
Introduction
Boron is a trace element that has not yet been recognized as essential for the human body. The World Health Organization (WHO) highlights that insufficient boron intake can impair the body's biological functions, potentially causing long-term harm [1]. The WHO recommends drinking water as the primary source of this element and prioritizing natural springs rich in boron [2].
A minimum intake of 0.4 mg of boron per day can contribute to the strengthening of bone mass, with the regulated boron concentration in drinking water providing the body with basic essential benefits [2, 3]. Moreover, an adequate boron intake can reduce calcium and magnesium loss through urine [4, 5], promote osteogenesis [3, 6], decrease inflammatory joint processes [7, 8], reduce articular discomfort, and improve mobility [4, 9]. Osteoarticular diseases that can be prevented by a boron-rich diet include osteoarthritis, rheumatoid arthritis, and osteoporosis [10-12]. Recent research shows positive effects of boron on bone mass when the daily intake is 3 mg or more [5, 13, 14].
Population studies conducted more than three decades ago revealed that the incidence of arthritis was negatively associated with boron concentrations in soil and foods. Thus, in areas where the population’s daily boron intake was below 1 mg/day, the arthritis incidence ranged from 20 to 70%, while in regions where it was 3-10 mg/day, the incidence of this pathology was between 0 and 10% [4]. Since those findings, no other population study of comparable scale has been conducted.
Following the previous national report, in the southern region of the Republic of Moldova, in Administrative Territorial Unit Gagauzia, drinking water is richest in boron, with concentrations reaching up to 3 mg/l. These results have not yet been linked with the population's health status [15]. Considering the lack of research on boron's impact on public health in our country, and the fact that osteoarticular diseases are the most studied in relation to daily boron intake, this association was chosen for our study.
Even though European regulations have set a limit of 1,5 mg/L of boron in drinking water and mention that this parameter can be raised to 2.4 mg/L in boron-rich areas [16], in our country, the maximum allowable boron concentration in drinking water is 1 mg/L [17]. Another justification for this research is to provide arguments for aligning national regulations on boron concentrations in drinking water with European standards.
This study aims to assess the morbidity caused by rheumatoid arthritis and inflammatory polyarthropathies in the population from regions with different boron concentrations in deep drinking water (public wells and artesian wells) of the Republic of Moldova.
Material and methods
To achieve the intended purpose, two full-length descriptive observational studies were conducted: one on osteoarticular morbidity and one on boron concentrations in deep drinking water.
The first step involved conducting a full-length descriptive observational study on osteoarticular morbidity (incidence and prevalence) caused by rheumatoid arthritis and inflammatory polyarthropathies during the period 2016-2020 (Table 1).
The results were analyzed and presented for the group of rheumatoid arthritis and inflammatory polyarthropathies as a whole. According to the International Statistical Classification of Diseases and Related Health Problems, Eleventh Revision (ICD-11), the group includes nine diseases, their codes being included between FA20 and FA27 and FA2Z.
Table 1. A brief description of the first full-length descriptive observational study on osteoarticular morbidity | |
Criteria | Description |
Object of study | Adult morbidity due to rheumatoid arthritis and inflammatory polyarthropathies |
Source of information | Data from the Health Data Management Department of the National Agency for Public Health |
Collection method | Data processing, calculation of multiannual averages |
Volume | A comprehensive study covering the period 2016-2020 |
Place of performance | National Agency for Public Health |
During the second step, a full-length descriptive observational study on boron concentrations in deep drinking water–from public wells and artesian wells–covering the 2015-2022 period was conducted (Table 2).
The main argument of including water from public wells into our study was that this water source is frequently used by the rural population, which according to the National Bureau of Statistics in 2017 constitutes 57.1% of the country's population and is a representative part of this research.
