
Introduction
Chronic kidney disease (CKD) is a prevalent global health problem, affecting an estimated 13.4% of the global population (over 800 million people worldwide) and contributing significantly to mortality [1]. CKD is often termed a “silent epidemic” due to its insidious progression, high cardiovascular mortality, and substantial public health burden [1, 2]. COVID-19, caused by SARS-CoV-2, has emerged as a multisystem disease; although initially recognized as a respiratory illness, it is now known to cause widespread organ damage, including acute kidney injury (AKI). The kidney’s high expression of ACE2 (the SARS-CoV-2 entry receptor) makes it particularly vulnerable to COVID-19-associated injury. Clinical reports indicate a high frequency of AKI in severe COVID-19, along with direct viral effects on renal tubular and glomerular cells leading to structural damage.
There is a bidirectional, syndemic interaction between CKD and COVID-19. CKD patients, especially those with advanced stages, are at a markedly increased risk for severe COVID-19 outcomes due to chronic uremic immunosuppression, systemic inflammation, and comorbidities. Indeed, CKD has been identified as an independent risk factor for COVID-19 severity and mortality. Conversely, surviving a COVID-19 infection may adversely affect kidney health. SARS-CoV-2 infection can trigger AKI and may accelerate the trajectory of chronic kidney damage, even in individuals without prior renal disease. An episode of COVID-19-related AKI can become a “reset point”, leading to faster-than-expected CKD progression or transition to end-stage renal disease (ESRD) than expected from the prior course. In practical terms, a CKD patient who contracts COVID-19 might reach advanced CKD stages or dialysis faster than a similar patient who never had COVID.
Emerging evidence suggests that COVID-19 survivors can experience persistent subclinical renal impairment. One cohort study found that at 6 months post-COVID, 35% of patients had a reduced estimated glomerular filtration rate (eGFR <90 mL/min/1.73 m²) despite normal kidney function during the acute infection. Notably, 13% of patients with no AKI in the hospital still showed a significant decline in eGFR by 6 months. These findings imply that even relatively mild COVID-19 can have lasting renal sequelae. Longer-term studies indicate a substantial proportion of COVID-19 survivors have persistent abnormalities such as reduced eGFR, proteinuria, or hematuria at 6–12 months. COVID-19 has thus been recognized as an emergent risk factor for kidney disease, adding to traditional factors like diabetes and hypertension.
Despite these concerns, data on the impact of COVID-19 on the progression of pre-existing CKD are limited, particularly in Eastern European populations with a high CKD burden. Most studies have been retrospective and have focused on AKI incidence or short-term outcomes. There is a need for a prospective analysis of how COVID-19 may influence the CKD trajectory and which patients are most vulnerable to renal function decline after infection. We hypothesized that CKD patients who recovered from COVID-19 would experience a faster decline in renal function compared to CKD patients with no COVID history, and that markers of inflammation or tissue injury might predict this decline.
This study aimed to evaluate the long-term impact of COVID-19 on CKD progression and to identify clinical and biological predictors of adverse renal outcomes. Specifically, we compared a cohort of CKD patients with prior COVID-19 to a matched cohort of CKD patients without COVID-19, in terms of renal function decline, the incidence of CKD stage progression or dialysis, and other health outcomes. We also explored associations between baseline inflammatory markers (CRP, ferritin, LDH), hematologic parameters, and progression risk. By providing prospective data in a previously under-studied population, our study seeks to inform post-COVID care strategies for CKD patients and guide early interventions to improve their prognosis.
Materials and methods
This prospective observational cohort study enrolled 280 adult patients with chronic kidney disease not on dialysis. Patients were recruited from nephrology clinics and inpatient services at Timofei Moșneaga Republican Clinical Hospital (Chișinău, Moldova) between 2023 and 2024. Inclusion criteria were: age 18–70 years, confirmed CKD (pre-dialysis, defined by evidence of chronic renal disease and/or eGFR <60 mL/min/1.73 m² for ≥3 months), and written informed consent. The study was conducted in accordance with the Declaration of Helsinki and was approved by the institutional ethics committee (favorable opinion of the Research Ethics Committee of Nicolae Testemitanu State University of Medicine and Pharmacy, no. 6 of 18.05.2023). All participants provided informed consent.
We excluded individuals receiving renal replacement therapy (dialysis) or with a history of kidney transplant, as well as those with active malignancy or tuberculosis, or who declined participation. After applying criteria, the study population consisted of 280 eligible CKD patients. These were divided into two equal groups based on COVID-19 exposure:
Post-COVID group (exposed cohort): 140 CKD patients who had recovered from a documented COVID-19 infection prior to or during the study period. COVID-19 was confirmed by clinical diagnosis and/or positive laboratory tests (e.g., PCR). Only patients evaluated after clinical recovery from acute COVID-19 were included, with a median of ~3 months from infection to enrollment. We recorded the date and severity of the COVID-19 episode for each (mild, moderate, or severe; whether hospitalization or ICU care was needed).
