
Introduction
The accurate measurement and understanding of the esophageal hiatus's anatomical and functional characteristics are crucial in the context of hiatal hernia (HH) diagnosis and surgical treatment. Disorders associated with the esophageal hiatus, particularly HHs, have become increasingly relevant in clinical practice due to their association with gastroesophageal reflux disease (GERD) and their impact on patient quality of life. HHs occur when the stomach protrudes through the enlarged esophageal hiatus into the thoracic cavity, often leading to significant clinical symptoms such as heartburn, regurgitation, and chest pain. HHs and GERD present significant clinical challenges due to their complex anatomy and the risk of postoperative complications such as dysphagia, gas-bloat syndrome and recurrent herniation. The prevalence of HHs and GERD is estimated to range from 10% to 50% in the adult population, with higher rates observed in older adults [1].
Historically, the management of HHs and GERD has focused on both conservative treatments, such as lifestyle modifications and pharmacotherapy, and surgical interventions, particularly in cases where conservative measures fail or complications occur. Currently, laparoscopic fundoplication (LF) remains the gold standard in antireflux surgery for HH and GERD, with excellent symptomatic results in 90% to 95% of cases [2, 3]. The surgical approach to HHs, however, has been a topic of ongoing debate, particularly regarding the best methods to ensure effective and durable repairs. The recurrence of HHs post-surgery, which has been reported in up to 10-30% of cases [4, 5], underscores the need for precise and individualized surgical techniques.
The integration of these advanced methodologies into the surgical workflow is particularly crucial in the context of an aging population, where the incidence of HHs is expected to increase. With the prevalence of GERD also on the rise, estimated to affect up to 20% of the adult population in Western countries [1], the need for effective and durable surgical solutions is more pressing than ever. The adoption of standardized measurement techniques, such as those proposed by Granderath and validated by Moten and Ouyang [6, 7], is likely to play a key role in addressing this challenge, providing surgeons with the tools they need to deliver optimal care.
The accurate assessment of the esophageal hiatus is a critical determinant of the success of HH and GERD surgery. The evolution of measurement techniques, from subjective intraoperative assessments to advanced imaging-based methods, represents a significant improvement in this field. As the surgical community continues to refine these approaches, the combination of intraoperative and imaging-based assessments will likely become a cornerstone of HH management, ultimately leading to improved patient outcomes and reduced rates of postoperative adverse events.
Material and methods
The study was conducted within the Department of General surgery and semiology no. 3 at Nicolae Testemițanu State University of Medicine and Pharmacy, at the General Surgery Clinic of the Gheorghe Paladi Municipal Hospital, Chisinau, Republic of Moldova. It involved 25 adult patients diagnosed with GERD with/or HH, all of whom underwent LF. The research was designed as a prospective, descriptive, observational and cross-sectional study aimed at assessing a novel intraoperative method for quantifying the HSA and its correlation with symptom severity and hernia recurrence. The study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Protocol No. 84, 20.06.2017). Informed consent was obtained from all participants.
Patient selection and surgical procedure. This study included 25 consecutive patients diagnosed with GERD and HH who were scheduled for elective LF. Patient inclusion criteria consisted of adults with a confirmed diagnosis of HH, and with preoperative symptoms of GERD. Patients with gross adhesions due to previous surgical interventions on the upper abdomen were excluded from this study.
To ensure uniformity and reproducibility of intraoperative measurements, all procedures were performed under general anesthesia using a laparoscopic approach with pneumoperitoneum established at 12–14 mmHg. During each surgery, standard laparoscopic techniques were employed, and exposure of the esophageal hiatus was achieved by systematic division of the phrenoesophageal ligament, hepatogastric ligament and atraumatic mobilization of the gastroesophageal junction, thereby facilitating clear identification of both diaphragmatic crura and optimal visualization for cruroplasty and fundoplication. After complete dissection and visualization of the esophageal hiatus, we proceeded with digital intraoperative imaging to assess the surface area of the defect.
