
Introduction
Stroke is one of the most critical medical emergencies and a major cause of mortality and disability both in the Republic of Moldova and globally. Early recognition and rapid intervention are key factors that can mean the difference between life and death, or between full recovery and permanent disability. In this context, the role of prehospital intervention is of paramount importance.
In a healthcare system undergoing modernization and alignment with international standards, the Republic of Moldova is increasingly prioritizing the initial stages of medical response. The implementation of standardized tools, such as checklists, has become essential in optimizing the performance of emergency response teams. These tools help standardize patient assessment, reduce response times, and ensure effective communication between prehospital services and specialized hospital units [1].
Checklists not only support swift decision-making in the field but also provide a clear and scientifically validated framework for applying diagnostic and treatment protocols tailored to local realities. Their systematic use can significantly improve the quality of prehospital care, reduce medical errors, and increase the chances of survival and recovery for stroke patients.
This article evaluates the effectiveness of using checklists in prehospital stroke interventions in the Republic of Moldova, based on an analysis of national statistical data and a systematic review of the scientific literature, including relevant examples from international experience.
Globally, various preventive strategies have been developed to combat acute neurological conditions, especially cerebrovascular diseases, which pose a significant burden on healthcare systems. These strategies reflect the efforts of countries and international organizations to reduce the incidence and impact of such conditions on public health.
The Republic of Moldova's commitment to reducing the incidence and impact of cerebrovascular diseases is reflected in governmental and intersectoral efforts to implement preventive measures and coordinated interventions. National and international strategies for the prevention of acute neurological pathologies emphasize the importance of a well-coordinated approach, adapted to each country’s specific context, focused on risk reduction and improved access to diagnosis and treatment.
Reviews indicate that prehospital protocols and stroke‑specific checklists (e.g., Face, Arm, Speech, Time (FAST), Cincinnati-based algorithms) enhance diagnostic accuracy, coordination, and time efficiency. In the Moldovan context, the FAST and Cincinnati scales were systematically adopted by emergency teams between 2017 and 2021, contributing to more rapid stroke recognition in the prehospital stage [2-5].
Through these integrated strategies, countries can reduce the incidence of acute neurological diseases, thus contributing to global public health and alleviating pressure on healthcare systems. These examples provide models of best practices for any state seeking to strengthen public health and reduce the burden of cerebrovascular disease [6, 7].
The prompt response of Emergency Medical Services (EMS) teams in the prehospital setting is crucial, and the use of protocols plays an important role in ensuring a fast and effective response. These tools enable emergency teams to perform a systematic assessment of the patient's condition and make the right decisions for stabilization and transport. Standardized protocols provide clear guidance, helping ambulance crews recognize and manage neurological emergencies, thereby reducing response times and the risk of complications [8].
International standardization: Organizations such as the WHO, the American Heart Association (AHA), and the European Stroke Organization (ESO) promote standardized algorithms and checklists like ABCDE (Airway, Breathing, Circulation, Disability, Exposure) and SCALE (Screening for Acute Stroke). These frameworks offer a unified structure for EMS teams across different countries, facilitating comparability and efficiency in stroke management. International algorithms are supported by research and studies demonstrating their effectiveness in reducing response times and improving patient outcomes [9, 10].
Material and methods
This observational, retrospective, and descriptive study combined a systematic literature review with a quantitative statistical analysis of national data from the National Prehospital Emergency Medical Service (NPHEMS) of the Republic of Moldova. The aim was to assess the effectiveness of using checklists during prehospital stroke interventions and their impact on the quality of intervention and response times.
Data sources and selection. The analysis included all stroke cases recorded in the national prehospital database between January 1, 2022, and December 31, 2023. Data were extracted from standardized emergency medical service records, including checklist use, algorithm compliance (e.g., FAST, ABCDE), dispatch-to-arrival times, initial evaluation, stabilization, and transport intervals.
A systematic review of scientific publications indexed in PubMed, Scopus, and Google Scholar was also conducted to contextualize the findings with international practices and to support methodological consistency.
