
Introduction
The Coronavirus disease 19 (COVID-19) pandemic remains the biggest challenge facing healthcare systems around the world. Although the respiratory system is the primary target of SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus 2), other systems and organs can also be affected by the virus via the circulatory system, including the renal system. Reports indicate that kidney involvement is common and ranges from mild proteinuria to severe acute kidney injury (AKI) [1, 2]. The pathogenetic mechanisms by which SARS-CoV-2 induces the development of AKI remain unclear; however, studies suggest that AKI appears to be closely related to the direct action of the virus on the kidneys [3].
Even though early in the pandemic, reports from China suggested low rates of kidney damage (0.5%), studies from the USA and Europe have reported increasing rates of AKI, particularly in intensive care settings, where approximately 45% of patients require renal replacement therapy [4, 5]. A 2020 meta-analysis reported that the combined incidence of AKI among hospitalized COVID-19 patients was 28.6% in the USA and Europe and 5.5% in China. Worldwide, among patients admitted to intensive care units, it is estimated that 29% develop AKI, and this proportion rises to 78% in those requiring intubation [6]. According to a 2022 study, AKI is a frequent complication of SARS-CoV-2 infection, with a cumulative incidence of 19.76% and a mortality rate exceeding 54.24% [7]. Differences in results may be due to the population studied and the definitions of AKI used.
Since the beginning of the pandemic, 607,450 cases of COVID-19 have been registered in the Republic of Moldova. From the total number of registered cases, 5,145 patients were admitted to the Timofei Moșneaga Republican Clinical Hospital, of which 10% (514) developed acute kidney injury. Of the total number, 80.68% (4,151) of patients had a favorable evolution, but 19.32% (994) died.
Therefore, the aim of the study was to establish the dynamics of COVID-19 in patients who develop AKI and to identify risk factors for developing AKI associated with COVID-19.
Material and methods
This retrospective descriptive study was carried out based on the clinical observation sheets of a group of 40 patients, of both sexes, aged between 37 and 88 years (mean age 64.08 ± 10.04 years). The inclusion criterion was the development of AKI secondary to COVID-19, and the exclusion criterion was the absence of signs of kidney damage. The analysis of the clinical observation sheets of these patients was carried out using a questionnaire that included the following criteria: age, sex, day of illness at admission, vaccination status, symptoms at admission, comorbidities, laboratory investigations (general urinalysis, complete blood count, biochemical blood analysis, inflammatory markers, coagulation tests), instrumental investigations (pulmonary radiography), treatment, need for mechanical ventilation, discharge status, and death. For each patient, data were collected on three different days: the day of admission (first investigation), during hospitalization (second investigation), and the last day of hospitalization (third investigation), which allowed us to identify the development of AKI and its dynamic evolution. Statistical analysis of the data was performed using the Student’s t-test.
Results
The clinical observation sheets were studied as a whole to observe the evolution of the patients' condition over time and to determine the existence of a correlation between COVID-19 infection and kidney damage. The patients included in the study were admitted to the COVID-19 Intensive Care Unit on the 8.66 ± 3.76 day of illness in a serious condition. According to the epidemiological history, 5% (n = 2) of the patients were vaccinated: one had received two doses of the Pfizer/BioNTech vaccine, and one had received a single dose of the Jonhson&Jonhson (Janssen) vaccine; 15% (n = 6) were not vaccinated, and for 80% (n = 32), vaccination status was not documented. Initially, the patients' symptoms at admission were studied. It was determined that all 40 patients presented with typical symptoms of SARS-CoV-2 infection: low-grade fever - 27.50% (n = 11), fever - 62.50% (n = 25), wet cough - 15% (n = 6), dry cough - 62.50% (n = 25), general weakness - 97.50% (n = 39), headache - 52.50% (n = 21), dyspnea - 95% (n = 38), myalgia - 37.50% (n = 15), chills - 7.50% (n = 3), hypogeusia - 7.50% (n = 3), hyposmia - 7.50% (n = 3). Additionally, 80% (n = 32) did not present with any symptoms of kidney damage at admission.