CKD control group (unexposed cohort): 140 CKD patients with no history of COVID-19 (by patient report and available testing). These patients served as the comparison group to isolate the effect of COVID-19 on CKD evolution.
The two groups were frequency-matched on key characteristics. They were similar in age and sex distribution and had comparable distributions of CKD etiology (diabetic nephropathy, hypertensive nephrosclerosis, glomerulonephritis, etc.). Both groups predominantly comprised patients in middle to advanced CKD stages (G2–G5 ND), with no significant differences in baseline CKD stage distribution (median stage 3 in each). Comorbid conditions such as diabetes mellitus (overall ~26%) and hypertension (~82%) were common and similarly distributed, aside from a non-significant trend toward higher diabetes prevalence in the post-COVID group (31% vs 21%, p ≈ 0.06). All patients continued to receive standard CKD care (e.g., blood pressure control, renin–angiotensin system blockers, anemia management) as per clinical guidelines.
At baseline (study entry), all patients underwent a comprehensive evaluation including clinical history, physical examination, laboratory tests, and questionnaire administration. Baseline evaluations for the post-COVID group were performed after recovery from acute infection (no patient had active COVID-19 at time of assessment).
Baseline characteristics: mean age 58.7 ± 12.4 years (post-COVID) and 56.9 ± 13.1 (control); males 55.0% vs 50.7%; diabetes prevalence 31% vs 21% (p ≈ 0.06); hypertension ~82% in both groups. Median CKD stage was 3 in both cohorts. All patients received standard nephrology care.
Baseline evaluations included clinical history, physical exam, SF-36 questionnaire, and laboratory tests.
Renal function: Serum creatinine, urea, eGFR (CKD-EPI 2021), urinalysis, proteinuria.
Hematology: Hemoglobin, leukocyte and platelet counts.
Inflammation/tissue injury: C-reactive protein (CRP), ferritin, lactate dehydrogenase (LDH).
Metabolic labs: Electrolytes, uric acid, liver enzymes, D-dimer, total protein, and albumin.
Quality of life: SF-36 assessed 8 domains (scored 0-100), including vitality and physical function.
Patients were followed for 12 months. Outcomes included CKD progression (≥30% eGFR decline or dialysis), changes in eGFR, dialysis initiation, and mortality.
Statistical analysis. We used SPSS v25 and R v4.1. Continuous variables were compared using t-tests or Mann-Whitney U; categorical variables via χ2 tests. Correlations (Pearson or Spearman) evaluated associations between biomarkers and eGFR change. Multivariable logistic regression identified independent predictors of CKD progression. ROC curves assessed predictive value (AUC). Statistical significance was set at p < 0.05.
Results
A total of 280 CKD patients were analyzed (140 post-COVID and 140 controls). Baseline demographic and clinical characteristics are shown in Table 1. The two groups were comparable in age (58.7 vs. 56.9 years), sex distribution (55.0% vs. 50.7% male), and comorbidity burden, including hypertension (>80%) and diabetes (~26%, with a non-significant trend toward higher prevalence in the post-COVID group). Baseline BMI and blood pressure were similar.
Renal function at study entry did not differ significantly: mean serum creatinine (2.23 vs. 2.38 mg/dL) and eGFR (57 vs. 65 mL/min/1.73 m², p = 0.19) were comparable. CKD stages were evenly distributed, with a median stage of 3 in both cohorts. Rates of proteinuria, microscopic hematuria, and leukocyturia were also similar.
Inflammatory markers showed wide interindividual variation, characteristic of CKD. Although mean CRP was numerically higher in the post-COVID group, median values were nearly identical (1.8 vs. 1.7 mg/L), and the difference was not statistically significant. Ferritin levels, ESR, and other inflammatory parameters likewise showed no meaningful group differences. Hemoglobin values averaged 11.4–11.5 g/dL across groups, consistent with CKD-related anemia.
LDH levels were mildly elevated in both groups, with a non-significant trend toward higher levels in controls (195 vs. 183 U/L). Albumin was modestly reduced (~3.5 g/dL) in both cohorts.
SF-36 results indicated similar physical functioning between the groups, while post-COVID patients reported significantly lower vitality (greater fatigue) and higher social functioning scores.
Overall, baseline clinical and laboratory characteristics were well balanced between groups, ensuring comparable starting conditions for assessing subsequent renal outcomes.