Participants and inclusion criteria. Patients included in the analysis met the following criteria:
Suspected stroke according to dispatch notes or prehospital diagnosis;
Managed by mobile emergency teams during the specified period;
Checklist or stroke-specific protocol (FAST, SCALE) documented in the patient chart;
Use of the “Checklist for the assessment of a patient with suspected stroke in the prehospital stage,” which is a method of data collection and a tool that facilitates the establishment of a preliminary diagnosis at the prehospital stage in 2023. The checklist was developed by the authors of the study, based on international recommendations, and adapted to the national context in cooperation with the National Prehospital Emergency Medical Assistance Service. This wording serves to clarify that the checklist is not internationally standardized, but rather derived from best practices and adapted to local requirements.
Exclusion criteria:
Incomplete documentation;
Secondary stroke diagnosis not confirmed or unrelated dispatch code.
Data collection and processing. Data collected through the NPHEMS internal reporting system and structured questionnaires were entered into Microsoft Excel (Microsoft Corp., 2021) for preliminary data processing. Statistical analysis was performed using variational methods (mean, standard deviation, frequency distribution); comparative and correlational analysis (χ², Pearson’s correlation); and discriminant analysis for evaluating intergroup differences in response time and outcomes. For extended statistical evaluation, MedCalc® Statistical Software v.20.218 (2023) was used. A p-value <0.05 was considered statistically significant.
Results and discussion
Neurological emergencies pose a significant challenge for Emergency Medical Services (EMS) in the prehospital stage, being among the conditions with the highest rates of misdiagnosis. This difficulty is amplified by the acute nature of such cases and the necessity for rapid intervention within the therapeutic window to prevent irreversible neurological deterioration. Although it is well understood that every minute counts and that timely and correct prehospital interventions can significantly impact patient prognosis, delays at this stage remain frequent [11, 12].
In the Republic of Moldova, the recognition and management of stroke in the prehospital setting are currently based on the use of the FAST scale, applied both by the medical dispatch center and emergency response teams. This method facilitates the rapid identification of clinical signs of stroke, allowing for prompt and effective intervention.
To improve and standardize prehospital interventions in stroke cases, a specific national checklist has been proposed for the management of this condition. The “Checklist for the assessment of a patient with suspected stroke in the prehospital stage,” implemented in 2023, supports medical personnel during the prehospital phase of care (Fig. 1). This tool aims to ensure a unified and comprehensive approach to the evaluation and treatment of stroke patients in the prehospital phase. The uniform adoption and implementation of checklists and specific guidelines, including at the medical dispatch level, are essential for optimizing patient care and reducing stroke-related mortality and morbidity [13] (Fig. 1).
According to data from the National Prehospital Emergency Medical Service, in 2022, 795,884 calls were serviced - 436,820 in urban areas and 359,064 in rural areas. In 2023, the total number of calls decreased to 744,456, with 397,460 recorded in urban areas and 346,996 in rural areas.
Neurological and neurosurgical emergencies represented a significant proportion during both years. In 2022, 106,152 such cases were reported (54,230 urban and 51,922 rural), and in 2023, the figure remained relatively stable at 104,993 cases (53,573 urban and 51,420 rural). Of these, over 25,000 patients required transport to emergency departments (EDs) each year. Special attention is given to stroke, which accounted for approximately 12,400 cases annually. Among them, the majority were reported as unspecified strokes – over 10,000 cases per year. Ischemic, hemorrhagic, and transient strokes made up the remainder, with a decreasing trend observed in ischemic cases (from 1,358 in 2022 to 867 in 2023).
