 37 patients (20.3%; 95% CI [14.5, 26.2]), syncope or presyncope in 10 patients (5.5%; 95% CI [2.2, 8.8]) and hemoptysis in 4 patients (2.2%; 95% CI [0.1, 4.3]).
Concomitant pathologies were common, the most frequent being angina pectoris in 149 patients (81.9%; 95% CI [76.3, 87.5]), arterial hypertension in 141 patients (77.5%; 95% CI [71.4, 83.5]), pneumonia in 65 patients (35.7%; 95% CI [28.8, 42.7]), arrhythmias in 60 patients (33.0%; 95% CI [26.1, 39.8]), diabetes mellitus in 34 patients (18.7%; 95% CI [13.0, 24.3]), and chronic obstructive pulmonary disease in 32 patients (17.6%; 95% CI [12.1, 23.1]).
Laboratory parameters revealed elevated D-dimer levels in 181 patients (99.5%), increased NT-proBNP in 33.0% of cases (95% CI [26.1, 39.8]), and elevated C-reactive protein in 149 patients (81.9%; 95% CI [76.3, 87.5]). The neutrophil-to-lymphocyte ratio (NLR) was elevated in 82 patients (45.1%; 95% CI [37.8, 52.3]), and the platelet-to-lymphocyte ratio (PLR) was elevated in 89 patients (48.9%; 95% CI [41.6, 56.2]). The overall mortality was 17.0% (95% CI [11.6, 22.5]), corresponding to 31 patients. Among these, 26 patients (14.3%; 95% CI [9.2, 19.4]) had elevated NLR, and 22 patients (12.1%; 95% CI [7.4, 16.8]) had elevated PLR, demonstrating a significant association between inflammatory hematological indices and mortality.
According to the Wells score, intermediate clinical probability was present in 129 patients (70.9%; 95% CI [64.3, 77.5]), and high probability in 52 patients (28.6%; 95% CI [22.0, 35.1]). The revised Geneva score indicated intermediate probability in 118 patients (64.8%; 95% CI [57.9, 71.8]) and high probability in 52 patients (28.6%; 95% CI [22.0, 35.1]).