Table 1. Baseline characteristics of CKD patients with and without prior COVID-19 | |||
Characteristic | Post-COVID CKD (n = 140) | CKD Control (n = 140) | p-value |
Age, years | 58.7 ± 12.4 | 56.9 ± 13.1 | 0.32 |
Male sex, % | 55.0% | 50.7% | 0.48 |
Body mass index, kg/m2 | 28.3 ± 5.7 | 27.8 ± 5.4 | 0.45 |
Diabetes mellitus, % | 31.4% | 21.4% | 0.06 |
Hypertension, % | 84.3% | 80.0% | 0.34 |
Coronary artery disease, % | 18.6% | 16.4% | 0.62 |
Renal function | |||
Serum creatinine, mg/dL | 2.23 ± 1.84 | 2.38 ± 1.73 | 0.53 |
eGFR, mL/min/1.73 m2 | 56.9 ± 33.4 | 64.7 ± 62.8 | 0.19 |
CKD stage (median) | 3 (G3b predominant) | 3 (G3a-G4 predominant) | 0.59 |
Proteinuria ≥0.3 g/day, % | 58.6% | 51.4% | 0.21 |
Hematuria (micro) % | 20.0% | 22.9% | 0.58 |
Inflammation & labs | |||
C-reactive protein, mg/L | 13.96 ± 42.5 (median 1.8) | 4.25 ± 8.25 (median 1.7) | 0.51¹ |
Ferritin, µg/L | 116 ± 141 | 139 ± 180 | 0.23 |
Lactate dehydrogenase, U/L | 183 ± 51 | 195 ± 66 | 0.10 |
Hemoglobin, g/dL | 11.4 ± 1.8 | 11.5 ± 1.9 | 0.74 |
White blood cells, ×109/L | 7.9 ± 2.5 | 7.6 ± 2.2 | 0.30 |
Platelet count, ×109/L | 262 ± 78 | 254 ± 69 | 0.55 |
Albumin, g/dL | 3.50 ± 0.42 | 3.55 ± 0.45 | 0.68 |
SF-36 Physical Function1 | 47.4 ± 25.0 | 40.4 ± 38.0 | 0.07 |
SF-36 Vitality (Energy)1 | 44.1 ± 16.9 | 56.5 ± 19.0 | <0.001 |
SF-36 Social Function1 | 59.0 ± 22.0 | 43.8 ± 25.6 | <0.001 |
Note: 1CRP values were highly skewed; medians are given in parentheses. SF-36 domain scores are scaled 0–100 (higher = better function). Abbreviations: eGFR = estimated glomerular filtration rate (CKD-EPI formula); CKD stage per KDIGO G categories; SF-36 = 36-item Short Form health survey. Values expressed as mean ± SD, median [IQR], or % | |||
Quality of life (SF-36) results. All patients completed the SF-36 at baseline. Overall quality of life was reduced in both groups, as expected in CKD. As shown in Table 1, Physical Functioning was slightly higher in the post-COVID group (47.4 vs. 40.4), though the difference was not statistically significant. Most physical and emotional role limitations were similar between the groups.
Two domains showed significant differences. Vitality scores were lower in the post-COVID group (44.1 vs. 56.5, p < 0.001), indicating more pronounced fatigue, which likely reflected persistent post-COVID symptoms. In contrast, Social Functioning was higher among post-COVID patients (59.0 vs. 43.8, p < 0.001), suggesting better perceived social engagement. A possible explanation is that recovery from COVID-19 may have reinforced social connectedness or coping behaviors.
Mental Health scores (~59), Bodily Pain (~38), and General Health perception (~40) were comparable. Both groups rated their overall health as relatively poor, consistent with the CKD burden.
In summary, post-COVID CKD patients reported greater fatigue but better social functioning compared to controls, highlighting the complex and multidimensional impact of COVID-19 on patient-reported outcomes.
Follow-up and renal outcomes. All patients were followed for a median of 12 months (minimum 12, maximum 15 months). During this period, no patients were lost to follow-up. We monitored for changes in renal function and the occurrence of our defined outcome of CKD progression. The results are presented in Table 2 and illustrated in Figure 1.
By the end of follow-up, the post-COVID cohort experienced a faster decline in kidney function compared to controls. The mean change in eGFR from baseline was –3.1 ± 6.5 mL/min/1.73 m² in the post-COVID group versus –1.2 ± 5.8 mL/min/1.73 m² in controls (a more than twofold greater decline; p = 0.01). Specifically, 62% of post-COVID patients had some drop in eGFR (any decline >0), compared to 45% of controls (where many control patients remained stable or even had slight improvements due to interventions or variability). Figure 1 illustrates the proportion of patients meeting our progression criteria in each group: 28% of the post-COVID group vs 15% of controls reached the composite endpoint of ≥30% eGFR decline or need for dialysis within one year (Figure 1, p = 0.002).
