

Introduction
Thyroid nodules are defined as abnormal, localized proliferations within the thyroid gland, and encompass a large spectrum of lesions, including colloid or cystic nodules, lymphocytic thyroiditis nodules, nodular or multinodular goiters, autonomously functioning nodules and tumors such as thyroid adenoma or carcinoma [1-3].
The incidence of thyroid nodules has increased over recent decades, largely due to the widespread use of imaging modalities such as neck ultrasonography, CT, and MRI, which frequently identify incidental nodules. Epidemiological studies suggest a strong correlation with aging, female sex, iodine deficiency, and exposure to ionizing radiation [4].
Current guidelines issued by professional societies provide frameworks for the evaluation of thyroid nodules followed by surveillance or treatment recommendations, which are usually based on cytologic results, while histopathological diagnosis remains the „gold standard” [5]. From this perspective, the management of thyroid nodules remains debatable regarding surgical indications, the extent of thyroidectomy, and the tactics in indeterminate or low-risk lesions.
Surgeons have a decisive role in the multidisciplinary management of patients with thyroid nodules, particularly when surgical treatment should be considered according to clinical, radiologic, or cytologic findings [6, 7].
The aim of our study is to optimize the diagnostic and surgical treatment strategies in patients with thyroid nodules through individualized approaches based on malignancy risk and clinico-imaging features.
Material and methods
This prospective study was conducted in the Department of Surgery No. 5 of the Nicolae Testemițanu State University of Medicine and Pharmacy, Chisinau, Republic of Moldova, between 2022 and the first semester of 2025. After applying inclusion criteria, 89 patients diagnosed clinically and/or radiologically with thyroid nodules were enrolled into the study. Prior to enrollment, all participants signed written informed consent forms in accordance with the approval of the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy Minutes No. 84, from June 07, 2017.
Diagnostic workup included initially medical history collection and physical examination. Thyroid hormonal status was assessed through TSH, FT4 and FT3 levels. In addition to standard investigations, the serum values of autoimmune markers - anti-TPO (anti-thyroperoxidase), anti-TG (anti-thyroglobulin) antibodies and the tumor marker - calcitonin, were determined for appraisal of the underlying etiology of thyroid nodules.
Neck ultrasonography was performed in all patients as a first-line imaging tool for the visualization of the thyroid gland and regional lymph nodes. Thyroid nodules were depicted by location, size, shape, composition, echogenicity, margins, presence of calcifications, and associated lymphadenopathy and were reported in categories according to the Thyroid Imaging Reporting and Data System (TI-RADS), as follows: TI-RADS 1 – normal thyroid gland; TI-RADS 2 – benign nodules; TI-RADS 3 – probably benign; TI-RADS 4 – suspicious for malignancy; TI-RADS 5 – probably malignant. Doppler mode and sonoelastography have enhanced the diagnostic value of ultrasonography by providing additional information on the vascular patterns and the elasticity of thyroid nodules.
Fine-needle aspiration biopsy (FNAB) was indicated in echographically suspicious for malignancy solitary or dominant thyroid nodules and cytological findings were interpreted and reported in accordance with the Bethesda System for Reporting Thyroid Cytopathology (TBSRTC): I – non-diagnostic or unsatisfactory; II – benign; III – atypia of undetermined significance or follicular lesion of undetermined significance; IV – follicular neoplasm or suspicious for a follicular neoplasm; V – suspicious for malignancy; VI – malignant.
Thyroid MRI (Magnetic Resonance Imaging) was used as an advanced imaging modality to evaluate possible extrathyroidal extension of disease and to determine the presence or extent of metastatic involvement in cervical lymph nodes, especially in cases where ultrasound findings were inconclusive.
Intraoperative frozen section (IFS) was performed in selected cases, particularly those with suspicious preoperative features or indeterminate cytological findings, in order to confirm the malignancy and had an important role in real-time surgical decision-making, especially in determining the volume of surgery – limitation to hemithyroidectomy or extension to total thyroidectomy.
Histopathological findings were crucial in confirming the final diagnosis and determining appropriate treatment strategies. The patients were actively monitored over a 24-month period to assess postoperative evolution and detect any signs of recurrence or complications.