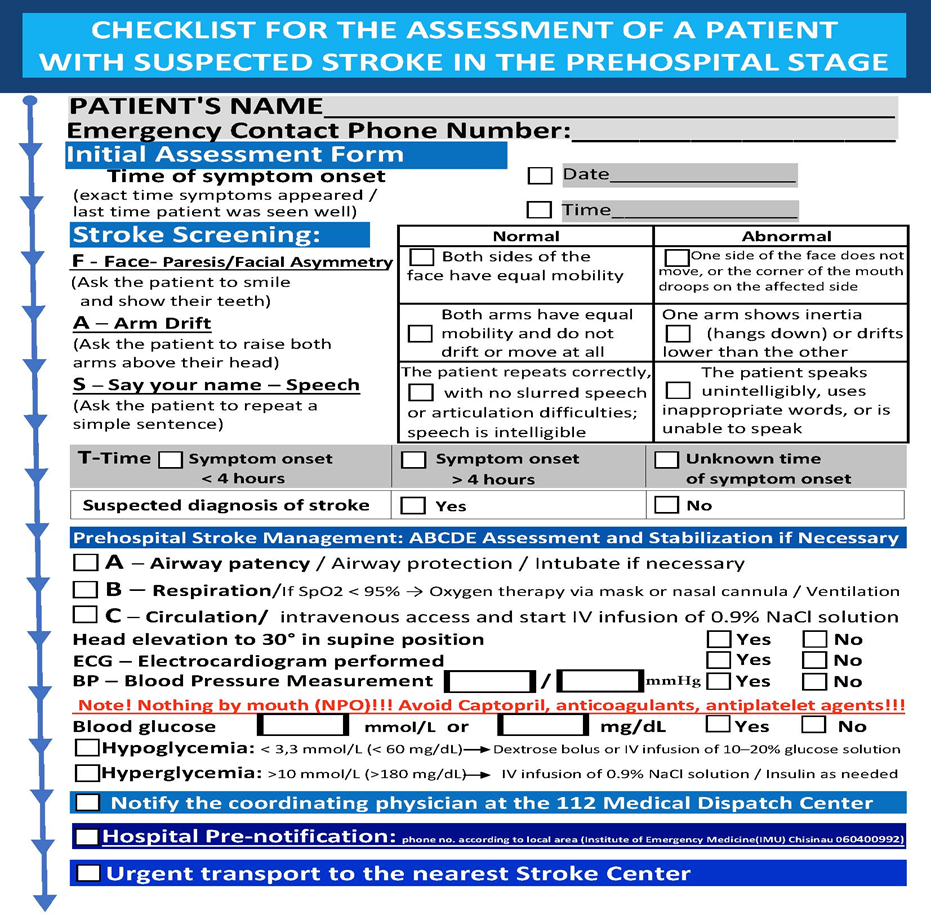 |
Fig. 1 Checklist for the assessment of a patient with suspected stroke in the prehospital stage |
Age group analysis shows that older adults are the most affected. In both years, the majority of stroke cases occurred in patients over the age of 60. In 2023, 4,025 cases were recorded in the 60–70 age group and 6,262 cases among those over 70. The age group under 50 accounted for less than 6% of all stroke cases. The urban-rural distribution remained relatively balanced across all age groups, with a slight predominance of rural cases in the older age categories (Fig. 2) [14, 15].
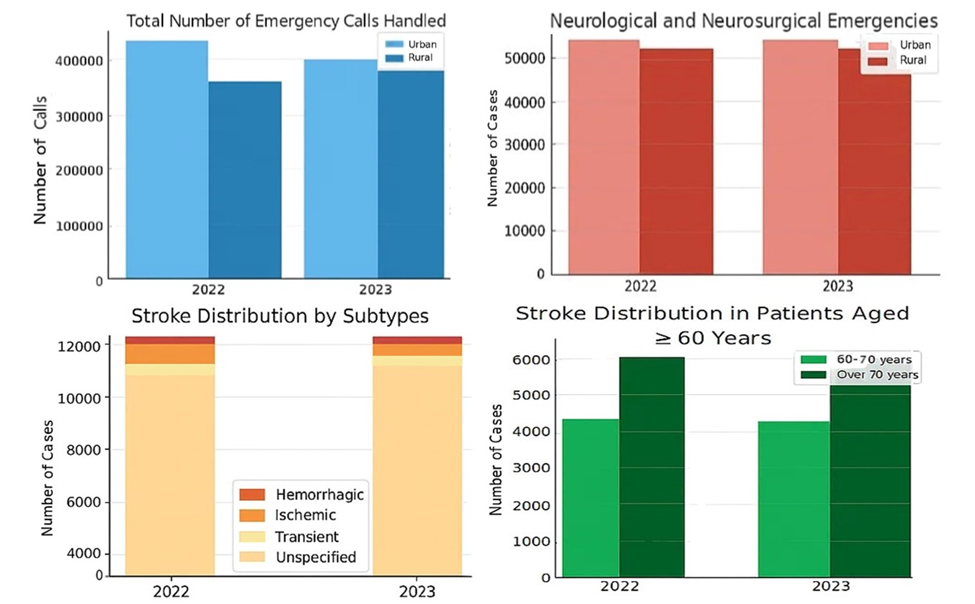 |
Fig. 2 Evolution of neurological emergency requests in the Republic of Moldova in 2022–2023 Note: The upper-left panel illustrates the total number of emergency calls managed, disaggregated by urban and rural areas. The upper-right panel presents neurological and neurosurgical emergency cases by location. The lower-left panel shows stroke cases by subtype (ischemic, hemorrhagic, transient, and unspecified). The lower-right panel indicates stroke distribution among elderly patients aged 60–70 and over 70. The figure highlights a stable volume of neurological emergencies with sustained demand among older age groups. |
In 2022, the average response time to stroke (CVA) cases was 13.23 minutes, while in 2023 it slightly increased to 13.4 minutes. Although the difference is minimal, it may reflect factors such as an increased number of calls, longer travel distances, or possible logistical delays (Fig. 3).