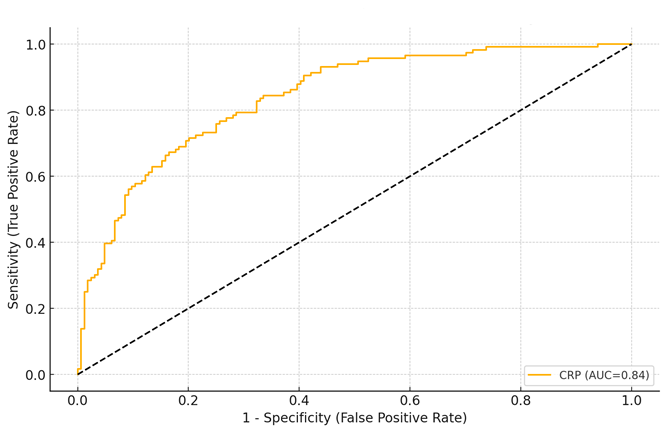 |
Fig. 1 CKD progression rates at 12 months in post-COVID vs control groups. Note: Bar heights represent the percentage of patients who progressed (≥30% eGFR decline or dialysis start). A significantly higher proportion of the post-COVID CKD group progressed (28.0%) compared to the CKD control group (15.0%, p = 0.002). |
In absolute terms, 39 out of 140 post-COVID patients vs. 18 out of 140 controls had a ≥30% decline in eGFR over 12 months (p = 0.001). Moreover, renal failure requiring dialysis occurred more frequently in the post-COVID group: 10 patients (7.1%) initiated chronic dialysis during follow-up compared to 2 patients (1.4%) in the control group (p = 0.03). The dialysis cases in the post-COVID group predominantly had severe baseline CKD (eGFR <20 mL/min/1.73 m2) and subsequently experienced COVID-19-associated AKI that never fully recovered, whereas the two control cases were due to the natural progression of CKD. Additionally, three post-COVID patients (2.1%) versus one control (0.7%) experienced rapid progression to an eGFR <15 mL/min/1.73 m2 without initiating dialysis by 12 months (being managed conservatively or awaiting access creation). When combining dialysis initiation with these late-stage cases, the difference remained significant. No patient in either cohort received a transplant during the study.
We also tracked other outcomes. All-cause mortality during follow-up was low, reflecting the relatively short observation period: 4 deaths occurred in the post-COVID group (2.9%) versus 3 in controls (2.1%, p = 0.70). Causes of death were cardiovascular in most cases (myocardial infarction or stroke), with one COVID-group patient dying of sepsis and one control of unknown sudden death. Although mortality was slightly higher in the post-COVID group, the difference was not statistically significant. Notably, two of the post-COVID deaths occurred in patients who had progressed to dialysis; this aligns with literature showing worse outcomes in CKD patients post-COVID, but our study size was not powered for mortality analysis.
Regarding quality of life over time, we did not perform a second SF-36 assessment at 12 months for all patients, therefore longitudinal QoL changes are not reported quantitatively. However, during clinical visits many post-COVID patients subjectively reported improvement in fatigue over time. By contrast, objective renal outcomes clearly diverged between the groups as described.
Table 2. Renal function outcomes at 12-month follow-up | |||
Outcome (12 months) | Post-COVID CKD (n = 140) | CKD Control (n = 140) | p-value |
eGFR change from baseline (mL/min/1.73 m²) | –3.1 ± 6.5 | –1.2 ± 5.8 | 0.010 ** |
≥30% decline in eGFR, n (%) | 39 (27.9%) | 18 (12.9%) | 0.001 ** |
Initiation of dialysis, n (%) | 10 (7.1%) | 2 (1.4%) | 0.017 * |
Composite progression (either of above) | 42 (30.0%) | 20 (14.3%) | 0.001 ** |
All-cause mortality, n (%) | 4 (2.9%) | 3 (2.1%) | 0.70 |
Δ Serum creatinine, mg/dL (baseline→12 m) | +0.43 ± 1.10 | +0.15 ± 0.96 | 0.07 |
Δ CKD stage (median) | +0.5 | ±0 | – |
Note: statistical significance: p < 0.05 *, p < 0.01 **. Δ indicates change; a positive Δ creatinine means an increase (worsening). “Composite progression” denotes meeting the primary endpoint (≥30% eGFR drop or dialysis start). Median CKD stage change: post-COVID group median progressed by half a stage (e.g. many G3a→G3b), whereas median control remained the same stage. | |||
As seen in Table 2, CKD progression was significantly more common among those with prior COVID-19. The unadjusted odds ratio (OR) for CKD progression in the post-COVID group was approximately 2.5 (95% CI ~1.4–4.4) relative to controls. This finding supports our hypothesis that COVID-19 has a measurable adverse effect on the CKD trajectory. It is consistent with recently published retrospective data, which reported that CKD patients with COVID-19 had about 3.7-fold higher odds of rapid eGFR decline compared to those without COVID. Our prospective design strengthens the causal inference that COVID-19 may accelerate underlying kidney disease.