Table 2. A brief description of the second full-length descriptive observational study on boron concentrations in deep drinking water | |
Criteria | Description |
Object of study | Boron concentrations in water from public wells and artesian wells across the territory of the Republic of Moldova |
Source of information | Data from territorial Public Health Centers (2015-2020) |
Collection method | Data processing, calculation of annual and multiannual averages |
Volume | A comprehensive study for the period 2015-2020, with 2,706 samples investigated |
Place of performance | National Agency for Public Health |
Of the 2706 samples investigated, 480 were public well water and 2226 were artesian well water. The results were taken from the registers of territorial public health centers for the period 2015-2020. All available results from both sources were analyzed. Most samples were collected during the late summer-autumn period (August-November) or during spring (March-April). For artesian well water, for each locality, at least one sample from each artesian well has been collected per year, and the majority of them were analyzed for boron concentrations. For public well water, samples were collected less often, with an average periodicity of 1-3 samples analyzed for boron concentrations in 6 years, and not for all researched localities.
Given the national regulations restrict the boron concentrations in deep drinking water to 1 mg/L, the territory of the Republic of Moldova was divided into three distinct areas:
Below the limit – boron concentrations between 0 and 0.8 mg/L;
Limit –boron concentrations between 0.9 and 1.2 mg/L;
Above the limit – boron concentrations above 1.2 mg/L.
From the available data, the most representative districts for each area were selected - for below the limit districts – districts with average values close to the lower limit, for districts in the limit area - average values close to the limit of 1 mg boron/l and for above the limit districts - maximum average values recorded in the country. Both public wells and artesian wells values were taken into consideration, but one of the two values for each district was the basis for the selection.
Following these criteria, selected districts for each boron-related area are:
Below the limit area:
Călărași: 0.2 mg B/L in public wells;
Briceni: 0.25 mg B/L in artesian wells;
Drochia: 0.3 mg B/L in public wells.
Limit area:
Cahul: 0.9 mg B/L in artesian wells;
Vulcănești: 1.1 mg B/L in artesian wells.
Above the limit area:
Ceadîr-Lunga: 1.8 mg B/L in public wells;
Comrat: 1.43 mg B/L in artesian wells.
In the final stage, boron concentrations in deep drinking water and adult morbidity due to rheumatoid arthritis and inflammatory polyarthropathies were graphically overlaid for each selected district, and trendlines for both boron concentrations and osteoarticular morbidity were calculated using Microsoft Excel 2021.
Statistical data processing: For the prevalence data of adults with rheumatoid arthritis and inflammatory polyarthropathies, the average prevalence for the research period was calculated. Boron concentration data in deep drinking water were organized into two separate databases: one for public wells and another for artesian wells. Average boron concentrations were calculated separately for each village and district, including the Administrative Territorial Unit Gagauzia, on a yearly basis. Subsequently the total average concentration for the analyzed period was determined for each district. Microsoft Excel 2021 was used for database creation and calculations of all averages.
The study protocol was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes No 1 of 07.09.2020).
Results
The below-the-limit boron in deep drinking water refers to multiannual averages of boron concentration between 0 and 0.8 mg/L.
In the Călărași district, in 2020, when the boron concentrations in public wells and artesian wells reached their highest levels during the research period, the prevalence of rheumatoid arthritis and inflammatory polyarthropathies recorded its lowest values. The upward trend in boron concentrations in deep drinking water (y = 0.06x + 0.3825 for artesian wells water and y = 0.0442x + 0,0654 for public wells water) overlapped with a downward trend in the prevalence of rheumatoid arthritis and inflammatory polyarthropathies among adults during the 2016-2020 period (y = -1,48x + 35.78) which supports the research hypothesis (Figure 1).
 |
Fig. 1 Boron concentrations in deep drinking water (mg/L) and adult morbidity from rheumatoid arthritis and inflammatory polyarthropathies (per 10,000 inhabitants), Călărași district, 2016-2020 |
In Briceni, in 2018, both the prevalence and incidence of adults with rheumatoid arthritis and inflammatory polyarthropathies increased against the background of a decrease in boron concentrations in water from public and artesian wells. The trends for boron concentrations in artesian wells (y = -3.25x + 28.65), as well as for the incidence (y = -0.18x +3.85) and prevalence (y = -0.055x +0.375) of rheumatoid arthritis and inflammatory polyarthropathies in adults, were all decreasing (Figure 2). Although the trendlines for boron concentrations in deep drinking water and adult morbidity do not support the research hypothesis, the increase in prevalence and incidence coincides with the decrease in boron concentrations in artesian wells.
