
Introduction
Following the introduction of anti-D immunoglobulin prophylaxis in 1968, the incidence of immune fetal hydrops decreased significantly [1]. Currently, non-immune etiologies account for approximately 95% of all cases of fetal hydrops [1, 2].
Historically, NIHF was considered a lethal condition. However, understanding NIHF as a clinical sign of a wide spectrum of underlying disorders, together with advances in prenatal diagnosis, neonatal intensive care, and pediatric surgery, has changed this perception [3, 4]. Cardiovascular malformations represent the most frequent etiology of NIHF (21.4%), followed by idiopathic causes (18.2%), chromosomal abnormalities (12.5%), hematologic disorders (10.1%), and congenital lymphatic dysplasia (7.5%). Infections account for 6.8% of NIHF cases, with the most common being parvovirus B19, cytomegalovirus, adenovirus, and enterovirus infections [1].
Maternal infection with Treponema pallidum can affect the fetus at all stages of the disease, regardless of the gestational trimester. During the primary and secondary stages of syphilis, the likelihood of vertical transmission from an untreated pregnant woman to her fetus approaches 100% [1]. The global prevalence of congenital syphilis is increasing, rising from 203 cases per 100,000 live births in 2015 to 295 cases per 100,000 in 2021 [5]. Clinical manifestations of fetal infection with Treponema pallidum include hepatosplenomegaly, thymic involution, placentomegaly, increased peak systolic velocity in the middle cerebral artery (a marker of fetal anemia), ascites, low birth weight, fetal hydrops, preterm birth, and perinatal death [6, 7]. Proinflammatory cytokines and an imbalance of angiogenic factors (PlGF – placental growth factor, VEGF – vascular endothelial growth factor) induce endothelial injury, contributing to placental dysfunction characteristic of Ballantyne syndrome (“mirror syndrome”) [8].
Case presentation
According to the anamnestic and serological data, maternal syphilitic infection was acquired during the current pregnancy, most likely in the second or third trimester of gestation, and was serologically detected in the active stage (primary syphilis). The absence of specific etiological treatment favored transplacental transmission of the infection and the development of a severe form of congenital syphilis.
We report the case of a preterm neonate born at 31 weeks of gestation, with a birth weight of 2254 g, body length of 42 cm, head circumference of 32 cm, and Apgar scores of 3 and 5 at 1 and 5 minutes, respectively. The pregnancy was complicated by untreated maternal primary syphilis, intrauterine infection, and polyhydramnios.
At birth, the neonate was in an extremely critical condition, presenting with generalized edema, severe respiratory distress, marked abdominal distension, and hemorrhagic cutaneous lesions. The abdominal circumference measured at the level of the umbilical stump was 36 cm. Endotracheal intubation was performed in the first minute of life, and the patient was placed on mechanical ventilation. Ultrasonography revealed hepatomegaly, a large amount of free intraperitoneal fluid, and intestinal loops compressed toward the posterior abdominal wall. Subsequent computed tomography confirmed the ultrasound findings, demonstrating hepatomegaly (right lobe 7.0 cm, left lobe 2.6 cm) extending into the splenic space with a mass effect displacing the spleen medially and caudally; the splenic size remained within normal limits. Abdominal radiography showed pronounced distension with an absence of intraluminal intestinal gas. Chest imaging revealed severe type I respiratory distress syndrome, right-sided polysegmental pneumonia, alveolar pulmonary edema, and marked cardiomegaly. Transthoracic echocardiography demonstrated nondilated cardiac chambers with preserved left ventricular systolic function. A patent foramen ovale (PFO) with a left-to-right shunt at the interatrial septum measuring 3 mm was identified, along with false chordae tendineae in the left ventricular cavity. Mild tricuspid regurgitation (grade I) and mild pulmonary valve regurgitation (grade I) were present, associated with mild pulmonary hypertension, estimated echocardiographically by a systolic pulmonary artery pressure of approximately 39 mmHg.