Factors associated with CKD progression. We next evaluated baseline predictors of CKD progression. In univariate analysis, progressors were more frequently from the post-COVID group (67%, p < 0.01) and had lower baseline eGFR (35 vs. 62 mL/min, p < 0.001), lower hemoglobin (10.8 vs. 11.7 g/dL, p = 0.004), and higher LDH (210 vs. 182 U/L, p = 0.01). CRP, ferritin, and other inflammatory markers did not differ between progressors and non-progressors, suggesting that post-recovery inflammation was not a major determinant of decline.
Correlation analysis showed that hemoglobin correlated inversely with eGFR decline (r = –0.25, p < 0.001), and LDH showed a weaker association (r = –0.14, p = 0.02). CRP and ferritin showed no meaningful correlations. ESR correlated moderately with decline (r≈–0.20, p < 0.01) and strongly with anemia, reflecting chronic inflammatory burden.
Multivariable logistic regression identified three independent predictors of CKD progression: prior COVID-19, lower hemoglobin, and higher LDH (Table 3). COVID-19 history remained a significant risk factor (aOR 2.28, p = 0.008). Each 1 g/dL decrease in hemoglobin increased progression risk by ~40% (aOR 1.38, p = 0.005), while LDH also predicted progression (aOR 1.20 per +50 U/L, p = 0.027). CRP, ferritin, diabetes, age, and baseline eGFR were not independent predictors.
These findings indicate that CKD patients with prior COVID-19, anemia, and elevated LDH are at a substantially higher risk for accelerated renal decline. Traditional risk factors such as diabetes showed no independent effect, likely because the impact of COVID-19 and anemia dominated short-term outcomes.
Table 3. Multivariate logistic regression for predictors of CKD progression (N = 280) | ||
Predictor | Adjusted OR (95% CI) | p-value |
Prior COVID-19 (yes vs no) | 2.28 (1.24–4.21) | 0.008 ** |
Hemoglobin (per –1 g/dL) | 1.38 (1.10–1.73) | 0.005 ** |
LDH (per +50 U/L) | 1.20 (1.02–1.42) | 0.027 * |
Baseline eGFR (per +5 mL/min) | 0.96 (0.89–1.04) | 0.30 |
Diabetes (yes vs no) | 1.32 (0.70–2.50) | 0.39 |
CRP (per +10 mg/L) | 1.05 (0.92–1.21) | 0.47 |
Ferritin (per +50 µg/L) | 0.98 (0.88–1.08) | 0.65 |
Age (per +10 years) | 1.11 (0.85–1.45) | 0.45 |
Sex (male vs female) | 0.89 (0.50–1.58) | 0.69 |
Note: Model χ² = 29.5, p < 0.001. OR = odds ratio; CI = confidence interval. OR >1 indicates higher odds of progression. Bold indicates p < 0.05. (Baseline eGFR and diabetes were not significant here, possibly due to collinearity and cohort matching). | ||
To illustrate the predictive value of the model, we plotted ROC curves. The baseline hemoglobin level alone yielded an AUC of 0.78 for predicting progression, suggesting fair discrimination. Adding COVID-19 status improved the AUC to ~0.81. A full model with COVID status + hemoglobin + LDH achieved an AUC of 0.85. In contrast, baseline CRP had minimal predictive power (AUC = 0.58, Figure 2), performing little better than chance. This reinforces that acute inflammatory markers measured after recovery are not useful prognostic indicators in this setting, whereas markers of chronic disease severity (anemia) and the exposure to COVID-19 are more critical.