Intraoperative imaging and analysis
To obtain accurate measurements of the hiatal defect, intraoperative digital photographs were taken. A digital camera mounted on a laparoscopic instrument with an adjustable lens (Olympus, Tokyo, Japan) was used to capture images under consistent lighting and focal distance settings to maintain measurement accuracy. A standardized "benchmark" reference object of known size (1.0 cm x 1.0 cm square) was placed within the operative field adjacent to the hiatal defect for calibration purposes. This benchmark was positioned in the same plane as the hiatal defect to avoid distortions from depth or angle, and all images were taken perpendicular to the plane of the defect to ensure consistency across measurements.
After obtaining the images, they were analyzed using ImageJ graphic software (National Institute of Mental Health, Bethesda, Maryland, USA), a free, open-source and commonly used tool for quantitative image analysis. The images were first converted to grayscale for enhanced contrast and ease of boundary definition. Each image was calibrated using the benchmark object, with the known area (1 cm²) used to set a pixel-to-square centimeter ratio. This ratio was critical in accurately quantifying the hiatal defect area. Each image was independently assessed by two experienced surgeons to assess inter-observer reliability, and each observer repeated the measurements twice at different time points to assess intra-observer reliability.
Measurement procedure
Calibration: In each image, the benchmark square was manually selected and designed as a standard reference using the ImageJ calibration function. The software calculated the pixel-to-centimeter ratio based on the 1.0 cm x 1.0 cm benchmark area.
Hiatal defect contouring: The hiatal defect was then contoured manually using the “Freehand Selection” tool in ImageJ, which allowed precise outlining of the defect’s irregular shape (Figure 1). Care was taken to include the full visible boundary of the defect while excluding surrounding tissues.
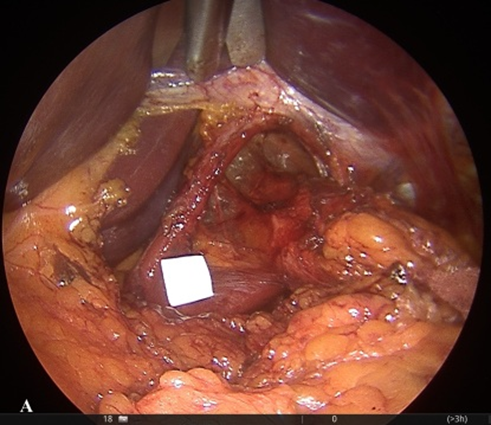 | 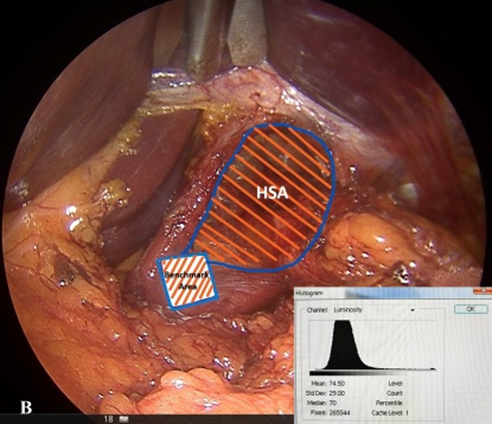 |
Fig. 1 Intraoperative method of HSA measurement. A - Intraoperative view of the esophageal hiatus, with a 1.0 × 1.0 cm square-shaped calibration benchmark placed adjacent to the defect for surface area measurement. B - Intraoperative analysis in ImageJ software: the hiatal contour is manually delineated, and the calculated area (in cm²) is based on pixel-to-size conversion using the internal calibration marker. Note: HSA – hiatal surface aria | |
Area calculation: After contouring, the software calculated the total pixel area of the defect. Using the previously established pixel-to-centimeter ratio, the area of the hiatal defect was calculated in square centimeters. This calculation was based on the proportional relationship between the number of pixels in the benchmark and the contoured defect area, expressed as:
![]()
Additional data. In addition to surface area quantification, we recorded demographic data, BMI, hernia type, and preoperative GERD-HRQL scores. All patients underwent fundoplication and posterior crural closure using nonabsorbable sutures, with or without mesh reinforcement, based on intraoperative judgment. Postoperative follow-up was performed at 3 and 12 months. At 12 months, patients were re-evaluated using the same GERD-HRQL instrument to assess clinical evolution. A reduction of ≥50% in the HRQL score was defined as significant symptomatic relief. Recurrence was defined clinically by symptoms returning or by characteristic endoscopic and/or radiologic abnormalities.