At 2 hours of life, a right-sided drainage microlaparotomy was performed, with the evacuation of clear serous ascitic fluid. The abdominal circumference decreased by 2 cm. Over time, ventilatory support parameters were reduced, while corrective measures addressed anemia (Hb 59 g/L, Ht 17%), thrombocytopenia (platelets 22 × 109/L), hypoproteinemia (total protein 39.26 g/L), and hypoglycemia (glucose 1.1 mmol/L). Neonatal serology confirmed active treponemal infection, and microbiological investigations excluded other bacterial infectious etiologies. During the course of the disease, the neonate developed syphilitic infectious hepatitis (ALT 278 U/L, AST 333 U/L) associated with severe cholestasis, evidenced by a total bilirubin level of 235.62 µmol/L with a predominance of direct bilirubin (192.12 µmol/L, approximately 82% of the total), consistent with syphilitic hepatocellular injury. Acute renal impairment was also documented (urea 28.46 mmol/L, creatinine 166.38 µmol/L). Radiography of the long bones demonstrated metaphyseal syphilitic osteochondritis (Fig. 1).
 |
Fig. 1 Radiograph of the long bones showing metaphyseal changes suggestive of congenital syphilitic osteochondritis (metaphyseal irregularity and areas of osteolysis). |
By the 8th day of life, the general condition showed slight improvement, and regression of respiratory failure allowed de-escalation of ventilatory therapy to noninvasive support.
On the 12th day of life, given the presence of blood streaks in the gastric aspirate, progressive abdominal distension, the absence of meconium passage since birth, and a lack of stool following a cleansing enema, an upright abdominal radiographic study with contrast at predefined intervals was performed (Fig. 2). This revealed retention of contrast within the small intestine, suggestive of meconium ileus, which was subsequently confirmed by computed tomography. The neonate underwent segmental small bowel resection with end-to-end enteroenterostomy. The postoperative diagnosis was: “Congenital distal intestinal obstruction. Ileal stenosis. Diffuse serofibrinous peritonitis. Fetal hepatitis.”
A 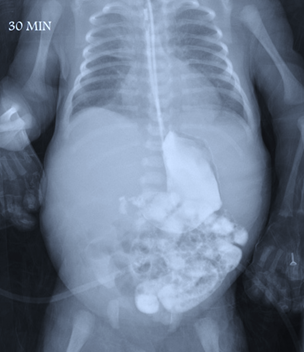 | B 
| C 
|
Fig. 2 Serial upright abdominal radiographs A - 30 minutes, B - 3 hours, and C - 24 hours following administration of an iodinated contrast medium (Ultravist), demonstrating a lack of distal progression and retention of contrast within the small intestine. | ||
The postoperative course was complicated by anemia, thrombocytopenia, pulmonary hemorrhage, toxic hepatitis, retinopathy of prematurity stage I–II, and neonatal jaundice. The neonate was weaned from ventilatory support 4 days postoperatively and passed stool on the 7th postoperative day. Histopathological examination confirmed the postoperative diagnosis, revealing connective tissue with micro- and macrofocal hemorrhages, intravascular erythrocyte thrombi, and focal and diffuse lymphocytic infiltration. The infant was completely weaned from oxygen support at 46 days of life and discharged in a satisfactory condition at 73 days of life.
Antepartum, maternal manifestations of NIHF included moderate peripheral edema, hypoalbuminemia (albumin 30.80 g/L), and hemodilution (urea 2.11 mmol/L, creatinine 39.80 µmol/L), which persisted postpartum. Histopathological examination of the placenta revealed discirculatory-anemic placentopathy associated with amnionitis.
Discussion
Although syphilitic infection is a preventable and treatable condition through prenatal screening and appropriate antimicrobial therapy, it continues to represent a public health problem, particularly in regions with limited access to healthcare services. The persistence of congenital syphilis cases primarily reflects deficiencies in the early detection of maternal infection and delayed or absent initiation of etiological treatment. The lack of adequate treatment during pregnancy is associated with increased perinatal mortality, severe neonatal morbidity, and long-term sequelae.