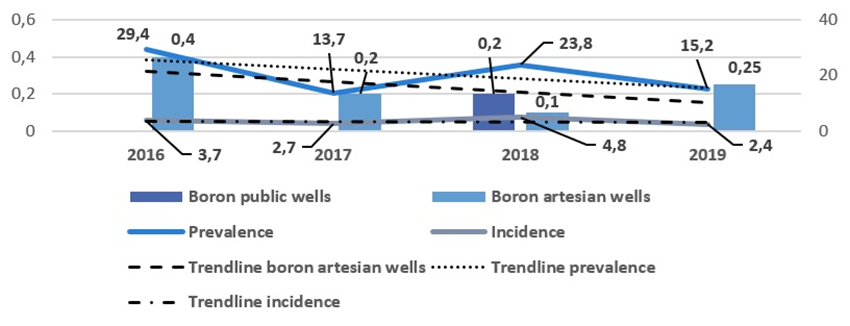 |
Fig. 2 Boron concentrations in deep drinking water (mg/L) and adult morbidity from rheumatoid arthritis and inflammatory polyarthropathies (per 10,000 inhabitants), Briceni district, 2016-2019 |
In the Drochia district, in 2020, boron concentrations in deep drinking water, as well as osteoarticular morbidity, reached their maximum values for the analyzed period. Additionally, the trends for boron concentrations in artesian well water (y = 0.0071x + 0.5143) and prevalence from rheumatoid arthritis and inflammatory polyarthropathies (y = 3.14x + 13.38) were both positive (Figure 3). Neither the trendlines for boron concentrations in deep drinking water and osteoarticular morbidity nor of the year-by-year overlap between boron concentrations and incidence/prevalence support the research hypothesis.
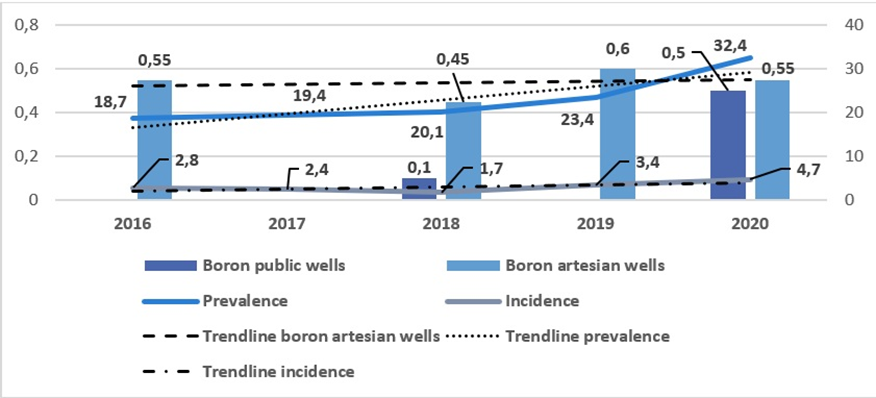 |
Fig. 3 Boron concentrations in deep drinking water (mg/L) and adult morbidity from rheumatoid arthritis and inflammatory polyarthropathies (per 10,000 inhabitants), Drochia district, 2016-2020 |
Limit-boron in the deep drinking water area (multiannual averages of boron in deep drinking water between 0.9 and 1.2 mg/L)
In the Cahul district, in 2016, when the boron concentration in water from public wells and artesian wells reached its highest levels, the prevalence of adults with rheumatoid arthritis and inflammatory polyarthropathies also reached a maximum, while the incidence was at its lowest for the 2016-2020 period. Trendlines for boron concentrations in deep drinking water (y = -3E-16x + 0.86 for boron concentrations in artesian wells) and osteoarticular morbidity (-0.14x + 11.76 for the prevalence and y = -0.12x +3.3 for the incidence) were both negative (Figure 4). The overlap of high boron concentrations in public and artesian wells with the incidence values matches the research hypothesis, while the trendlines for boron and morbidity do not.