Echocardiographic evaluation revealed significant right ventricular alterations. Right ventricular dysfunction was present in 146 patients (80.2%; 95% CI [74.4, 86.0]), and TAPSE was reduced in 105 patients (57.7%; 95% CI [50.5, 64.9]). Assessment of right ventriculo-arterial coupling, expressed as the TAPSE/PASP ratio, showed normal values in 41 patients (22.5%; 95% CI [16.5, 28.6]), mildly reduced values in 44 patients (24.2%; 95% CI [18.0, 30.4]), and reduced values in 97 patients (53.3%; 95% CI [46.0, 60.5]), indicating severe right ventricular dysfunction in more than half of the patients.
The diagnosis of PTE was confirmed by CTPA in 153 patients (84.1%; 95% CI [78.7, 89.4]) while in 29 patients (15.9%; 95% CI [10.6, 21.3]) the diagnosis was not confirmed.
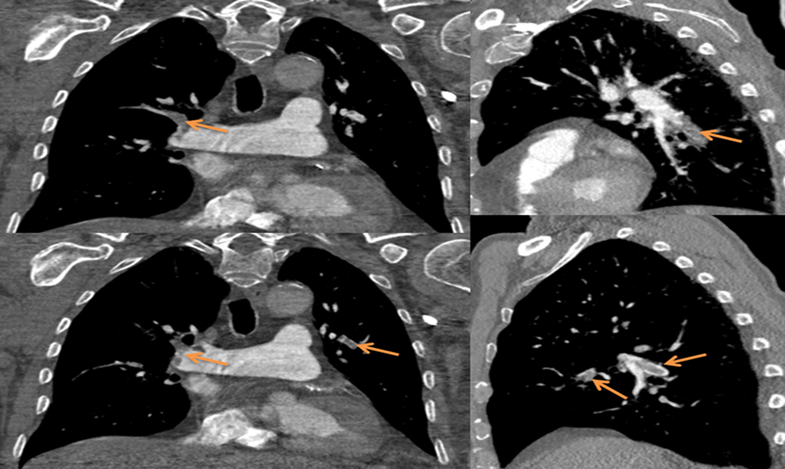 |
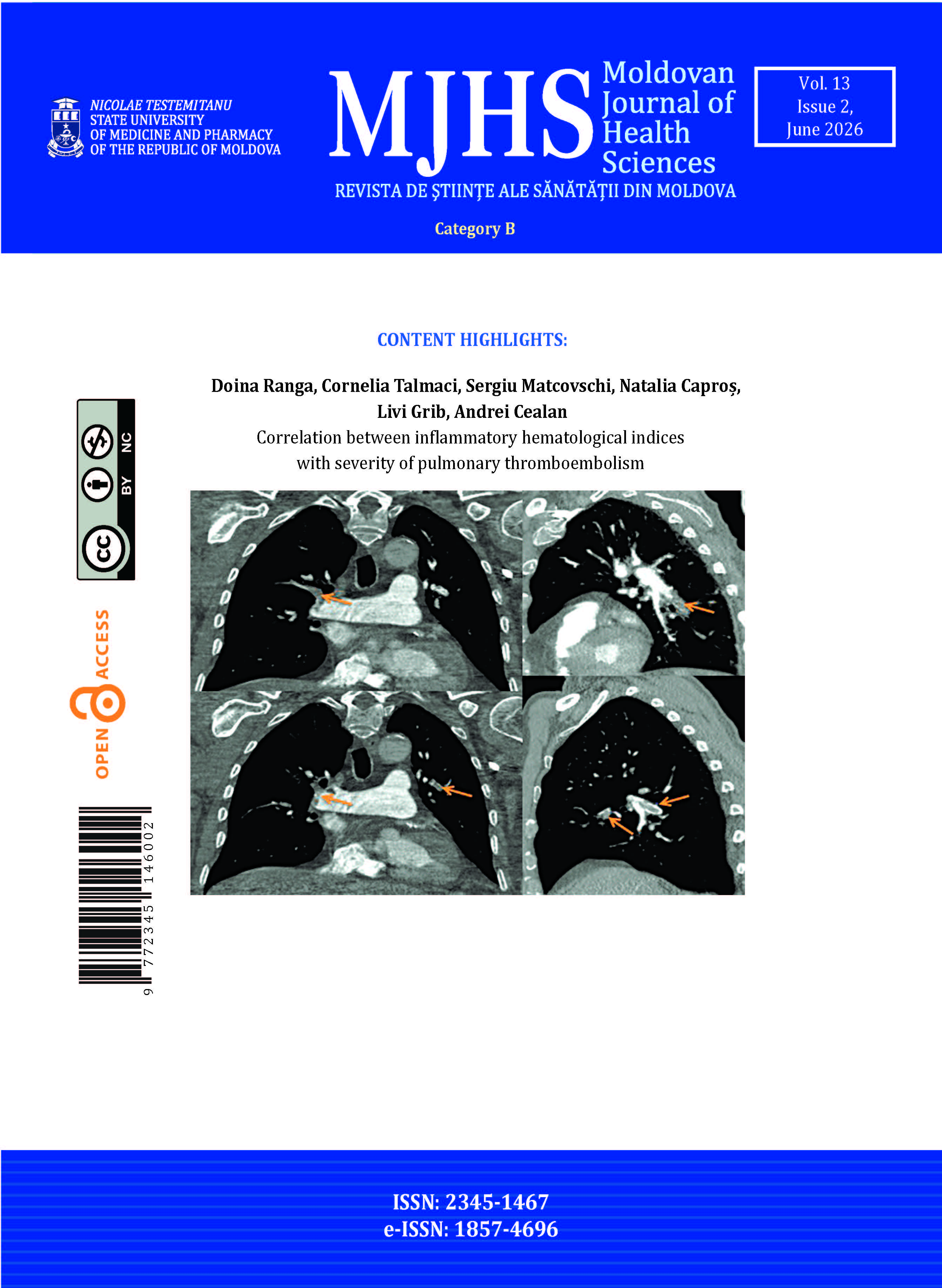
Fig. 1 Chest and mediastinal CT pulmonary angiography. Note: After intravenous contrast administration, filling defects are observed in the right middle and lower lobe pulmonary arteries, associated with areas of pulmonary consolidation containing air bronchograms, suggestive of pulmonary infarction with abscess formation on the right. A right-sided pleural effusion with air-fluid levels is also present, consistent with pleural empyema. Pulmonary hypertension is indicated by a pulmonary trunk diameter of 3.2 cm. |
Among patients with confirmed PTE (Figure 1), bilateral filling defects were identified in 123 patients (67.6%; 95% CI [60.8, 74.4]), central-peripheral location in 114 patients (62.6%; 95% CI [55.6, 69.7]), peripheral location in 38 patients (20.9%; 95% CI [15.0, 26.8]), involvement of the right pulmonary artery in 22 patients (12.1%; 95% CI [7.4, 16.8]), and the left pulmonary artery in 8 patients (4.4%; 95% CI [1.4, 7.4]). Signs of right ventricular dilatation on CTPA were present in 77 patients (42.3%; 95% CI [35.1, 49.5]).