The obtained data were processed and analyzed using IBM SPSS Statistics software, version 26.0 (IBM Corp., Armonk, NY) and Microsoft Excel. Absolute and relative values were calculated, expressed in frequencies (n) and percentages, while continuous variables were summarized using means and standard deviations. A 95% confidence interval (CI) was calculated to estimate the precision of observed effects, and a p-value < 0.05 was considered statistically significant in comparable variables.
Results
The study included 89 patients with thyroid nodules who met the inclusion criteria. The age of the patients ranged from 20 to 77 years, with a significant predominance of women - 78 (87.64%) cases (Table1).
The most commonly reported symptoms among patients included discomfort or pain during swallowing (n = 89; 100%), perceived as a “globus sensation”, unexplained fatigue (n = 72; 80.89 %), and a mass (lump) in the anterior cervical region (n = 45; 50.56%) (Table 1). Other less frequent complaints were emotional instability and irritability (n = 34; 38.2%), dyspnea (n = 14; 15.73%), and dysphonia (n = 3; 3.37%).
While most nodules exhibited a slow, symptomatic evolution, and patients were monitored by the family physician or endocrinologist, 12 patients (13.48%) experienced rapid nodule growth within a period ranging from 5 days to 6 months, which prompted earlier surgical referral. At the time of admission, most of the patients presented with unilateral lesions of the thyroid gland as solitary nodules (n = 38; 42.7%), or multinodularity of one lobe (n = 5; 5.61%). Bilateral lesions were consisted of multinodular goiter (n = 32; 35.97%) or toxic diffuse-nodular goiter (n = 8; 8.99%). It is important to note that nodule recurrence was documented in 4 cases (4.49%). Two cases involved contralateral lobe recurrence, one occurred following partial resection of the left thyroid lobe, and one case was identified after total thyroidectomy, according to the medical record excerpt. Combined lesions were present in 2 patients (2.25%). The demographic and clinical data of the patients are summarized in Table 1.
Table 1. Demographic and clinical characteristics of patients | |
Variable | Value (n, %, 95% CI) |
Mean age | 48.4 ± 14.2 years |
Gender Women Men Gender ratio |
78 (87.64 %) (95% CI: 80.8 - 94.5) 11 (12.36 %) (95% CI: 5.5 - 19.2) 7:1 (p < 0.0001) |
Complaints Discomfort or pain during swallowing Fatigue Lump in the anterior cervical region |
89 (100%) (95% CI: 100 - 100) 72 (80.89%) (95% CI: 72.7 - 89.1) 45 (50.56%) (95% CI: 40.2 - 60.9) |
Duration of the disease | 5 days – 20 years |
Preventive diagnosis Solitary nodule Multinodular goiter Toxic diffuse-nodular goiter Recurrence Cyst of the right lobe and isthmus nodule Left nodular goiter and left parathyroid adenoma |
38 (42.7%) (95% CI: 32.45 - 52.95) 37 (41.58%) (95% CI: 31.34-51.80) 8 (8.99%) (95% CI: 3.05 - 14.93) 4 (4.49%) (95% CI: 0.18 - 8.80) 1 (1.12%) (95% CI: 0 - 3.32) 1 (1.12%) (95% CI: 0 - 3.32) |
Comorbidities Diabetes mellitus, arterial hypertension, etc. |
5 (5.61%) (95% CI: 0.84 – 10.4) |
Note: The results were analyzed descriptively, presenting absolute numbers - n, percentages - %, and 95% confidence intervals – 95% CI. A chi-squared test was used to evaluate the relationship between the gender variables. The resulting p-value indicates a highly significant difference between genders. | |
Based on serum thyroid hormone levels, all patients were in a euthyroid hormonal status, which in 8 (8.99%) cases of toxic diffuse-nodular goiter was maintained through the administration of antithyroid medication. Although TSH levels were within the normal range in most cases, in 2 patients (2.25%) they were below the reference range, while FT3 and FT4 remained within normal limits (Table 2).
Elevated levels of either anti-thyroglobulin (Anti-TG) or anti-thyroid peroxidase (Anti-TPO) antibodies (not both simultaneously) were observed in 5 cases (5.61%), and revealed an autoimmune thyroiditis etiology of the nodules.