Statistical analysis
Data were recorded and analyzed using SPSS software (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation. Interobserver and intraobserver agreement for HSA measurements were assessed using the intraclass correlation coefficient (ICC). Correlation between HSA and GERD-HRQL score (pre- and postoperative) was evaluated using Pearson’s coefficient. Statistical significance was defined as p < 0.05.
Results
Patient characteristics
A total of 25 patients with HH and GERD were included in this study. The mean age of the patients was 57.8 ± 12.3 years, with a range from 34 to 75 years. Of the 25 patients, 15 (60%) were female, and 10 (40%) were male. The mean body mass index (BMI) was 28.5 ± 3.7 kg/m².
Hiatal surface area (HSA) measurements
Using the new intraoperative imaging method with ImageJ software, the mean HSA of the hiatal defect was calculated to be 5.4 ± 1.8 cm², with individual measurements ranging from 2.8 to 9.2 cm². Table 1 summarizes the HSA measurements and provides additional demographic and clinical data.
The preoperative GERD-HRQL score averaged 27.7 ± 5.6, indicating moderate to severe symptoms burden. At 12-month follow-up, the postoperative GERD-HRQL score was 11.5 ± 4.9, reflecting significant symptomatic improvement (p <0.001). The proportion of patients achieving a ≥50% reduction in HRQL score was 80% (n=20).
Table 1. Patient Demographics, HSA Measurements, and GERD-HRQL Scores (n = 25) | ||
Variable | Mean ± SD | Range |
Age (years) | 57.8 ± 12.3 | 34 – 75 |
BMI (kg/m²) | 28.5 ± 3.7 | 24.1 – 34.3 |
HSA (cm²) | 5.4 ± 1.8 | 2.8 – 9.2 |
Preoperative GERD-HRQL Score | 27.7 ± 5.6 | 10 – 30 |
Postoperative GERD-HRQL Score | 11.5 ± 4.9 | 6-13 |
Note: Data are presented as mean ± standard deviation (SD) and range. Abbreviations: HSA – hiatal surface area; GERD-HRQL – Gastroesophageal Reflux Disease Health-Related Quality of Life; BMI – body mass index.HSA – Hiatal surface aria | ||
Interobserver and intraobserver reliability
Two independent reviewers analyzed each patient’s images to assess reliability. The interobserver intraclass correlation coefficient (ICC) was 0.92 (95% CI: 0.86–0.97), indicating high reliability between reviewers. The intraobserver ICC for repeat measurements was 0.94 (95% CI: 0.89–0.98) demonstrated in Table 2, confirming excellent measurement consistency.
Table 2. Interobserver and intraobserver reliability metrics | ||
Reliability metric | ICC | 95% Confidence interval |
Interobserver ICC | 0.92 | 0.86 – 0.97 |
Intraobserver ICC | 0.94 | 0.89 – 0.98 |
Note: Data are expressed as intraclass correlation coefficients (ICC) with corresponding 95% confidence intervals. Measurements were performed independently by two observers using the same digital image analysis protocol.Abbreviations: ICC – intraclass correlation coefficient. | ||
Correlation between HSA and clinical outcomes
The HSA measurements were analyzed for potential correlations with preoperative symptoms, clinical outcomes, including postoperative symptom resolution and hernia recurrence at a 12-month follow-up (Figure 2). A strong positive correlation was identified between preoperative GERD-HRQL score and measured HSA (r = 0.69), suggesting that patients with larger hiatal defects experienced more severe symptoms (Table 3).
 |
Fig. 2 Correlation between HSA and Preoperative GERD-HRQL Note: The scatter plot illustrates a positive linear relationship between HSA and symptom severity, as measured by the preoperative GERD-HRQL score. Each dot represents one patient. Abbreviations: HSA – hiatal surface area; GERD-HRQL – Gastroesophageal Reflux Disease Health-Related Quality of Life. |
Furthermore, a strong correlation was observed between HSA and postoperative symptoms improvement (r = 0.74), indicating the relevance of anatomical defect quantification in predicting surgical outcomes.