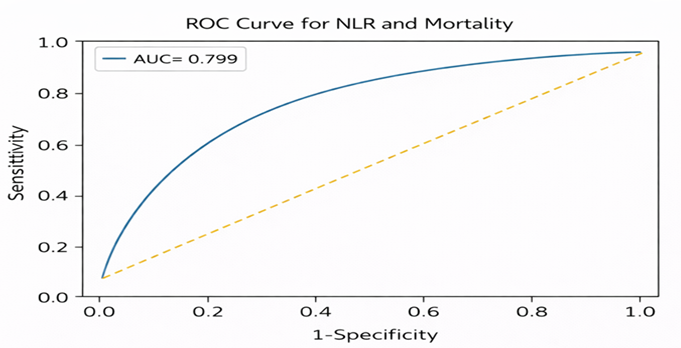 |
Fig. 2. ROC curve for NLR predicting mortality. Note: Receiver operating characteristic (ROC) curve demonstrating the predictive performance of the neutrophil-to-lymphocyte ratio (NLR) for mortality in patients with pulmonary embolism. The area under the curve (AUC) was 0.799. The dashed line represents the line of no discrimination. |
ROC curve analysis demonstrated that the neutrophil-to-lymphocyte ratio (NLR) had the highest predictive value for mortality, with an AUC of 0.799, indicating very good prognostic performance (Figure 2).
 |
Fig. 3 ROC curve for PLR predicting mortality. Note: Receiver operating characteristic (ROC) curve demonstrating the predictive performance of the platelet-to-lymphocyte ratio (PLR) for mortality in patients with pulmonary embolism. The area under the curve (AUC) was 0.715. The dashed line represents the reference line. |
The platelet-to-lymphocyte ratio (PLR) showed good predictive value, with an AUC of 0.715 (Figure 3), and NLR correlated with disease severity assessed by the PESI score, with an AUC of 0.614 (Figure 4).
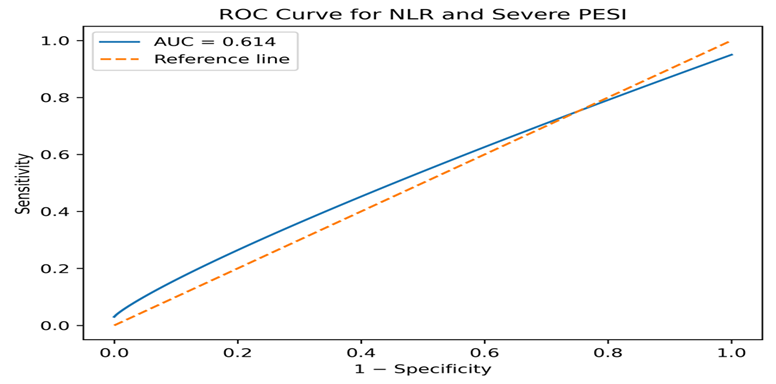 |
Fig. 4 ROC curve for NLR predicting severe PESI. Note: Receiver operating characteristic (ROC) curve showing the predictive value of the neutrophil-to-lymphocyte ratio (NLR) for severe pulmonary embolism assessed by the Pulmonary Embolism Severity Index (PESI). The area under the curve (AUC) was 0.614. The dashed line represents the reference line (line of no discrimination). |
Assessment of disease severity using the PESI score showed a predominance of patients with intermediate and high risk, comprising 104 patients (57.1%; 95% CI [50.0, 64.3]).
Discussion
In our study, the diagnosis of pulmonary thromboembolism was confirmed by CT pulmonary angiography, which remains the gold standard for identifying arterial filling defects and assessing disease severity, with high sensitivity and specificity, as previously reported, including in studies conducted at our institution [1].