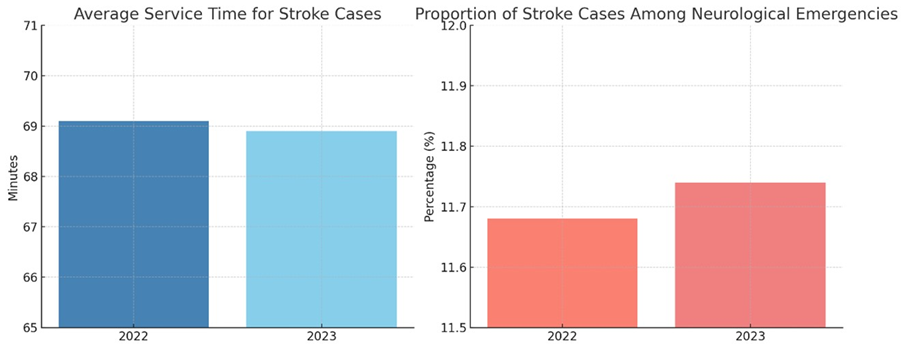 |
Fig. 3 Trends in Stroke Case Management and Proportion Among Neurological Emergencies in the Prehospital stage, 2022–2023 Note: The left panel illustrates a slight reduction in the average service time for stroke cases between 2022 and 2023, indicating a modest improvement in operational efficiency. The right panel shows a marginal increase in the proportion of stroke cases among all neurological emergencies, potentially reflecting enhanced diagnostic accuracy and prehospital identification of stroke. |
The total duration of managing a stroke case – which includes response time, patient evaluation, first aid, and transport to the hospital – has remained relatively stable in recent years. In 2022, the average service time was 69.1 minutes, and in 2023, it slightly decreased to 68.9 minutes. This modest improvement can be attributed to the more efficient application of intervention protocols and the growing experience of emergency teams.
The proportion of stroke cases among all neurological and neurosurgical emergencies has been steadily increasing. In 2022, it was 11.68%, and in 2023, it reached 11.74%. This trend may indicate either a slight increase in the incidence of strokes or an improvement in the identification, diagnosis, and reporting processes.
An essential indicator of prehospital care quality is the percentage of stroke patients transported directly to specialized facilities. As of November 2023, only two tertiary hospitals – the Institute of Emergency Medicine and the Diomid Gherman Institute of Neurology and Neurosurgery in Chisinau – met the criteria to function as multidisciplinary stroke centers. In 2022, 92.8% of patients were transported to these centers, with this figure increasing to 94.2% in 2023, reflecting an improvement in triage capacity and patient routing to appropriate structures.
However, due to the absence of a functional regional network, many patients continued to be initially transported to district hospitals before being transferred to specialized centers in Chișinău. This practice caused significant delays, even for patients identified within the therapeutic window, severely limiting access to specific treatments such as intravenous thrombolysis or mechanical thrombectomy.
As a result, inter-hospital transfers of stroke patients increased significantly from 268 cases in 2022 to 403 cases in 2023. This trend reflects a structural imbalance rather than an increase in efficiency, underlining the need for a functional reorganization of the emergency stroke care system, which was initiated in 2023 (Fig. 4).