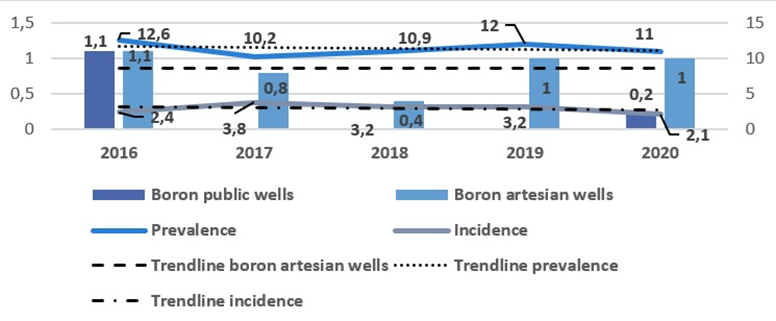 |
Fig. 4 Boron concentrations in deep drinking water (mg/L) and adult morbidity from rheumatoid arthritis and inflammatory polyarthropathies (per 10,000 inhabitants), Cahul district, 2016-2020 |
In the second district with limited boron concentration in deep drinking water, Vulcănești, during the years with the highest boron concentrations in public well water (2017-2018), both the prevalence and the incidence of adults with osteoarticular pathologies were at their highest. Additionally, the trends for boron concentrations in artesian wells (y = -0.18x +1.55) and morbidity values (y=-1.63x +18.6 for the prevalence and y = -0.45x +2 for the incidence) were negative (Figure 5). The overlapping of boron concentrations in artesian wells and annual osteoarticular morbidity, as indicated by the trendlines equations, is opposite to the research hypothesis.
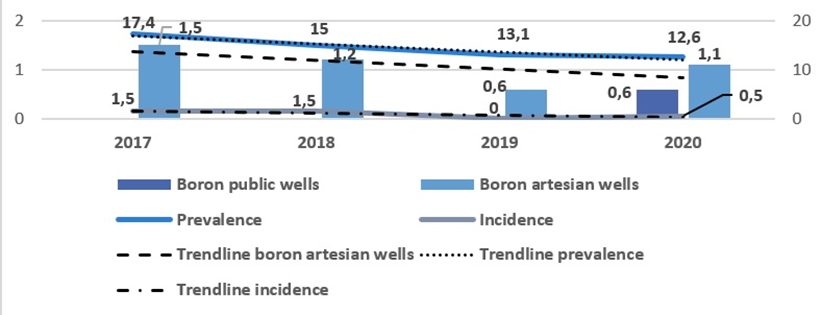 |
Fig. 5 Boron concentrations in deep drinking water (mg/L) and adult morbidity from rheumatoid arthritis and inflammatory polyarthropathies (per 10,000 inhabitants), Vulcănești district, 2017-2020 |
Above-the-limit boron in deep drinking water area (multiannual averages of boron in deep drinking water above 1.2 mg/L)
Boron concentrations in deep drinking water and morbidity indicators in the Ceadîr-Lunga district show that prevalence values for rheumatoid arthritis and inflammatory polyarthropathies increased during the period when boron concentration in deep waters was decreasing (2018-2019). Trends in boron concentrations were negative (y = -0.19x + 2.36 for public wells water and y = -0.31x + 2.61 for artesian wells water), while prevalence of rheumatoid arthritis and inflammatory polyarthropathies showed positive trends (y = 0.02x +35.96) (Figure 6).