The comorbidities identified in the studied patients were consistent with those described in the specialized literature and had the following frequencies: chronic cardiovascular diseases - 95% (n = 38), diabetes - 50% (n = 20), obesity - 52.50% (n = 21), chronic kidney disease (CKD) - 35% (n = 14), chronic kidney disease on dialysis - 5% (n = 2), and other conditions - 57.5% (n = 23). These comorbidities can be considered decisive factors in the development of AKI.
Analyzing the laboratory investigations, it was found that from the first day of hospitalization, patients already presented changes suggestive of kidney damage. In the general urinalysis, hematuria, leukocyturia, and proteinuria were observed, with values worsening over the course of the disease. As shown in Figure 1, on the day of hospitalization (urinalysis I), the following results were recorded: erythrocytes – mean 19.75/HPF, 95% CI: 7.27-32.26, p < 0.001; leukocytes – 10.47/HPF, 95% CI: 2.25-23.19, p = 0.10; proteins – 0.73 g/L, 95% CI: 0.49-0.97, p < 0.001. During hospitalization (urinalysis II): erythrocytes – 23.96/HPF, 95% CI: 12.26-35.69, p < 0.001; leukocytes – 6.21/HPF, 95% CI: 3.62-8.79, p < 0.001; proteins – 0.68 g/L, 95% CI: 0.49-0.87, p < 0.001. On the last day of hospitalization (urinalysis III): erythrocytes – 32.15/HPF, 95% CI: 13.75-50.56, p < 0.001; leukocytes – 9.83/HPF, 95% CI: 4.42-15.24, p < 0.001; proteins – 0.75 g/L, 95% CI: 0.53-0.97, p < 0.001. The difference between the values on the first and last day of hospitalization was statistically significant (p < 0.001).
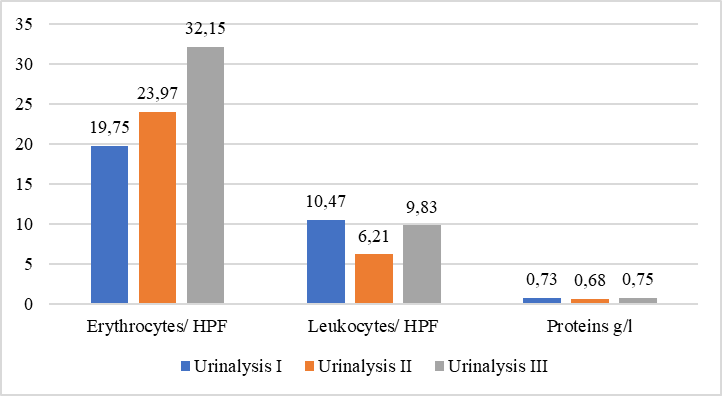 |
Fig. 1 Urinalysis values in dynamics Note: Urinalysis I –day of admission, Urinalysis II – during hospitalization, Urinalysis III – last day, HPF – High-Power Field. |
The presence of a severe inflammatory syndrome was also observed, being associated with an increased severity of COVID-19. This was demonstrated by the dynamic analysis of inflammatory markers. On the day of admission (urinalysis I), the following values were recorded: ESR – 36.57 mm/h, 95% CI: 31.17-41.97, p < 0.001: CRP – 624.18 mg/dl, 95% CI: 435.71-1684.08, p = 0.24; LDH – 447.74 U/l, 95% CI: 378.3-517.13, p < 0.001. During hospitalization (urinalysis II): ESR – 39.30 mm/h, 95% CI: 34.54-44.05, p < 0.001; CRP – 119.31 mg/dl, 95% CI: 90.06-148.55, p < 0.001; LDH – 606.91 U/l, 95% CI: 342.99-871.84, p < 0.001. On the last day (urinalysis III): ESR – 40.72 mm/h, 95% CI: 34.62-46.82, p < 0.001; CRP – 208.89 mg/dl, 95% CI: 66.19-531.59, p = 0.003; LDH – 550.98 U/l, 95% CI: 369.27-733.70, p < 0.001. According to these results, the difference in ESR, CRP, and LDH values between the first, second, and third measurements were statistically significant (p < 0.001), except for CRP on admission (p = 0.24), which was not statistically significant.