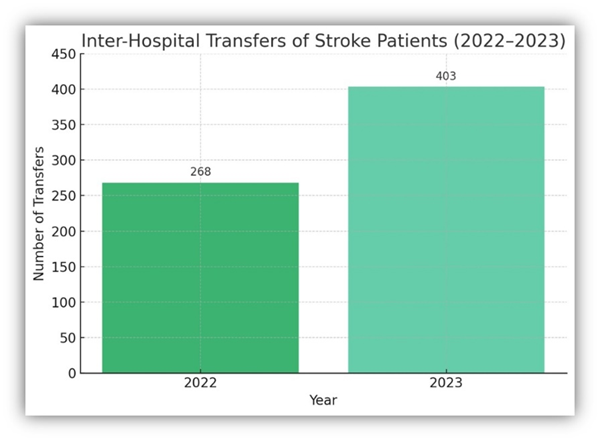 |
Fig. 4 Interhospital transfers of stroke patients in 2022–2023 Note:The bar chart shows the number of stroke patients transferred between hospitals in Moldova in 2022 (n = 268) and 2023 (n = 403). The observed increase suggests a growing need for timely access to specialized stroke care. This trend underscores systemic inefficiencies and reinforces the necessity for continued structural reforms in emergency stroke services. |
To address the existing dysfunctions in the management of stroke cases, the Ministry of Health of the Republic of Moldova proposed, during the College meeting on June 29, 2022, the Concept of Functional and Regional Reorganization of the Stroke Reference, Diagnosis, and Treatment System. This concept provides for organizing services on three levels: Primary Stroke Centers, intended for rapid initial interventions; Multidisciplinary Stroke Centers, for managing complex cases; and a Comprehensive Stroke Center, dedicated to severe cases and coordinated by the Institute of Emergency Medicine in Chișinău [16].
Following the opening of 11 primary stroke centers, a significant increase in the number of thrombolysis performed nationwide was recorded. At the Institute of Emergency Medicine, the thrombolysis rate increased by approximately 61% compared to 2022, highlighting the positive impact of the reorganization on treatment time and access. Additionally, the rate of thrombectomies performed at IEM saw a remarkable rise of about 121%, reflecting both an improvement in technical capacity and the flow of eligible patients [17].
A key indicator for evaluating the quality of rapid intervention is the reduction of critical times, such as door-to-CT time and door-to-treatment administration time. In 2023, these indicators showed a monthly decreasing trend, suggesting better coordination between emergency medical teams and hospital staff [18].
Furthermore, approximately 30% of thrombectomies performed at the Institute of Emergency Medicine in Chișinău were carried out on patients transferred from primary stroke centers, reflecting the effective functioning of the new referral network and the strengthening of the clinical pathway for stroke patients.
A notable progress in 2024 was that the primary stroke centers in the district hospitals of Florești, Căușeni, Hîncești, and Soroca performed intravenous thrombolysis procedures for the first time. At the primary center level, the thrombolysis rate stood at 9.3%, a promising indicator for a system in the process of development and consolidation [17, 19].
Equally important was the integration of standardized checklists in the prehospital phase, which significantly contributed to the streamlining of stroke care. These checklists enabled EMS teams to assess neurological symptoms more systematically, reduce diagnostic uncertainty, and ensure the timely relay of essential clinical information to receiving hospitals. Their implementation helped unify the prehospital approach across regions, facilitated earlier identification of eligible candidates for reperfusion therapy, and reduced the risk of delays caused by incomplete or inconsistent initial evaluations.
These advancements reflect the efforts of the Republic of Moldova to build a modern and functional healthcare system that provides rapid, standardized, and high-quality interventions for stroke patients. During the analyzed period, a positive trend in the quality and efficiency of prehospital services is evident, demonstrated by reduced service times, increased transport rates to specialized centers, and improved early recognition of clinical signs by emergency teams.
To optimize the initial assessment of neurological patients, implementing standardized checklists for all acute neurological conditions is essential. Although the FAST scale remains a valuable tool for rapid stroke identification, recent evidence demonstrates that more comprehensive checklists significantly improve diagnostic accuracy, interprofessional communication, and early initiation of treatment protocols. For example, a 2023 study validating a prehospital nomogram for differentiating hemorrhagic from ischemic stroke showed enhanced triage precision [20]. Moreover, a quality improvement initiative in emergency departments reported that using stroke evaluation checklists increased the odds of delivering thrombolytic therapy within 60 minutes of arrival (OR 6.4; 95% CI 1.1–68.7), underscoring the benefit of structured tools in acute neurological care [3].