In 6 cases, serum calcitonin values exceeded 2.0 pg/ml and were associated with follicular adenoma (n = 2), and papillary carcinoma (n = 4). While elevated calcitonin is typically considered a marker for medullary thyroid carcinoma, its increase in these cases may suggest atypical secretion or cross-reactivity.
The ultrasound evaluation revealed that the size of thyroid nodules in greatest diameter in solitary lesions varied between 1.0 cm and 6.0 cm, and from 0.8 cm to 3.5 cm in multinodular lesions.
The majority of thyroid nodules were ultrasonographically classified as TI-RADS 4, followed by TI-RADS 3, while a smaller proportion were categorized as TI-RADS 5, which reflects a predominance of nodules with suspicious features. Doppler ultrasound revealed mixed vascular patterns in the evaluated nodules, while elastography demonstrated predominantly elastic tissue. Sonographic examination revealed laterocervical lymphadenopathy in two cases (Table 2).
FNAB was performed on solitary nodules or dominant nodules within unilateral multinodular goiters measuring 1.0 cm and larger. The distribution of cytological results among the TBSRTC categories was non-significant according to the frequencies (Table 2). Papillary carcinoma was histopathologically confirmed in one case from each category III and IV. In two cases reported as TBSRTC V, malignancy was not determined. Both cases classified as TBSRTC VI were diagnosed with papillary carcinoma. It is noteworthy that 10 patients declined FNAB due to concerns about potential bleeding or other complications.
MRI was used in three cases: two cases of suspicious cervical lymphadenopathy identified via ultrasonography, and in one case for a detailed assessment of a parathyroid lesion.
Table 2. Relevant investigations results | |
Variable | Value (n, %, 95% CI) |
TSH TSH ↓ | 1.8 ± 1.42 uIU/ml 2 (2.25%) (95% CI: 0 - 5.33) |
Hormonal status Euthyroidism Euthyroidism (maintained with antithyroid drugs) |
81 (91.01%) (95% CI: 85.10 - 96.90) 8 (8.99%) (95% CI: 3.10 - 14.80) |
Thyroid ultrasound TI-RADS 3 TI-RADS 4 TI-RADS 5 | 89 (100 %) (95% CI: 100 - 100) 30 (33.7%) (95% CI: 23.9 - 43.5) 52 (58.43%) (95% CI: 48.2 - 68.6) 7 (7.87%) (95% CI: 2.2 - 13.5) |
FNAB TBSRTC II TBSRTC III TBSRTC IV TBSRTC V TBSRTC VI | 13 (14.61%) (95% CI: 8.5 - 23.9) 3 (23.08%) (95% CI: 6.2 - 54.0) 2 (15.38%) (95% CI: 2.1 - 45.5) 3 (23.08%) (95% CI: 6.2 - 54.0) 3 (23.08%) (95% CI: 6.2 - 54.0) 2 (15.38%) (95% CI: 2.1 - 45.5) |
Anterior cervical region MRI Regional lymphadenopathy | 3 (3.37%) (95% CI: 0 - 7.06) 2 (2.25%) (95% CI: 0 - 4.89) |
IFS Benign Malignant | 5 (5.61%) (95% CI: 0.83 - 10.41) 4 (4.49 %) (95% CI: 0.20 - 8.78) 1 (1.12%) (95% CI: 0 - 3.28) |
Note: Descriptive analysis of categorical variables included absolute frequencies (n - number), relative frequencies (%- percentage), and corresponding 95% confidence intervals – 95% CI; TSH - thyroid stimulating hormone; TI-RADS - Thyroid Imaging Reporting and Data System; TBSRTC - Bethesda System for Reporting Thyroid Cytopathology; FNAB - fine-needle aspiration biopsy; MRI - Magnetic Resonance Imaging; IFS - Intraoperative frozen section. | |
Surgical indications were established based on the presence of nodules ≥ 1.0 cm with compressive symptoms, suspicious imaging features of nodules, rapid growth, cytological findings suggestive of malignancy, or the presence of multiple nodules ≥ 0.8 cm and with an association with elevated serum calcitonin values serving as a supplementary indication.