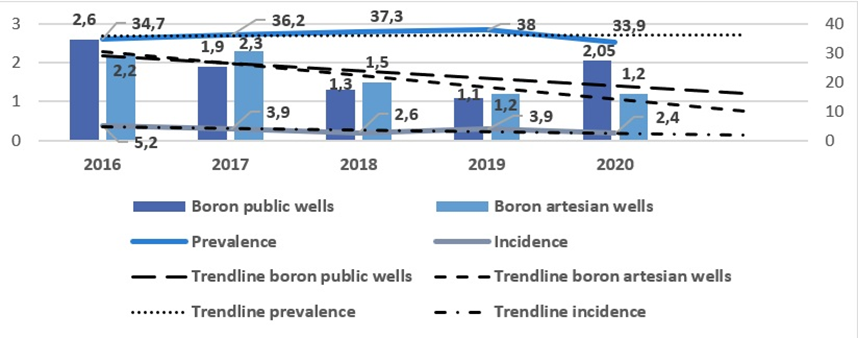 |
Fig. 6 Boron concentrations in deep drinking water (mg/L) and adult morbidity from rheumatoid arthritis and inflammatory polyarthropathies (per 10,000 inhabitants), Ceadîr-Lunga district, 2016-2020 |
In the second selected above-the-limit district, Comrat, increasing boron concentrations in artesian wells water trendline (y = 0.025x + 1.375) coincided with decreasing trends in osteoarticular morbidity (y=-3.76x + 48.7 for the prevalence and y = -1.05x + 6.7 for the incidence) (Figure 7). Although osteoarticular morbidity remains high during periods of elevated boron concentrations in artesian wells, the opposing trendlines for incidence and prevalence compared to boron concentrations support the research hypothesis.
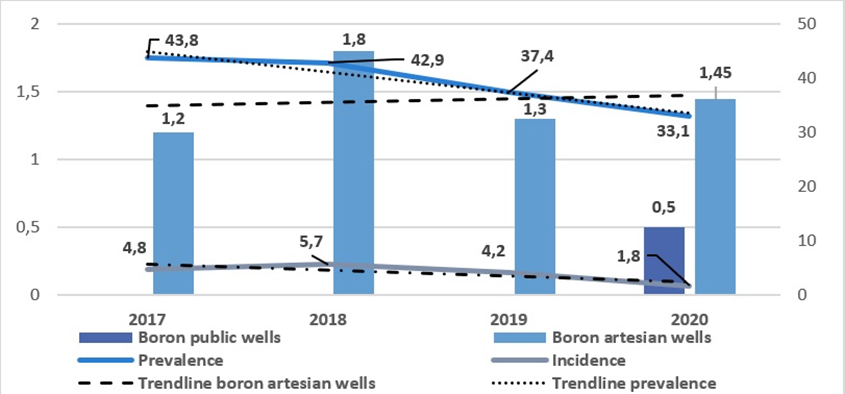 |
Fig. 7 Boron concentrations in deep drinking water (mg/L) and adult morbidity from rheumatoid arthritis and inflammatory polyarthropathies (per 10,000 inhabitants), Comrat district, 2017-2020 |
Discussion
During this research, we compared the annual averages of boron concentrations in deep drinking water (from public and artesian wells) with annual averages of incidence and prevalence of rheumatoid arthritis and inflammatory polyarthropathies in selected districts from each boron-related area, using periods when all relevant data were available. Additionally, we calculated trends for all four indicators – boron concentrations in public well water and artesian wells water, and incidence and prevalence of rheumatoid arthritis and inflammatory polyarthropathies. The aim of this study was to assess whether boron concentrations in deep drinking water can influence osteoarticular morbidity in specific regions, based on existing literature [2-14].
In the below-the-limit boron area of deep drinking water, the Călărași district showed fluctuations in boron concentrations from public and artesian wells that corresponded with the prevalence of adults with rheumatoid arthritis and inflammatory polyarthropathies, consistent with the research hypothesis. This is further supported by the increasing boron and decreasing morbidity trends. Similarly, in the Briceni district, the hypothesis is confirmed by the overlap of boron concentrations in deep drinking water and the osteoarticular morbidity indicators in adults, along with matching trends across the four indicators. However, in the Drochia district, the research hypothesis was not confirmed.