Table 3. HSA correlation analysis | |
Variable pair | Correlation coefficient (r) |
HSA vs preoperative GERD-HRQL | 0.69 |
HSA vs symptoms improvement (%) | 0.74 |
HSA >6 cm² vs recurrence | Strong association |
Note: Data include Pearson correlation coefficients (r) for continuous variables and descriptive association for binary outcomes. “Strong association” indicates a statistically significant relationship observed in all cases with HSA >6 cm².Abbreviations: HSA – hiatal surface area; GERD-HRQL – Gastroesophageal Reflux Disease Health-Related Quality of Life. | |
Patients with a larger HSA (≥6 cm²) exhibited a higher recurrence rate (20%) compared to those with a smaller HSA (<6 cm²), who had a recurrence rate of 6.6%. Table 4 provides a summary of postoperative outcomes in relation to HSA size.
Table 4. Postoperative outcomes based on HSA measurements | ||||
HSA Group | No. of Patients | Mean HSA (cm²) | Recurrence Rate (%) | Symptom Resolution (%) |
HSA <6 cm² | 15 | 4.2 ± 0.7 | 6.6 | 93.3 |
HSA ≥6 cm² | 10 | 7.3 ± 1.1 | 20 | 80 |
Overall | 25 | 5.4 ± 1.8 | 12 | 88 |
Note: Data are presented as means ± standard deviations and percentages. Recurrence was defined as radiologically or endoscopically confirmed reappearance of hiatal hernia at 12-month follow-up. Symptom resolution was defined as ≥50% improvement in GERD-HRQL scores compared to baseline. Abbreviations: HSA – hiatal surface area; GERD-HRQL – Gastroesophageal Reflux Disease Health-Related Quality of Life. | ||||
A positive correlation (r = 0.58, p < 0.05) was observed between HSA size and postoperative symptom severity, with larger defects being associated with higher postoperative symptom scores. Additionally, a higher BMI was weakly associated with an increased HSA size (r = 0.34, p = 0.07), though this was not statistically significant in this sample.
Discussion
Surgical treatment of HH and GERD remains challenging due to technical complexity, anatomical variability, including esophageal hiatus size, and associated risk of recurrence. Thus, the accurate measurement of the diaphragmatic hiatal surface area (HSA) is a decisive factor in selecting a reliable and safe modality for hiatus repair, i.e. simple suturing or mesh reinforcement. Traditional surgical methods have often relied on attempts of real measurement or subjective intraoperative assessments, which can lead to variability in outcomes. Granderath et al. [6] have been at the forefront of addressing this issue, proposing a standardized method for calculating the HSA using geometric principles applied intraoperatively. Their studies have shown that tailoring the crural closure based on the calculated HSA significantly reduces the risk of postoperative complications, such as dysphagia and recurrent herniation. In a study involving 55 patients who underwent LF, Granderath and colleagues reported a recurrence rate of less than 5% when the HSA was used to guide surgical decisions.
The limitations of intraoperative measurements, which can be influenced by factors such as patient positioning and the extent of surgical dissection, have prompted the exploration of more objective and reproducible methods. Moten et al. [7] developed a novel technique using multi-detector computed tomography (MDCT) combined with multi-planar reconstruction (MPR) to measure the HSA in vivo. This method offers a significant advancement over traditional techniques by allowing for a non-invasive, preoperative assessment of the hiatus. In their study, which included 30 patients scheduled for HH repair, Moten and colleagues demonstrated a strong correlation between the HSA measurements obtained via MDCT-MPR and those obtained intraoperatively (Pearson correlation coefficient = 0.83, p<0.001). The study also highlighted the high reproducibility of the MDCT-MPR technique, with intra-class correlation coefficients for intra- and inter-observer agreement both exceeding 0.97 (p <0.001), indicating excellent consistency.