Studies report that in severe forms of COVID-19, where there is a considerable increase in cytokine levels, there is also a marked increase in ferritin, which is much higher in patients showing signs of kidney damage. Thus, ferritin can serve as a marker of severity and prognosis in SARS-CoV-2 infection [8].
The presence of elevated ferritin levels was also attested in our study from the day of admission and continued to increase dynamically along with the progression of COVID-19, a fact that confirms the data from the literature. On the first day (ferritin I) – 787.21 ng/ml, 95% CI: 601.50-972.93, p < 0.001; during hospitalization (ferritin II) – 943.59 ng/ml, 95% CI: 749.78-1137.39, p < 0.001; and on the last day (ferritin III) – 1029.00 ng/ml, 95% CI: 833.87-1224.12, p < 0.001. The values were statistically significant for p < 0.001.
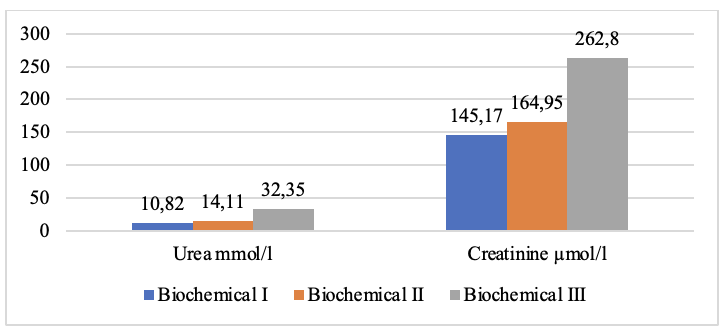
To establish the presence of AKI, markers of renal function – urea and creatinine – were studied. Following Figure 2, we notice that on the day of admission (biochemical I), the average value of urea was 10.82 mmol/l, 95% CI: 8.29-13.34, p < 0.001, and of creatinine 145.17 µmol/l, 95% CI: 73.73-216.62, p < 0.001. These data demonstrate that signs of renal function impairment were present even before the patients were admitted and showed a negative dynamic over time, especially after the initiation of mechanical ventilation through orotracheal intubation. During hospitalization (biochemical II), the average value of urea was 14.11 mmol/l, 95% CI: 11.83-16.40, p < 0.001, and of creatinine 164.95 µmol/l, 95% CI: 110.34-219.62, p < 0.001. On the last day (biochemical III), the average value of urea was 32.35 mmol/l, 95% CI: 27.3-37.3, p < 0.001, and of creatinine 262.80 µmol/l, 95% CI: 207.49-318.11, p < 0.001. Of the total number of 40 patients, 10% (n = 4) required renal replacement therapy. The values were statistically significant for p < 0.001.
|
Fig. 2 Markers of renal function in dynamics Note: Biochemical I – the day of admission, Biochemical II – during hospitalization, Biochemical III – last day. |
Analyzing the dynamic coagulation tests of the patients, a deviation in their values was observed, indicating a state of hypocoagulation, in contrast to data reported in the literature, where it is stated that patients with severe forms of COVID-19 typically develop a hypercoagulable state. This discrepancy may be attributed to the high doses of anticoagulants used in the treatment of COVID-19. On the day of hospitalization (coagulation tests I), the mean value of PT was 74.64%, 95% CI: 68.56-80.72, p < 0.001; INR – 1.44, 95% CI: 1.39-1.49, p < 0.001; fibrinogen – 4.30 g/l, 95% CI: 3.85-4.75, p < 0.001; aPTTT – 36.69 sec, 95% CI: 32.01-41.37, p < 0.001. During hospitalization (coagulation tests II), PT – 70.93%, 95% CI: 67.60-74.27, p < 0.001; INR – 1.68, 95% CI: 1.08-2.27, p < 0.001; fibrinogen – 5.20 g/l, 95% CI: 2.84-7.55, p < 0.001; aPTT – 44.14 sec, 95% CI: 39.49-48.78, p < 0.001. On the last day (coagulation tests III), PT – 67.62%, 95% CI: 63.19-72.05, p < 0.001; INR – 1.51, 95% CI: 1.30-1.60, p < 0.001; fibrinogen – 4.12 g/l, 95% CI: 3.70-4.53, p < 0.001, aPTT – 43.87 sec, 95% CI: 38.65-49.09, p < 0.001. All values were statistically significant (p < 0.001).