In the limit-boron area of deep drinking water, the research hypothesis was only partially confirmed in the Cahul district, and only by the incidence of the studied diseases in a single year of the study period; however, the overall trendlines did not align with the hypothesis. In Vulcănești, neither the boron concentrations in deep drinking water nor the morbidity of adults with the studied osteoarticular pathologies corresponded with the research hypothesis, and the trendlines for the three indicators also failed to match it.
In the above-the-limit boron area of deep drinking water, the research hypothesis was largely confirmed in the Ceadîr-Lunga and Comrat districts, where the boron concentrations and their trendlines overlapped with the annual averages and trendlines of morbidity, demonstrating the expected relationship.
The described results complement previously published findings, which showed that in the above-the-limit boron area of deep drinking water in the southern region of the Republic of Moldova, the multiannual averages of rheumatoid arthritis and inflammatory polyarthropathies prevalence were the highest in the country [18]. However, analyzing annual averages instead of multiannual ones, and calculating trends for both boron concentrations and osteoarticular morbidity, revealed mixed results and provided a different perspective on the boron-rich areas.
The limitations of this research include incomplete data on boron concentrations in deep drinking water, particularly for public wells, which were not available for every year. Additionally, morbidity data were only available up to 2020, resulting in differences in the analyzed periods between districts. Furthermore, it was not possible to separate rheumatoid arthritis from other inflammatory polyarthropathies, as the Health Data Management Department provided combined data. Consequently, some results may be influenced by the inclusion of various inflammatory pathologies in the statistics. For the same reason, studying the association with osteoarthritis was not feasible, as it was grouped with other chondropathies.
Taking these aspects into consideration, we believe that future investigations focusing specifically on the association between boron concentrations in deep drinking water and the separate conditions of rheumatoid arthritis and osteoarthritis could be a valuable direction.
Conclusions
The overlap of trends in boron concentrations in deep drinking water and trends in adult morbidity from rheumatoid arthritis and inflammatory polyarthropathies confirmed the research hypothesis in the above-the-limit boron area (Ceadîr-Lunga and Comrat districts) and partially in the below-the-limit boron area (Călărași and Briceni districts). These results provide a foundation for future research on the impact of boron on public health.
Competing interests
None declared.
Authors’ contributions
MVR conceived the study and drafted the manuscript, IP participated in the study design and data analysis, EC helped draft the manuscript and contributed to the study design, and LMN performed statistical analysis of clinical data. All authors have read and approved the final version of the manuscript.
Ethics approval
The study was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes No 1 of 07.09.2020).
Patient consent
Obtained.
Acknowledgements and funding
No external funding
Provenance and peer review
Not commissioned, externally peer reviewed.
Authors’ ORCID IDs
Maria-Victoria Racu – https://orcid.org/0000-0002-9203-7892
Iurie Pînzaru – https://orcid.org/0000-0001-5293-8410
Elena Ciobanu – https://orcid.org/0000-0002-8969-922X
Lucia Mazur-Nicorici – https://orcid.org/0000-0003-3983-8292
References
World Health Organization. Boron in drinking water. Background document for development of WHO guidelines for drinking-water quality. Geneva: WHO; 2009. 20 p.
Sinitsyna OO, Plitman SI, Ampleeva GP, Gil’denskiol’d OA, Ryashentseva TM. Essential elements and standards for their contents in drinking water. Health Risk Anal. 2020;(3):30-38. doi: 10.21668/health.risk/2020.3.04.eng.
Nielsen FH. Manganese, molybdenum, boron, silicon, and other trace elements. In: Marriott BP, Birt DF, Stallings VA, Yates AA, editors. Present knowledge in nutrition. 11th ed. Elsevier; 2020. Vol. 1: Basic nutrition and metabolism. P. 485-500.