The present case demonstrates that untreated congenital syphilis may progress with severe systemic manifestations, including multiorgan involvement and rare surgical complications, requiring complex multidisciplinary interventions to ensure survival. Preterm neonates exhibit immature intestinal motility and a vascular system predisposed to injury, which may facilitate the extension of inflammatory lesions and increase susceptibility to severe intestinal obstruction in the context of treponemal inflammation [9]. The presence of non-immune fetal hydrops indicates an advanced stage of congenital infection and reflects the systemic impact of fetal inflammation and associated placental dysfunction. The pathogenic mechanisms involved include fetal anemia secondary to hemolysis, high-output cardiac failure, hepatic impairment with hypoalbuminemia, and placental dysfunction caused by treponemal vasculitis. These mechanisms cumulatively contribute to fluid accumulation in the fetal compartments and the development of hydropic syndrome.
Antenatal diagnosis of intestinal stenosis or obstruction remains challenging and is primarily based on indirect imaging findings. Fetal ultrasonography may reveal dilated bowel loops, increased echogenicity, and reduced or absent peristalsis, frequently associated with polyhydramnios and intrauterine growth restriction. Fetal magnetic resonance imaging (MRI) can provide additional information regarding meconium distribution and the probable level of obstruction. However, precise confirmation of the affected segment and the degree of stenosis is achieved in most cases postnatally, sometimes only during the surgical intervention [10].
In the present case, the antenatal diagnosis of fetal hydrops allowed anticipation of a guarded neonatal prognosis and facilitated the early initiation of intensive supportive measures immediately after birth. Prompt intervention through early ascitic drainage was essential to reduce intra-abdominal pressure, improve respiratory mechanics, and achieve hemodynamic stabilization. The combination of invasive respiratory support, hematological corrections, and anti-infective therapy played a decisive role in the initial stabilization of the neonate.
A particular feature of this case is the association of fetal hydrops with distal congenital intestinal obstruction. The literature describes only isolated cases of intestinal obstruction or necrotizing enterocolitis associated with congenital syphilis, and the causal relationship remains insufficiently elucidated [7, 11]. In the absence of specific histopathological evidence of treponemal obliterative vasculitis at the intestinal level, a direct causal link cannot be established. Nevertheless, prenatal systemic inflammation, mesenteric ischemia, and subclinical vascular injury may represent plausible contributory mechanisms.
The postoperative course was marked by complications commonly encountered in severe congenital syphilis, necessitating close monitoring and continuous therapeutic adjustments. The progressive recovery and survival of the neonate underscore the importance of an integrated multidisciplinary approach involving neonatologists, pediatric surgeons, infectious disease specialists, and intensive care physicians.
Another relevant aspect of this case is the presence of maternal manifestations associated with fetal hydrops, consistent with Ballantyne syndrome (“mirror syndrome”). Maternal edema, hemodilution, and hypoproteinemia suggest the involvement of placental dysfunction and angiogenic imbalance in the pathogenesis of this syndrome. Early recognition of maternal signs may serve as an additional indicator for assessing the severity of fetal involvement.
Prevention of congenital syphilis remains essential, as once fetal hydrops develops, the neonatal prognosis is often unfavorable, and postnatal interventions become complex and resource-intensive. Systematic screening of pregnant women, repeat testing in subsequent trimesters for high-risk populations, and the prompt treatment of maternal infection are key measures for reducing the incidence of these severe forms.
In line with the existing literature, this report highlights the need for increased clinical vigilance regarding atypical and rare manifestations of congenital syphilis. The limitations of this report include its single-center nature and the inability to establish a definitive causal relationship between treponemal infection and intestinal malformation, underscoring the need for further studies to clarify these rare associations.