During preoperative assessment, 2 patients (2.25%) were identified with contraindications to surgery due to cardiac comorbidities associated with high anesthetic-surgical risk.
The extent of thyroidectomy was decided according to several factors, including the presence of unilateral or bilateral thyroid lesions, regional metastases, established guideline recommendations, patient preference, the age of the patient and IFS results.
Hemithyroidectomy was performed in patients with unilateral nodular lesions, indeterminate cytology, microcarcinomas, or encapsulated carcinoma, benign IFS results, as well as in 2 cases of bilateral multinodular goiter when the contralateral lesions measured between 3–5 mm. Total thyroidectomies were performed in patients with bilateral multiple lesions, confirmed or highly suspected or unforeseeable malignancy, malignant IFS result, and toxic diffuse-nodular goiter.
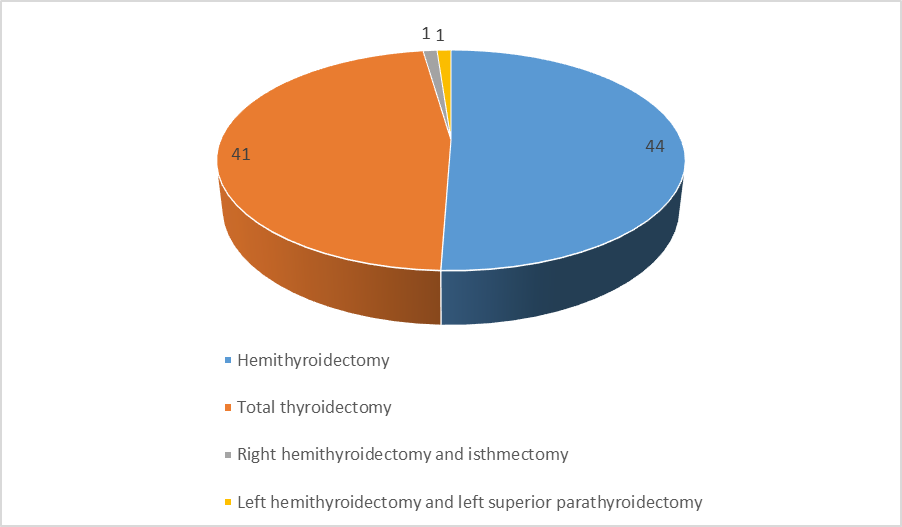
The most frequently performed surgery was hemithyroidectomy, carried out in 44 patients (49.41%, 95% CI: 39.11 - 59.77), followed by total thyroidectomy in 41 cases (46.09%, 95% CI: 35.75 - 56.43); right hemithyroidectomy with isthmectomy and left hemithyroidectomy combined with left superior parathyroidectomy were each performed in 1 patient (1.12%, 95% CI: 0 - 3.32) respectively (Figure 1).
|
Figure 1. Types of performed surgeries Note: The pie chart illustrates the distribution of the performed surgeries. Each slice represents the absolute number of surgical procedures, out of a total of 87 procedures. |
Completion thyroidectomy was performed in one patient, three months after initial hemithyroidectomy, due to histopathological confirmation of papillary thyroid carcinoma. The operation was indicated by the oncologist in order to initiate postoperative radioiodine therapy.
In two cases with preoperative suspicion of cervical lymphadenopathy, lymphadenectomy was not performed. In the first case, the tumor was locally advanced, with pathological lymph nodes firmly adherent to the carotid artery, rendering dissection contraindicated due to high surgical risk. In the second case, intraoperatively during revision, the lymph nodes were not identified.
Histopathological examination of the thyroid nodules confirmed a variety of benign and malignant entities, as detailed in table 3, with goiter being the most common finding, followed in frequency by follicular adenoma.