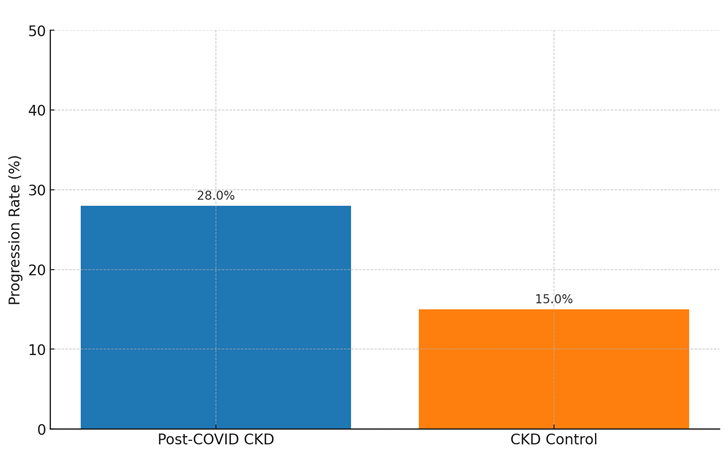 |
Fig. 2 ROC curve for baseline CRP level predicting CKD progression. Note: The curve (orange line) shows the trade-off between sensitivity and specificity for various CRP cut-offs. The area under the ROC curve (AUC) was 0.58, indicating poor discriminative ability of CRP alone for predicting progression in this cohort (no better than chance). The diagonal dashed line represents the line of no discrimination (AUC = 0.50). |
Notably, the finding that anemia is a strong predictor aligns with the idea that low hemoglobin signifies advanced CKD and systemic inflammation/malnutrition, which contribute to faster decline. Anemia can also worsen renal hypoxia, accelerating nephron loss. The importance of prior COVID-19 as an independent predictor, even when controlling for baseline CKD severity, suggests a direct effect of the infection on kidney disease progression. This could be mediated by residual damage (e.g., from AKI) and/or persistent inflammatory or immune dysregulation after the infection.
Post-hoc analysis: COVID-19 severity and renal outcomes. Within the post-COVID group, we conducted exploratory analyses to see if the severity of the acute COVID-19 episode was associated with the degree of CKD progression. Patients were stratified by their COVID-19 severity: 28 had mild (outpatient) cases, 82 had moderate cases (hospitalized with pneumonia but no ICU), and 30 had severe cases (required ICU or high-flow oxygen). We found a significant gradient: 50% of those with severe COVID progressed, compared to 30% with moderate and 14% with mild disease (χ² trend p = 0.002). Those with severe COVID had a mean eGFR decline of -5.8 mL/min, vs. -2.7 for moderate and –0.5 for mild (ANOVA p = 0.01). This aligns with external data from large cohorts: for example, a US Veterans study showed that patients who required ICU for COVID had an additional 5-7 mL/min/year loss of eGFR beyond normal decline, while even non-hospitalized COVID patients had an extra ~3 mL/min/year decline. In our cohort, severe COVID often coincided with AKI; among post-COVID patients who had COVID-related AKI (n = 22), the progression rate was 55% versus 24% in those without AKI (p = 0.003). These observations, although from a subgroup, suggest that the acute insult severity correlates with long-term CKD impact – a finding echoed by other studies.
It is important to note that even some patients with mild COVID (no initial AKI) experienced CKD progression, consistent with reports that even mild COVID-19 can leave residual renal sequelae in susceptible individuals. We did not find a significant correlation between time since COVID infection and progression in this one-year window (most infections were within 6-18 months prior to baseline), though longer follow-up is needed to see if these effects attenuate or persist.
Discussion
This prospective study demonstrates that CKD patients with prior COVID-19 experienced a significantly faster renal decline than CKD patients without COVID-19, with nearly one-third meeting the criteria for progression within one year. Prior COVID-19 remained an independent predictor of progression even after adjustment for baseline renal function, supporting the hypothesis that SARS-CoV-2 may accelerate CKD deterioration [2]. These results align with earlier research indicating higher risks of rapid eGFR decline among CKD patients who contract COVID-19 [2, 3] and with long-term cohort data showing increased adverse renal outcomes in COVID-19 survivors [3].
A likely mechanism is COVID-19-related AKI, which can lead to irreversible nephron loss or maladaptive fibrosis. In our cohort, patients with previous AKI – especially severe cases requiring ICU care – had the highest progression rates [4], consistent with evidence that COVID-19-associated AKI increases the risk of sustained CKD worsening. SARS-CoV-2 may injure renal tubular and endothelial cells directly, and autopsy studies have confirmed viral particles and inflammatory injury in kidney tissue [4, 5]. Systemic inflammation, coagulopathy, and hemodynamic instability during the acute infection may further accelerate CKD progression [5, 6].
Inflammation is a known driver of CKD decline [5, 6], yet traditional inflammatory markers (CRP, ferritin) did not predict outcomes in our cohort, likely because acute inflammation had resolved by baseline [6, 7]. ESR, however, correlated with decline, suggesting that the chronic inflammatory burden remains a relevant pathway [6, 7]. LDH, another marker linked to acute and long-COVID states, independently predicted progression, possibly indicating persistent subclinical organ injury [6, 7].