The results of our study demonstrated that the NLR is an important predictor of mortality in patients with pulmonary thromboembolism, with an AUC of 0.799. These findings are consistent with those reported by Tang et al., who found similar predictive value for NLR, confirming the role of systemic inflammation in disease progression [3]. Elevated NLR reflects activation of the inflammatory response and has been associated with right ventricular dysfunction and poor prognosis, data consistent with the findings of Kowsika R. et al [2].
Elevated NLR in acute PE was associated with a worse short-term and long-term prognosis and with a longer duration of hospitalization in a study by Efros O. et al [5]. In a meta-analysis by Wang Q, was revealed that NLR and PLR are promising biomarkers in predicting prognosis in acute PE patients and recommended NLR and PLR be used routinely in the PE prognostic assessment [6].
Severity assessed by the PESI score correlated with elevated NLR values, confirming the results reported by Teodoru M. et al., who showed that inflammatory hematological indices can improve risk stratification in patients with pulmonary thromboembolism [7].
Conclusions
The neutrophil-to-lymphocyte ratio is an important prognostic marker of severity and mortality in pulmonary thromboembolism, with a predictive value superior to that of the platelet-to-lymphocyte ratio. Integrating inflammatory hematological indices with clinical scores and imaging assessment may improve risk stratification and the management of patients with pulmonary thromboembolism.
Competing interests
None declared.
Authors’ contributions
DR conceived the study design and performed the statistical analysis. CT participated in diagnosing and treating patients with pulmonary thromboembolism. SM critically reviewed the manuscript and contributed to its intellectual content. NC participated in the study design and critically reviewed the manuscript. LG provided clinical expertise and consultation for the management of most patients. CA radiologist, performed CT, pulmonary angiography in the majority of patients. All authors have read and approved the final version of the manuscript.
Ethics approval
The study protocol was reviewed and approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy, Chișinău, Republic of Moldova (Approval No. 2/25; March 30, 2023). All procedures were conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments.
Patient consent
Obtained.
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer reviewed.
Authors’ ORCID IDs
Doina Ranga – https://orcid.org/0009-0007-1345-4975
Cornelia Talmaci – https://orcid.org/0000-0002-5603-2277
Sergiu Matcovschi – https://orcid.org/0000-0003-1623-930X
Natalia Caproș – https://orcid.org/0000-0001-7283-8468
Livi Grib – https://orcid.org/0000-0001-6913-0864
Andrei Cealan – https://orcid.org/0000-0001-8478-097X
References
- Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41(4):543-603. doi: 10.1093/eurheartj/ehz405.
- Kowsika R, Muthukumaran L, Sridhar R et al. Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio as biomarkers for risk stratification and predictors of 90-day mortality in acute pulmonary embolism. South East Eur J Pub Health. 2025;26(Suppl 1):6009-6018.
- Tang S, Hu Y. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as predictors of mortality in acute pulmonary embolism: a systematic review and meta-analysis. Pak J Med Sci. 2024 Jul;40(6):1274-1279. doi: 10.12669/pjms.40.6.8802.
- Ranga D, Caproș N, Cealan A, Sirbu I, Talmaci C, Matcovschi S. Diagnosing pulmonary embolism with computed tomography pulmonary angiography. In: Sontea V, Tiginyanu I, Railean S, editors. IFMBE-2023: 6th International Conference on Nanotechnologies and Biomedical Engineering, 20-23 September 2023, Chişinău, Republic Moldova: Abstract book. Chişinău: Springer; 2024. Vol.92, p. 333-342. ISBN 978-303142781-7. https://doi.org/10.1007/978-3-031-42782-4_36.
- Efros O, Beit Halevi T, Meisel E, et al. The prognostic role of neutrophil-to-lymphocyte ratio in patients hospitalized with acute pulmonary embolism. J Clin Med. 2021 Sep 8;10(18):4058. doi: 10.3390/jcm10184058.
- Wang Q, Ma J, Jiang Z, Ming L. Et al. Prognostic value of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in acute pulmonary embolism: a systematic review and meta-analysis.Int Angiol. 2018 Feb;37(1):4-11. doi: 10.23736/S0392-9590.17.03848-2.
- Teodoru M, Negrea MO, Cozgarea A, et al. Enhancing pulmonary embolism mortality risk stratification using machine learning: the role of the neutrophil-to-lymphocyte ratio. J Clin Med. 2024 Feb 20;13(5):1191. doi: 10.3390/jcm13051191.