The present study is constrained to the prehospital stage in the Republic of Moldova, within the context of the application of the checklist by emergency medical teams.
Conclusions
The implementation of standardized checklists in the prehospital management of stroke has improved the accuracy, timeliness, and coordination of emergency medical interventions in the Republic of Moldova. These tools, alongside system-wide reorganization, have contributed to increased access to reperfusion therapies and better clinical outcomes. Continued integration and training remain essential to sustain these improvements and reduce stroke-related morbidity and mortality.
Competing interests
None declared.
Authors’ contributions
NC – substantial contribution to the conception and design of the work, substantial contribution to data acquisition, substantial contribution to data analysis and interpretation, taking responsibility for and being accountable for all aspects of the work. MP – substantial contribution to the conception and design of the work, substantial contribution to data acquisition, substantial contribution to data analysis and interpretation, drafting the article, taking responsibility for and being accountable for all aspects of the work. LR – critical review of the article for important intellectual content, taking responsibility for and being accountable for all aspects of the work. NM – drafting the article. All authors critically reviewed the work and approved the final version of the manuscript.
Informed consent for publication
Informed consent was not required, as only anonymized, retrospective data were used and no direct patient involvement occurred.
Acknowledgements and funding
No external funding was received.
Ethics approval
The study protocol was approved by the Research Ethics Committee of the Nicolae Testemițanu State University of Medicine and Pharmacy (no. 38, dated 02.04.2013).
Provenance and peer review
Not commissioned, externally peer-reviewed.
Authors’ ORCID IDs
Natalia Catanoi – https://orcid.org/0000-0002-5838-0363
Mihail Pestereanu – https://orcid.org/0000-0002-9797-2919
Larisa Rezneac – https://orcid.org/0000-0001-7545-1728
Natalia Mocanu – https://orcid.org/0000-0001-5989-4553
References
Manole E, Tiu C, Vilionskis A, Tsiskaridze A, Zota E, Grecu A, et al. Stroke care indicators in the Republic of Moldova – the RES-Q registry. Mold J Health Sci. 2022;(1):32-34. https://doi.org/10.52645/MJHS.2022.1.03
Ministerul Sănătății al Republicii Moldova [Ministry of Health of the Republic of Moldova]; Groppa S, Gavriliuc M, Zota E, et al. Accidentul vascular cerebral ischemic: Protocol clinic național [Ischemic stroke: National clinical protocol]. Chisinau: The Ministry; 2017. 112 p. (PCN-13). Romanian.
Elam M, Moyal-Smith R, Canfora M, Cohen W, Eum KD, Fischer C, Margo J, McCune M, Moin O, Selim M, Wendell L, Kumar S. A checklist to improve acute stroke evaluation and treatment in the emergency department. Am J Med Qual. 2025 Mar-Apr 01;40(2):53-63. doi: 10.1097/JMQ.0000000000000217.
Kessler C, Khaw AV, Nabavi DG, Glahn J, Grond M, Busse O. Standardized prehospital treatment of stroke. Dtsch Arztebl Int. 2011 Sep;108(36):585-91. doi: 10.3238/arztebl.2011.0585.
Catanoi N. Managementul accidentului vascular cerebral ischemic la etapa de prespital în Republica Moldova = Management of ischemic stroke at the prehospital stage in the Republic of Moldova. Mold J Health Sci. 2022;(3 Suppl):73. Romanian, English.
Luiz T, Moosmann A, Koch C, Behrens S, Daffertshofer M, Ellinger K. Optimized logistics in the prehospital management of acute stroke. Anasthesiol Notfallmed Schmerzther. 2001;36(12):735-41. doi: 10.1055/s-2001-18981. German.
Feigin VL, Roth GA, Naghavi M, Parmar P, Krishnamurthi R, Chugh S, et al. Global burden of stroke and risk factors in 188 countries, during 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol. 2016;15(9):913-924.https://doi.org/10.1016/S1474-4422(16)30073-4.
Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344-e418. doi: 10.1161/STR.0000000000000211.
Bernic V, Ciobanu N, Ciocanu M, et al. Accidentul vascular cerebral: epidemiologie, factori de risc, prevenție [Stroke: epidemiology, risk factors, prevention]. Groppa S, editor. Chișinău: [s. n.]; 2020. 212 p. Romanian.