Table 3. Distribution of patients according to histopathological result | |||
Histopathological result | n | % | 95% CI |
Goiter | 52 | 59.77 | 49.15 - 70.00 |
Follicular adenoma | 16 | 18.40 | 10.50 - 26.30 |
Papillary carcinoma | 14 | 16.08 | 8.50 - 23.70 |
Colloidal cyst | 2 | 2.30 | 0 - 5.50 |
Papillary adenoma | 1 | 1.15 | 0 - 3.40 |
Oncocytic adenoma | 1 | 1.15 | 0 - 3.40 |
Thyroiditic nodule (de Quervain thyroiditis) | 1 | 1.15 | 0 - 3.40 |
Note: The histological results as categorical variables were analyzed descriptively, with reporting of n - absolute numbers, % - percentages, and 95% CI - 95% confidence intervals. | |||
In our study, it can be observed that the malignancy rate of thyroid nodules was 18.39%, with all malignant nodules being histologically confirmed as papillary thyroid carcinoma, probably reflecting the fact that this type represents the most prevalent form of thyroid malignancy.
The postoperative period was favorable in all the patients. Throughout the 24-month follow-up, no relapse of thyroid pathology and no complications were recorded. The mean duration of the hospital stay was 7.82 days. Thyroid hormone replacement therapy was adjusted individually by endocrinologists based on serum hormone levels. Patients who did not undergo surgery were followed up regularly.
Discussion
A rational and systematic assessment of thyroid nodules is fundamental to achieving successful outcomes, both in surgical and conservative management. Most guidelines and recent publications recommend measuring only the thyroid-stimulating hormone (TSH) [1, 2, 8, 9] as the first step in evaluating a thyroid nodule. We consider that the determination of the complete hormonal profile, of calcitonin, and of autoimmune antibodies is an essential component in the evaluation of thyroid nodules, as it provides valuable information for the etiological background, diagnosis, and risk stratification. Calcitonin has retained its important role as a single biomarker in the screening and early detection of medullary thyroid carcinoma, contributing significantly to preoperative diagnosis and appropriate surgical planning [10].
As highlighted by Grani et al. (2024), neck ultrasonography remains a cornerstone in the preoperative assessment of thyroid nodules [11]. Similarly, our study demonstrated that, within the appropriate clinical context and supplemented by Doppler mode and elastography, ultrasonography can often obviate the need for biopsy and serve as a reliable tool to guide surgical decision-making.
The role of ultrasonography is also crucial in the evaluation of both unilateral and bilateral multinodular goiters, whose management is poorly described in the literature. Although each nodule carries a risk of malignancy, we do not suggest performing multiple simultaneous biopsies, in accordance with guideline recommendations [1, 2, 8, 12, 13]. To exclude malignancy in unilateral thyroid disease and to assess intraoperatively the extent of thyroidectomy, we prefer to use IFS. This allowed us to adjust the volume of surgery based on intraoperative findings, thereby optimizing patient management. In cases of bilateral multinodular thyroid disease where nodules exceed 0.8 cm, we recommend total thyroidectomy to effectively prevent compressive symptoms such as dyspnea, dysphagia, and voice changes. This approach also reduces the risk of recurrent surgery and allows for comprehensive management of potentially malignant or symptomatic nodules.
In this context, thyroid nodules larger than 2 cm, which anatomically occupy approximately half of a thyroid lobe, can cause anterior neck deformities resulting in cosmetic concerns. When nodules extend posteriorly, they may induce compressive symptoms. Despite the absence of malignancy risk, such nodules warrant consideration for a surgical approach.
To prevent the recurrence of thyroid nodules, which varies between 8.9% and 40% (J. Rudnicki et al.), we advocate for the use of hemithyroidectomy and total thyroidectomy as standard surgical approaches [14]. Partial lobectomies or subtotal thyroidectomies, although historically performed, are associated with a higher risk of disease recurrence due to the potential persistence of residual nodular tissue.
Conclusions
Thyroid nodules remain a significant clinical concern due to their potential for malignancy and their capacity to produce compressive symptoms on adjacent cervical structures. They necessitate careful clinical, laboratory, and imaging evaluation and ongoing surveillance. The timing and indications for surgery must result from a multidisciplinary collaboration involving endocrinologists, family physicians, radiologists, and surgeons, to develop an evidence-based and personalized management plan for patients with suspicious nodules, which is fundamental for ensuring accurate diagnosis, appropriate treatment, and prevention of disease recurrence or progression.
Competing interests
None declared.
Authors’ contributions
AB and CC had a crucial role in the conception and design of the work, acquisition and analysis of data. Both authors interpreted the data, drafted and critically reviewed this article. All authors have approved final version of this paper for publication.