Conclusions
This case demonstrates that even severe congenital syphilis complicated by non-immune fetal hydrops may result in a favorable outcome when an early diagnosis and timely, coordinated multidisciplinary management are ensured. The report underscores the essential role of systematic prenatal screening for maternal treponemal infection and the importance of integrated perinatal care in improving survival and reducing severe neonatal morbidity.
Competing interests
None declared.
Acknowledgements and funding
No external funding.
Authors’ contributions
AN contributed to the acquisition, analysis, and interpretation of the primary data, and LC participated in the study design and drafted the manuscript. All authors critically reviewed the work and approved the final version of the manuscript.
Ethics approval
Not needed for this study.
Informed consent for publication
Obtained.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Authors’ ORCID IDs
Anastasia Neagu – https://orcid.org/0009-0005-6042-4926
Larisa Crivceanscaia – https://orcid.org/0000-0003-4388-374X
References
Dysart K, Moldenhauer J. Nonimmune hydrops fetalis. In: Eichenwald E, Hansen A, Martin C, Stark A, editors. Cloherty and Stark’s Manual of neonatal care. 9th ed. Philadelphia: Wolters Kluwer; 2023. p. 52-64.
Crivceanscaia L, Pintea I. Sifilis congenital [Congenital syphilis]. In: Crivceanscaia L, et al. Protocoale clinice standardizate pentru secțiile neonatale [Standardized clinical protocols for neonatal units]. Chisinau; 2022. p. 288-295. Romanian.
Pegoraro V, Urbinati D, Visser G, Renzo G, Zipursky A, Stotler B, et al. Hemolytic disease of the fetus and newborn due to Rh(D) incompatibility: a preventable disease that still produces significant morbidity and mortality in children. PLoS One. 2020;15(7):e0235807. doi: 10.1371/journal.pone.0235807.
Swearingen C, Colvin Z, Leuthner S. Nonimmune hydrops fetalis. Clin Perinatol. 2020;47(1):105-121. doi: 10.1016/j.clp.2019.10.001.
Duan B, Zhou Y, Wang X, Wang H, Li Y, Zhou X, et al. Congenital syphilis: adverse pregnancy outcomes and neonatal disorders. Infection. 2025;53(6):2303-2319. doi: 10.1007/s15010-025-02591-z.
Rac M, Revell P, Eppes C. Syphilis during pregnancy: a preventable threat to maternal-fetal health. Am J Obstet Gynecol. 2017;216(4):352-363. doi: 10.1016/j.ajog.2016.11.1052.
Serra G, Carta M, Pace MR, Sala E, Piro E, Salerno S, Schierz IA, Vassallo A, Giuffrè M, Corsello G. Congenital syphilis in a preterm newborn with gastrointestinal disorders and postnatal growth restriction. Ital J Pediatr. 2022;48(1):205. doi: 10.1186/s13052-022-01404-5.
Chandra S, Chowdhury S. Systemic effect of different physiological parameter associated with mirror syndrome. J Obstet Gynaecol Res. 2025;51(9):e70062. doi: 10.1111/jog.70062.
Lee HS, Lee JI, Jeon J. Congenital syphilis unusually presenting with prematurity-related severe neonatal morbidities including meconium obstruction: a case report and review of the literature. Medicine (Baltimore). 2020;99(40):e22321. doi: 10.1097/MD.0000000000022321.
Rubio EI, Blask AR, Badillo AT, Bulas DI. Prenatal magnetic resonance and ultrasonographic findings in small-bowel obstruction: imaging clues and postnatal outcomes. Pediatr Radiol. 2017;47(4):411-421. doi: 10.1007/s00247-016-3770-0.
Çelik M, Bülbül A, Uslu S. Congenital syphilis presenting with prenatal bowel hyperechogenicity and necrotizing. Med Bull Şişli Etfal Hospital. 2020;54(1):113-116. doi: 10.14744/SEMB.2018.22605.