Analyzing the treatment regimens of the patients included in the study, the use of several drugs with nephrotoxic effects was identified, which could be considered additional potential factors in the development of AKI in patients with COVID-19. The identified drugs were as follows: vancomycin – 22.5% (n = 9), colistin – 40% (n = 16), gentamicin – 20% (n = 8), amikacin – 10% (n = 4), lopinavir/ritonavir (Aluvia) – 10% (n = 4), ascorbic acid – 90% (n = 36), hydroxychloroquine – 10% (n = 4), and others – 92.5% (n = 37), including ciprofloxacin, meropenem, pospenem, imipenem with cilastatin, ampicillin, amoxicillin with clavulanic acid, piperacillin with tazobactam, cefoperazone with sulbactam, and cefazolin. All patients (100%, n = 40) received combinations of two or more of the above-mentioned drugs as part of their treatment regimens. The development of AKI in patients with COVID-19 may also be explained by the lung-kidney interaction. Respiratory failure can trigger AKI through systemic hypoxia, which develops in patients with severe forms of COVID-19, as well as through hypercapnia and even mechanical ventilation [9]. Therefore, we can conclude that the degree of lung damage is correlated with kidney injury and the development of AKI. The greater the degree of pulmonary damage, the earlier mechanical ventilation is instituted, which may lead to the development of early AKI. Evaluating the results of chest radiographs, it was determined that on the day of admission (radiograph I), the degree of lung damage had an average of 66.90% ± 13.82, 95% CI: 62.48-71.32, p < 0.001. During hospitalization (radiograph II), the degree of lung damage was 68.38% ± 11.78, 95% CI: 64.60-72.15, p < 0.001. On the last day (radiograph III), it reached 69.00% ± 10.20, 95% CI: 65.74-71.26, p < 0.001. The differences between the radiographic values were statistically significant (p < 0.001).
All patients (100%, n = 40) were mechanically ventilated via orotracheal intubation for a mean duration of 7.73 ± 5.09 days. The average length of hospitalization was 15.43 ± 7.63 days. The clinical course in all patients (100%, n = 40) was fulminant and ended in death.
Discussions
Being a pathology with predominant damage to the respiratory system, COVID-19 can also affect other systems and organs, including the kidneys, which are particularly susceptible to infection with the SARS-CoV-2 virus, with AKI being the most common manifestation of kidney damage.
The consequences of the COVID-19 pandemic are drastic. Evidence shows that patients with CKD or those with risk factors for developing kidney disease are significantly affected. Patients with CKD undergoing renal replacement therapy and those with a kidney transplant are at higher risk of complications from COVID-19, while patients with severe forms of SARS-CoV-2 infection are at increased risk of developing AKI, with devastating consequences both in the short and long term [10].