Further reinforcing the importance of accurate HSA measurement, Koch et al. [8] explored the relationship between the size of the esophageal hiatus and the outcomes of surgical repairs. Their research, involving a cohort of patients undergoing laparoscopic fundoplication, found that patients with larger hiatal defects (HSA >8 cm²) were more likely to experience postoperative complications, including reherniation and persistent reflux symptoms, compared to those with smaller defects. Specifically, they reported a reherniation rate of approximately 15% in patients with HSA >8 cm², compared to just 3% in those with HSA ≤4 cm². This study underscores the need for precise preoperative assessment of the hiatal defect to tailor the surgical approach, particularly in determining whether to use mesh reinforcement during the repair. The role of advanced imaging techniques in enhancing surgical outcomes has also been highlighted by Ouyang et al. [7], who validated the use of MDCT-MPR for preoperative planning and postoperative assessment. Their findings suggest that MDCT-MPR not only provides accurate measurements of the HSA but also aids in identifying anatomical variations that could impact surgical decision-making, such as the presence of large hernias that might require more complex repairs. The incorporation of such imaging techniques into clinical practice represents a paradigm shift, moving away from subjective assessments to more objective, data-driven approaches that can improve patient outcomes.
The integration of these advanced methodologies into the surgical workflow is particularly crucial in the context of an aging population, where the incidence of HHs is expected to increase. With the prevalence of GERD also on the rise, estimated to affect up to 20% of the adult population in Western countries, the need for effective and durable surgical solutions is more pressing than ever. The adoption of standardized measurement techniques, such as those proposed by Granderath and validated by Moten and Ouyang [6, 7], is likely to play a key role in addressing this challenge, providing surgeons with the tools they need to deliver optimal care.
In our study, we proposed a novel intraoperative method for measuring the HSA based on calibrated digital photography and analysis with freely available software. The results obtained confirm that this technique is simple, reliable, and correlates strongly with the clinical severity of gastroesophageal reflux symptoms, as well as with the recurrence rate observed at 12 months postoperatively. A major strength of this method lies in its ability to overcome limitations of traditional intraoperative assessment, which often relies on subjective visual estimation or linear crural measurements. By introducing a fixed-size benchmark and analyzing the captured image through digital software, the surface area can be determined with high precision, regardless of the surgeon's experience or the degree of laparoscopic distortion. This objectivity adds reproducibility, which is critical when planning the extent of cruroplasty or the need for mesh reinforcement.
Furthermore, our findings showed a strong correlation between preoperative HSA and GERD-HRQL scores, reinforcing the anatomical-functional relationship between the size of the diaphragmatic defect and the severity of reflux symptoms. Larger defects appear to facilitate more pronounced disruption of the antireflux barrier, leading to increased symptom burden. From a therapeutic perspective, this observation supports the need for individualized surgical planning, particularly in high-HSA patients.
The recurrence rate of 12% observed at 12 months is consistent with previously reported data. Importantly, all patients with recurrence had an HSA greater than 6 cm². This suggests a potential threshold above which standard suture cruroplasty may be insufficient, regardless of technique and suture material. Stratification of patients based on HSA could, therefore, be used intraoperatively to decide on additional interventions such as mesh hiatoplasty or anterior crural buttressing. While controversy persists regarding mesh use, particularly due to complications like erosion or fibrosis, a risk-based approach guided by anatomical quantification could lead to better outcomes and personalized therapy.
Compared to imaging-based techniques (e.g., CT volumetry, EUS, or intraoperative 3D scanning), our approach is markedly more accessible and inexpensive, not requiring specialized equipment or extended training. The only requisites are a sterile scale reference, a digital camera (standard laparoscopic systems suffice), and access to basic image processing software. Its simplicity makes it suitable for both tertiary centers and lower-resource surgical settings.
The reproducibility of the method was confirmed by strong inter- and intra-observer reliability scores. The protocol’s minimal learning curve also allows it to be implemented across surgical teams with varying levels of experience, facilitating standardization in clinical practice and possibly in future multicentric research.