Anemia emerged as one of the strongest predictors of progression, consistent with prior studies [8]. Low hemoglobin both reflects the disease severity and contributes to renal hypoxia, creating a cycle of worsening kidney injury. These findings underscore the importance of optimal anemia management, particularly in post-COVID CKD patients [8, 9].
Quality-of-life data showed greater fatigue among post-COVID patients, consistent with post-COVID syndrome [10, 11], which may indirectly influence disease trajectory by limiting functional capacity. Higher social functioning scores may reflect behavioral or psychological changes following recovery from severe illness [11].
Clinically, CKD patients with a history of COVID-19 – especially severe disease – should receive intensified renal monitoring. More frequent assessment of eGFR and proteinuria may allow earlier detection of decline and timely interventions [12, 13]. Kidney-protective strategies and optimization of comorbidity management may be particularly important in this group [12, 13]. SGLT2 inhibitors could be beneficial post-COVID, a hypothesis requiring further study [14]. Preventive measures, including vaccination, remain essential.
From a pathophysiological standpoint, our findings support the concept that COVID-19 acts as a “second hit,” accelerating CKD progression through persistent metabolic and inflammatory effects [15]. Reports of post-COVID glomerulopathies, although rare, reinforce the need for vigilance [16, 17].
The study’s limitations include its one-year follow-up, single-center design, and limited sample size for subgroup analyses. Despite these, strengths include complete follow-up, rigorous matching of cohorts, and detailed phenotyping [17, 18]. These results generate important hypotheses for future research, particularly regarding anemia correction and LDH-based risk stratification [19].
In conclusion, COVID-19 exposure should be recognized as a significant prognostic factor in CKD. Incorporating COVID-19 history into risk stratification and follow-up pathways may help prevent premature progression to ESRD [19, 20]. The interaction between COVID-19 and CKD illustrates how acute infectious diseases can substantially alter the course of chronic conditions, contributing to a broader syndemic burden.
Conclusions
This study demonstrates that prior COVID-19 infection is a significant accelerator of chronic kidney disease progression. CKD patients who recovered from COVID-19 showed nearly a twofold risk of major renal function decline within one year compared to those without COVID-19, even after adjusting for baseline renal status.
COVID-19 history, low hemoglobin, and elevated LDH were the strongest independent predictors of progression, highlighting the roles of persistent tissue injury and anemia in post-COVID renal vulnerability. Classical inflammatory markers such as CRP and ferritin were not predictive, suggesting that chronic – not acute – inflammation is more relevant for long-term renal decline.
Clinically, CKD patients with prior COVID-19 – especially those with a history of severe disease or COVID-related AKI – require closer monitoring, more frequent assessment of eGFR and proteinuria, and early optimization of renoprotective therapy. Attention to anemia correction may be particularly important in this population.
Overall, COVID-19 should be considered a key prognostic factor in CKD management. Integrating COVID-19 history into risk stratification algorithms may help prevent premature progression to end-stage renal disease.
Competing interests
None declared.
Authors’ contribution
TR and LG conceived and designed the study. TR, ER, and CG collected clinical data. RE and CG performed statistical analysis. TR drafted the manuscript. LG and ER critically revised the manuscript. All authors approved the final version.
Informed consent for publication
Obtained.
Ethics approval and informed consent
The study involving human participants was reviewed and approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (favorable opinion no.6 of 18.05.2023). Patient consent was waived due to the retrospective nature of the study and use of de-identified data. All methods were carried out in accordance with relevant guidelines and regulations, and the study conforms to the principles of the Declaration of Helsinki.
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Authors’ ORCID IDs
Tatiana Răzlog – https://orcid.org/0009-0005-1277-2774
Eugeniu Russu – https://orcid.org/0000-0001-8957-8471
Costina Groza – https://orcid.org/0000-0002-6820-0522
Liliana Groppa – https://orcid.org/0000-0002-3097-6181
References
Coresh J, Byrd-Holt D, Astor BC, et al. Chronic kidney disease awareness, prevalence, and trends among U.S. adults, 1999 to 2000. J Am Soc Nephrol. 2005;16(1):180-188. doi: 10.1681/ASN.2004070539.
Couturier A, Ferlicot S, Chevalier K, et al. Indirect effects of severe acute respiratory syndrome coronavirus 2 on the kidney in coronavirus disease patients. Clin Kidney J. 2020;13(3):347-353. doi: 10.1093/ckj/sfaa088.