Miljkovic D, Scorei RI, Cimpoiaşu VM, Scorei ID. Calcium fructoborate: plant-based dietary boron for human nutrition. J Diet Suppl. 2009;6(3):211-226. doi: 10.1080/19390210903070772.
Pizzorno L. Nothing boring about boron. Integr Med (Boulder). 2015;14(4):35-48.
Khaliq H, Juming Z, Ke-Mei P. The physiological role of boron on health. Biol Trace Elem Res. 2018;186(1):31-51. doi: 10.1007/s12011-018-1284-3.
Mogoșan GD, Biță A, Bejenaru LE, Bejenaru C, et al. Calcium fructoborate for bone and cardiovascular health. Biol Trace Elem Res. 2015;172(2):277-281. doi: 10.1007/s12011-015-0590-2.
Reyes-Izquierdo T, Nemzer B, Gonzalez AE, Zhou Q, Argumedo R, Shu C, et al. Short-term intake of calcium fructoborate improves WOMAC and McGill scores and beneficially modulates biomarkers associated with knee osteoarthritis: a pilot clinical double-blinded placebo-controlled study. Am J Biomed Sci. 2012;4(2):111-122. doi: 10.5099/aj120200111.
Ali Mahmood NM, Barawi OR, Hussain SA. Relationship between serum concentrations of boron and inflammatory markers, disease duration, and severity of patients with knee osteoarthritis in Sulaimani city. Nat J Physiol Pharm Pharmacol. 2016;6(1):27-31. doi: 10.5455/njppp.2015.5.0809201576.
Sosa Baldivia A, Ruiz Ibarra G, Etchevers Barra JD. Will boron be essential for human nutrition? Arch Latinoam Nutr [Internet]. 2016;66(1) [cited 2025 Jan 31]. Available from: https://www.alanrevista.org/ediciones/2016/1/art-10/.
AlRawi Z, Gorial F, AlShammary W, Muhsin F, AlNaaimi A, Sa S, et al. Serum boron concentration in rheumatoid arthritis: correlation with disease activity, functional class, and rheumatoid factor. J Exp Integr Med. 2013;3(1):9-15. doi: 10.5455/jeim.101112.or.053.
Price AK, de Godoy MRC, Harper TA, Knap KE, Joslyn S, Pietrzkowski Z, et al. Effects of dietary calcium fructoborate supplementation on joint comfort and flexibility and serum inflammatory markers in dogs with osteoarthritis. J Anim Sci. 2017;95(7):2907-2916. doi: 10.2527/jas.2017.1588.
Palacios C. The role of nutrients in bone health, from A to Z. Crit Revi Food Sci Nutr. 2006;46(8):621-8. doi: 10.1080/10408390500466174.
Rondanelli M, Faliva MA, Barrile GC, Cavioni A, Mansueto F, Mazzola G, et al. Nutrition, physical activity, and dietary supplementation to prevent bone mineral density loss: a food pyramid. Nutrients. 2022;14(1):74. doi: 10.3390/nu14010074.
UNICEF; Government of the Republic of Moldova. Calitatea apei, a sanitației și a practicilor de igienă în școlile din Moldova [Water quality, sanitation and hygiene practices in schools in Moldova]. Chisinau: UNICEF; 2009. Romanian.
European Parliament; Council of the European Union. Directive (EU) 2020/2184 of the European Parliament and of the Council of 16 December 2020 on the quality of water intended for human consumption. Official J European Union. 2020;L 435/1:1-62.
Republica Moldova, Parlamentul. [Republic of Moldova, The Parliament]. Legea Nr. 182 din 19.12.2019 privind calitatea apei potabile. [Law No. 182 of 19.12.2019 on drinking water quality]. Monitorul Oficial al Republicii Moldova. 2020;(1-2):art. 2. Romanian.
Racu M-V, Scorei IR, Pînzaru I. The role of boron in prevention of osteoarticular diseases and its distribution in the Republic of Moldova. One Health Risk Manag. 2021;2(4):54-64. doi: 10.38045/ohrm.2021.4.05.