Nevertheless, several limitations must be acknowledged. First, although images were standardized as much as possible, subtle differences in camera angle or distance may still introduce minor variation in surface area estimation. Second, the study used GERD-HRQL score as a subjective symptom marker; objective measures such as 24-hour pH monitoring or manometry were not systematically incorporated. Lastly, follow-up was limited to 12 months, and long-term recurrence data remain to be assessed.
Conclusions
In conclusion, the proposed measurement technique offers a clinically useful, practical, and reproducible solution for quantifying the hiatal defect. Its potential impact includes improved intraoperative decision-making, more personalized surgical techniques, and better prediction of recurrence risk. However, patients with a HSA over 6 cm2 exhibited a statistically significant higher recurrence rate compared to those with a smaller HSA (20% vs 6.6%, r = 0.58). Future research may focus on refining calibration protocols, integrating this method with other intraoperative tools, and validating it in prospective multicenter trials.
Competing interests
None declared.
Authors’ contributions
SC and VG interpreted the data and performed the analytical part of the work, SC drafted the first manuscript; VI and EG conceptualized the project, designed the research and revised the manuscript critically.
Ethics approval
The research project was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Minutes no. 84, 20.06.2017).
Patient consent
Obtained.
Acknowledgements and funding
No external funding.
Declaration of generative AI and AI-assisted technologies in the writing process
The authors (SC) used OpenAI’s ChatGPT in order to assist with reference formatting in Vancouver style and language refinement. After using this tool, the authors (EG, VI and VG) thoroughly reviewed and edited all content and take full responsibility for the scientific accuracy, originality, and integrity of the publication.
Provenance and peer review
Not commissioned, externally peer reviewed.
Authors’ ORCID IDs
Serghei Cumpătă – https://orcid.org/0000-0003-3472-6152
Vasile Guzun – https://orcid.org/0009-0001-1545-3470
Vladimir Iacub – https://orcid.org/0000-0002-1865-0787
Evghenii Guțu – https://orcid.org/0000-0003-4590-4735
References
El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2014;63(6):871-80. doi: 10.1136/gutjnl-2012-304269.
Schlottmann F, Herbella FA, Allaix ME, Rebecchi F, Patti MG. Surgical treatment of gastroesophageal reflux disease. World J Surg. 2017;41(7):1685-1690. doi: 10.1007/s00268-017-3955-1.
Robinson B, Dunst CM, Cassera MA, Reavis KM, Sharata A, Swanstrom LL. 20 years later: laparoscopic fundoplication durability. Surg Endosc. 2015;29(9):2520-4. doi: 10.1007/s00464-014-4012-x.
Dallemagne B, Arenas Sanchez M, Francart D, et al. Long-term results after laparoscopic reoperation for failed antireflux procedures. Br J Surg. 2011;98(11):1581-7. doi: 10.1002/bjs.7590.
Turkcapar A, Kepenekci I, Mahmoud H, et al. Laparoscopic fundoplication with prosthetic hiatal closure. World J Surg. 2007;31(11):2169-76. doi: 10.1007/s00268-007-9066-7.
Granderath FA, Schweiger UM, Pointner R. Laparoscopic antireflux surgery: tailoring the hiatal closure to the size of hiatal surface area. Surg Endosc. 2007;21(4):542-8. doi: 10.1007/s00464-006-9041-7.
Moten AS, Ouyang W, Hava S, Zhao H, Caroline D, Abbas A. In vivo measurement of esophageal hiatus surface area using MDCT: description of the methodology and clinical validation. Abdom Radiol (NY). 2020 Sep;45(9):2656-2662. doi: 10.1007/s00261-019-02279-7.
Koch OO, Asche KU, Berger J, Weber E, Granderath FA. Influence of the esophageal hiatus size on the rate of reherniation after laparoscopic fundoplication and refundopilication with mesh hiatoplasty. Surg Endosc. 2013;25(4):1024-30. doi: 10.1007/s00464-010-1308-3.