Zachrison KS, Nielsen VM, Perez de la Ossa N, et al. Prehospital stroke care Part 1: Emergency medical services and the stroke systems of care. Stroke. 2023;54(4):1138-1147. doi: 10.1161/STROKEAHA.122.039586.
Guvernul Republicii Moldova [Government of the Republic of Moldova]. Programul național de prevenire și control al bolilor netransmisibile prioritare în Republica Moldova pentru anii 2023-2027 [National Program for the Prevention and Control of Priority Noncommunicable Diseases in the Republic of Moldova for 2023-2027]. Chisinau: The Government; 2023. Romanian.
Ministerul Sănătății al Republicii Moldova [Ministry of Health of the Republic of Moldova]. Ordinul nr. 870 din 16.10.2023 cu privire la organizarea Serviciului național de asistență medicală al AVC [Order no. 870 of 16.10.2023 on the organization of the National Stroke Medical Assistance Service] [Internet]. [cited 2025 May 12]. Available from: https://ms.gov.md/wp-content/uploads/2023/10/870-16.10.2023.pdf. Romanian.
Catanoi N. Hipertensiunea arterială complicată cu accident vascular cerebral la etapa de prespital [Arterial hypertension complicated with stroke in the prehospital stage] [dissertation]. Chișinău: Nicolae Testemițanu State University of Medicine and Pharmacy; 2024. 155 p. Romanian.
National Center for Pre-Hospital Emergency Medical Assistance of the Republic of Moldova. Raport de activitate pentru anul 2022 [Annual Activity Report 2022] [Internet]. Chisinau: The Center; 2022 [cited 2025 Apr 14]. Available from: https://ambulanta.md/rapoarte-%C8%99i-statistici. Romanian.
National Center for Pre-Hospital Emergency Medical Assistance of the Republic of Moldova. Raport de activitate pentru anul 2023 [Annual Activity Report 2023] [Internet]. Chisinau: The Center; 2023 [cited 2025 Apr 14]. Available from: https://ambulanta.md/storage/uploads/Rapoarte%20%C8%99i%20statistici/09.02.2024%20Raport%20activitate%20pentru%202023.pdf. Romanian.
Ministerul Sănătăţii al Republicii Moldova [Ministry of Health of the Republic of Moldova]. Acces la asistență medicală calificată în 13 centre pentru pacienții care au suferit accident vascular cerebral [Access to specialized medical care in 13 centers for patients who have suffered a stroke] [Internet]. 2023 Oct 16. Chișinău: The Ministry; 2023- [cited 2025 Jun 12]. Available from: https://ms.gov.md/comunicare/comunicate/acces-la-asistenta-medicala-cal…; or on: https://emedicina.md/13-centre-pentru-pacientii-cu-avc-vor-fi-infiintat…. Romanian.
Institute of Emergency Medicine of the Republic of Moldova. Rapoarte de activitate 2023-2024 [Annual Reports 2023-2024]. Chisinau: The Institute; 2024 [cited 2025 May 12]. Available from: https://www.urgenta.md/rapoarte.html. Romanian.
Ministry of Health of the Republic of Moldova. Raportul de activitate pentru anul 2024 [Activity report for 2024] [Internet]. Chisinau: The Ministry; 2024 [cited 2025 May 12]. Avalable from: https://ms.gov.md/wp-content/uploads/2024/12/Raport-de-actvitate-al-MS-…. Romanian.
National Agency for Public Health of the Republic of Moldova. Săptămâna globală de acțiuni pentru prevenirea bolilor netransmisibile [Global Week of Action for the Prevention of Noncommunicable Diseases] [Internet]. Chisinau: The Agency; 2023 [cited 2025 May 12]. Available from: https://ansp.md/apelul-in-saptamana-globala-de-actiuni-pentru-prevenirea-bolilor-netransmisibile-din-acest-an-este-sa-reducem-decalajul-in-ingrijirile-medicale. Romanian.
Ye S, Pan H, Li W, Wang J, Zhang H. Development and validation of a clinical nomogram for differentiating hemorrhagic and ischemic stroke prehospital. BMC Neurol. 2023;23(1):95. https://doi.org/10.1186/s12883-023-03138-1.