It is well known that in severe forms of infection with the SARS-CoV-2 virus, a cytokine storm occurs, causing a considerable elevation of inflammatory markers and the release of a large number of cytokines into the circulation. Subsequently, a state of shock, hypoxia, and rhabdomyolysis can develop, which may eventually lead to the onset of AKI [11]. In kidney damage, an important role is played by the drug treatment administered to patients with COVID-19. The administration of drugs with nephrotoxic potential, such as aminoglycosides, vancomycin, and colistin, has been reported as a major risk factor in the development of AKI in patients infected with SARS-CoV-2. Even though beneficial effects of antiviral treatment with Remdesivir have been reported, it can also exert nephrotoxic effects through mitochondrial damage in renal tubular cells, especially when used in high doses. Cases of AKI associated with Lopinavir and low-dose Ritonavir therapy have also been reported during the management of COVID-19 [12]. Another drug commonly used in the treatment of COVID-19 is ascorbic acid. In addition to its antioxidant properties, it can lead to hyperoxaluria with severe and irreversible AKI, especially in patients with pre-existing CKD. Therefore, it is necessary to take renal function into account before using high doses of vitamin C [13]. During the first phase of the pandemic, hydroxychloroquine was used in the standard treatment protocols for COVID-19 patients. In addition to its antimalarial activity, it also possesses anti-inflammatory properties. As the pandemic evolved, it was found that hydroxychloroquine could contribute to AKI by increasing lysosomal pH and inhibiting autophagy. However, the results remain controversial, as other studies show that hydroxychloroquine does not have direct nephrotoxic activity, with toxicity likely potentiated by the drug combinations [11, 14].
Studies show that mechanical ventilation alters systemic hemodynamics and neurohormonal status. It can lead to changes in renal perfusion due to increased intrathoracic pressure, elevated pulmonary vascular resistance, and increased central venous pressure, which together reduce venous return and contribute to right ventricular dysfunction [15, 16].
In this study, the most common factors identified as decisive in the development of AKI in COVID-19 patients were advanced age, the presence of multiple comorbidities such as chronic cardiovascular diseases, diabetes mellitus, obesity, chronic kidney disease, mechanical ventilation via orotracheal intubation, and the use of drugs with nephrotoxic potential. Hospitalized at 8.66 ± 3.76 days after symptom onset, the patients were in serious condition, with evident signs of kidney damage that continued to worsen over time. Urinalysis revealed proteinuria, hematuria, and leukocyturia from the day of admission. Urea and creatinine levels were elevated on admission and continued to rise, with urea increasing from 10.82 mmol/l to 32.35 mmol/l and creatinine from 145.17 μmol/l to 262.80 μmol/l; 10% of patients required renal replacement therapy. These changes were associated with considerable increases in inflammatory markers: ESR rose from 36.57 mm/h to 40.72 mm/h, CRP from 624.18 mg/dl to 208.89 mg/dl, LDH from 447.74 U/l to 550.98 U/l, and ferritin from 787.21 ng/ml to 1029.00 ng/ml–values that were directly proportional to the severity of the patients' condition. Based on these results, we cannot accurately specify the etiology and mechanisms underlying AKI in COVID-19 patients, but it is clear that once AKI develops, the disease progression is fulminant.
Conclusions
Acute kidney injury is a frequent and severe complication among mechanically ventilated intensive care unit patients with COVID-19, often associated with rapid deterioration and high mortality.
This study highlights the significant contribution of comorbidities and nephrotoxic drugs to AKI development in this population.
Our findings underscore the need for increased vigilance and early monitoring of the renal status to improve outcomes in critically ill COVID-19 patients.
Competing interests
None declared.
Authors’ contributions
All authors participated in the design of the study and had significant contributions to the drafting of the manuscript. All authors reviewed the work critically and approved the final version of the manuscript.
Informed consent for publication
Obtained.
Acknowledgements and funding
No external funding.
Ethics approval
The study was approved by the Ethics Committee of the Timofei Moșneaga Republican Clinical Hospital (Minutes No. 11, from 29.07.2025)
Provenance and peer review
Not commissioned, externally peer-reviewed.
Authors’ ORCID IDs
Marinela Murea –https://orcid.org/0009-0007-7350-4495
Andrei Bradu – https://orcid.org/0000-0001-7285-8717
Andrei Oprea – https://orcid.org/0000-0001-9269-5468
Andrei Galescu – https://orcid.org/0000-0002-7953-2450
Emil Ceban –https://orcid.org/0000-0002-1583-2884
References
Ahmadian E, Hosseiniyan Khatibi SM, Razi Soofiyani S, Abediazar S, Shoja MM, Ardalan M, et al. COVID-19 and kidney injury: pathophysiology and molecular mechanisms. Rev Med Virol. 2021;31(3):e2176. doi: 10.1002/rmv.2176.