Del Vecchio, L, Balafa O, Dounousi E, et al. COVID-19 and cardiovascular disease in patients with chronic kidney disease. Nephrol Dial Transplant. 2024;39(2)177-189. https://doi.org/10.1093/ndt/gfad170.
Dellepiane S, Vaid A, Jaladanki SK, et al. Acute kidney injury in patients hospitalized with COVID-19 in New York City: temporal trends from march 2020 to april 2021. Kidney Med. 2021;3(5):877-879. doi: 10.1016/j.xkme.2021.06.008.
Farouk SS, Fiaccadori E, Cravedi P, Campbell KN. COVID-19 and the kidney: what we think we know so far and what we don't. J Nephrol. 2020;33(6):1213-1218. doi: 10.1007/s40620-020-00789-y.
Eligulashvili, A, Gordon M, Lee JS, et al. Long-term outcomes of hospitalized patients with SARS-CoV-2/COVID-19 with and without neurological involvement: 3-year follow-up assessment. PLoS Med. 2024;21(4):e1004263. https://doi.org/10.1371/journal.pmed.1004263.
Fisher, M, Neugarten J, Bellin E, et al. AKI in hospitalized patients with and without COVID-19: a comparison study. J Am Soc Nephrol. 2020;31(9):2145-2157. https://doi.org/10.1681/ASN.2020040509.
Flythe JE, Assimon MM, Tugman MJ, et al. Characteristics and outcomes of individuals with pre-existing kidney disease and COVID-19 admitted to intensive care units in the United States. Am J Kidney Dis. 2021;77(2):190-203.e1. doi: 10.1053/j.ajkd.2020.09.003.
Gok, M, Cetinkaya H, Kandemir T, et al. Chronic kidney disease predicts poor outcomes of COVID-19 patients. Int Urol Nephrol. 2021;53(9):1891-1898. https://doi.org/10.1007/s11255-020-02758-7.
Graham EL, Clark JR, Orban ZS, et al. Persistent neurologic symptoms and cognitive dysfunction in non-hospitalized Covid-19 “long haulers. Ann Clin Trans Neurol. 2021;8(5):1073-1085. doi: 10.1002/acn3.51350.
Groza C, Russu E, Rotaru L, Razlog T, Calancea V, Groppa L. Evaluarea influenţei psihosociale asupra calităţii vieţii pacienţilor cu boala cronică de rinichi = Assessing the psychosocial influence on the quality of life of patients with chronic kidney disease. Mold J Health Sci. 2024;11(2 Suppl 1):58. Romanian, English.
Răzlog T, Russu E, Ceban E, Groza C, Alexa Z, Groppa L. Factorii de progresie ai bolii cronice de rinichi la pacienții cu COVID-19 = Factors of progression of chronic kidney disease in COVID-19 patients. Mold J Health Sci. 2024;11(2 Suppl 1):59. Romanian, English.
Răzlog T, Russu E, Alexa Z, Ceban E, Groza C, Groppa L. Manifestations of kidney involvement in COVID-19 patients and progression to chronic kidney disease. Mold J Health Sci. 2024;11(1):11-18. https://doi.org/10.52645/MJHS.2024.1.02
Khatri, M, Charytan DM, Parnia S, et al. Outcomes among hospitalized chronic kidney disease patients with COVID
19. Kidney 360. 2021;2(7):1107-1114. https://doi.org/10.34067/KID.0006852020.
Gupta S, Hayek SS, Wang W, et al. Factors associated with death in critically ill patients with coronavirus disease 2019 in the US. JAMA Int Med. 2020;180(11):1436-1447. doi: 10.1001/jamainternmed.2020.3596.
Henry BM, Lippi G. Chronic kidney disease is associated with severe coronavirus disease 2019 (COVID-19) infection. Int Urol Nephrol. 2020;52(6):1193-1194. doi: 10.1007/s11255-020-02451-9.
Huang C, Huang L, Wang Y, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2021;397(10270):220-232. doi: 10.1016/S0140-6736(20)32656-8.
Long JD, Strohbehn I, Sawtell R, Bhattacharyya R, Sise ME. COVID-19 survival and its impact on chronic kidney disease. Transl Res. 2022;241:70-82. https://doi.org/10.1016/j.trsl.2021.11.003.
Ng JH, Hirsch JS, Hazzan A, et al. Outcomes among patients hospitalized with COVID-19 and acute kidney injury. Am J Kidney Dis. 2021;77(2):204-215.e1. doi: 10.1053/j.ajkd.2020.09.002.
Valeri AM, Robbins-Juarez SY, Stevens JS, et al. Presentation and outcomes of patients with ESKD and COVID-19. J Am Soc Nephrol. 2020;31(7):1409-1415. doi: 10.1681/ASN.2020040470.