Patient consent
Obtained.
Ethics approval
The study was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes no. 84, dated 07.06.2017).
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Authors’ ORCID IDs
Alin Bour - https://orcid.org/0000-0001-6316-0763
Cristina Cojocaru - https://orcid.org/0000-0001-9814-5467
References
Durante C, Hegedüs L, Czarniecka A, Paschke R, Russ G, Schmitt F, Soares P, Solymosi T, Papini E. 2023 European Thyroid Association Clinical Practice Guidelines for thyroid nodule management. Eur Thyroid J. 2023;12(5):e230067. https://doi.org/10.1530/ETJ-23-0067.
Gharib H., Papini E, Garber JR, Duick DS, Harrell RM, Hegedüs L, et al.; AACE/ACE/AME Task Force on Thyroid Nodules. American Association of Clinical Endo crinologists, American College of Endocrinology, and Associazione Medici Endocrinologi Medical Guidelines for clinical practice for the diagnosis and management of thyroid nodules - 2016 Update. Endocr Pract. 2016;22(5):622-39. doi: 10.4158/EP161208.GL.
Hamill C, Ellis P, Johnston PC. Ultrasound for the as sessment of thyroid nodules: an overview for non-radiologists. Br J Hosp Med (Lond). 2022;83(7):1-7. doi: 10.12968/hmed.2022.0071.
Mu C, Ming X, Tian Y, Liu Y, Yao M, Ni Y, Liu Y, Li Z. Mapping global epidemiology of thyroid nodules among general population: a systematic review and meta-analysis. Front Oncol. 2022;12:1029926. doi: 10.3389/fonc.2022.1029926.
Tobcu E, Karavaş E, Yılmaz GT, Topçu B. Comparison of K-TIRADS, EU-TIRADS and ACR-TIRADS Guidelines for malignancy risk determination of thyroid nodules. Diagnostics. 2025;15(8):1015. https://doi. org/10.3390/diagnostics15081015.
Scheller B, Culié D, Poissonnet G, Dassonville O, D’Andréa G, Bozec A. Recent advances in the surgical management of thyroid cancer. Curr Oncol. 2023;30(5):4787-4804. doi: 10.3390/curroncol30050361.
Cojocaru C, Bour A. The time for surgery in thyroid 32 nodules. Med Surg J - Rev Med Chir Soc Med Nat, Iaşi. 2022;126(4):520-527. doi: 10.22551/MSJ.2022.04.08.
Kant R, Davis A, Verma V. Thyroid nodules: advances in evaluation and management. Am Fam Physician. 2020;102(5):298-304.
Uludag M, Unlu MT, Kostek M, Aygun N, Caliskan O, Ozel A, Isgor A. Management of thyroid nodules. Sisli Etfal Hastan Tıp Bul. 2023;57(3):287-304. doi: 10.14744/SEMB.2023.06992.
Broecker-Preuss M, Simon D, Fries M, Kornely E, Weber M, Vardarli I, Gilman E, Herrmann K, Görges R. Update on calcitonin screening for medullary thyroid carcinoma and the results of a retrospective analysis of 12,984 patients with thyroid nodules. Cancers (Basel). 2023;15(8):2333. https://doi.org/10.3390/cancers15082333.
Grani G, Sponziello M, Filetti S, Durante C. Thyroid nodules: diagnosis and management. Nat Rev Endocrinol. 2024;20(12):715-728. doi: 10.1038/s41574-024-01025-4.
Lam S, Lang BHH. A review of the pathogenesis and management of multinodular goiter [Internet]. In: Soto GD, editor. Thyroid disorders - focus on hyperthyroidism. InTech; 2014 [cited 2025 May 12]. Available from: http://dx.doi.org/10.5772/57547.
Cojocaru C, Bour A. The current assessment and management of thyroid nodules. Mold J Health Sci. 2023;1(10):73-81. https://doi.org/10.52645/MJHS.2023.1.11.
Rudnicki J, Agrawal AK, Jelen M, Sebastian M, Sroczyński M, Zyśko D. Histopathological evaluation of recurrent goiter. Folia Histochem Cytobiol. 2010 Sep 30;48(3):430-3. doi: 10.2478/v10042-010-0036-9.