Cheng Y, Luo R, Wang K, Zhang M, Wang Z, Dong L, et al. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020;97(5):829-38. https://doi.org/10.1016/j.kint.2020.03.005.
Sabaghian T, Kharazmi AB, Ansari A, Omidi F, Kazemi SN, Hajikhani B, et al. COVID-19 and acute kidney injury: a systematic review. Front Med (Lausanne). 2022;9:705908. doi: 10.3389/fmed.2022.705908.
Izzedine H, Jhaveri KD. Acute kidney injury in patients with COVID-19: an update on the pathophysiology. Nephrol Dial Transplant. 2021;36(2):224-6. doi: 10.1093/ndt/gfaa184.
Legrand M, Bell S, Forni L, Joannidis M, Koyner JL, Liu K, et al. Pathophysiology of COVID-19-associated acute kidney injury. Nat Rev Nephrol. 2021;17(11):751-764. doi: 10.1038/s41581-021-00452-0.
Fu EL, Janse RJ, De Jong Y, Van Der Endt VHW, Milders J, Van Der Willik EM, et al. Acute kidney injury and kidney replacement therapy in COVID-19: a systematic review and meta-analysis. Clin Kidney J. 2020 Sep 2;13(4):550-563. doi: 10.1093/ckj/sfaa160.
Raina R, Mahajan ZA, Vasistha P, Chakraborty R, Mukunda K, Tibrewal A, et al. Incidence and outcomes of acute idney injury in COVID-19: a systematic review. Blood Purif. 2022;51(3):199-212. doi: 10.1159/000514940.
Kaushal K, Kaur H, Sarma P, Bhattacharyya A, Sharma DJ, Prajapat M, et al. Serum ferritin as a predictive biomarker in COVID-19. A systematic review, meta-analysis and meta-regression analysis. J Crit Care. 2022;67:172-81. doi: 10.1016/j.jcrc.2021.09.023.
Hu B, Guo H, Zhou P, Shi ZL. Characteristics of SARS-CoV-2 and COVID-19. Nat Rev Microbiol. 2021;19(3):141-154. doi: 10.1038/s41579-020-00459-7.
Jager KJ, Kramer A, Chesnaye NC, Couchoud C, Sánchez-Álvarez JE, Garneata L, et al. Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int. 2020;98(6):1540-8doi: 10.1016/j.kint.2020.09.006.
Mauthe M, Orhon I, Rocchi C, Zhou X, Luhr M, Hijlkema KJ, et al. Chloroquine inhibits autophagic flux by decreasing autophagosome-lysosome fusion. Autophagy. 2018;14(8):1435-55. doi: 10.1080/15548627.2018.1474314.
Gérard AO, Laurain A, Fresse A, Parassol N, Muzzone M, Rocher F, et al. Remdesivir and acute renal failure: a potential safety signal from disproportionality analysis of the WHO safety database. Clin Pharmacol Ther. 2021;109(4):1021-1024. doi: 10.1002/cpt.2145.
Lemee N, Chamley P, Francois A, Guincestre T, Duval M, Promerat A, et al. MO116: Vitamin C nephrotoxicity in a COVID-19 patient: a case report. Nephrol Dial Transplant. 2022;37(Suppl 3):i168. https://doi.org/10.1093/ndt/gfac066.019.
Liao ZM, Zhang ZM, Liu Q. Hydroxychloroquine/chloroquine and the risk of acute kidney injury in COVID-19 patients: a systematic review and meta-analysis. Ren Fail. 2022;44(1):415-25. doi: 10.1080/0886022X.2022.2046609.
Chong WH, Saha BK. Relationship between severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and the etiology of acute idney injury (AKI). Am J Med Sci. 2021;361(3):287-96. doi: 10.1016/j.amjms.2020.10.025.
Li Z, Wu M, Yao J, Guo J, Liao X, Song S, et al. Caution on kidney dysfunctions of COVID-19 patients. medRxiv. 2020;2020.02.08.20021212. doi: 10.1101/2020.02.08.20021212.