
Introduction
The coexistence of frailty and cardiovascular diseases is recognized, yet remains an emerging concept in cardiology, with reported prevalence ranging from 19% to 76%. In the context of chronic heart failure (CHF), the prevalence of sarcopenia ranges from 11-12% in stable conditions to up to 65% among inpatients. In frail patients with heart failure, the presence of sarcopenia significantly influences clinical decision-making, especially regarding the selection and timing of diagnostic and therapeutic approaches. On the other hand, frailty and sarcopenia are major syndromes with a significant impact on the course of CHF, due to the reduction of physiological reserves and a diminished ability to adapt to both endogenous and exogenous stressors. In CHF, these conditions frequently coexist, amplifying the risk of decompensation, hospitalization and mortality [1, 2].
Although introduced by Rosenberg in 1989 to define age-related muscle mass and strength decline, sarcopenia was only officially classified as a disease by the World Health Organization in 2016. It is defined as the age-related loss of muscle mass and function and is associated with frequent falls, osteoporosis and increased mortality. The prevalence of sarcopenia among individuals over 65 years old ranges between 6% and 22%, escalating with age [3].
Several international expert groups such as the International Working Group on Sarcopenia, the Asian Working Group for Sarcopenia (AWGS), and the European Working Group on Sarcopenia in Older People (EWGSOP2) have attempted to create a standardized definition and diagnostic system. A stepwise assessment approach F-A-C-S (Find, Assess, Confirm, Severity) is commonly recommended, beginning with screening questionnaires, followed by evaluation of muscle strength and concluding with severity evaluation based on physical performance and muscle mass. Despite these efforts, a universally accepted definition and diagnostic tool remain lacking [4].
Various tools are available for sarcopenia assessment, including the SARC-F questionnaire, its extended SARC-Calf version (incorporating calf circumference), handgrip strength, chair stand test, gait speed, the Short Physical Performance Battery (SPPB), the Timed Up and Go (TUG) test, and the 6-minute walk test. Recommended imaging modalities include dual-energy X-ray absorptiometry (DXA), bioelectrical impedance analysis (BIA), computed tomography (CT), and magnetic resonance imaging (MRI). Where advanced technologies are unavailable, anthropometric assessments serve as a validated and practical alternative. International guidelines endorse these methods, while highlighting the importance of adapting them to specific population contexts [5-7].
Considering that sarcopenia is a recognized component of physical frailty that impairs functionality and often remains underdiagnosed, we conducted a study focused on assessing sarcopenia in frail patients with chronic heart failure.
This study aimed to assess sarcopenia in patients with chronic heart failure (CHF) and frailty syndrome, focusing on the identification of both risk and protective factors to support early diagnosis and inform personalized clinical management.
Material and methods
An observational, cross-sectional study was conducted on 44 frail patients hospitalized for decompensated chronic heart failure between January and June 2025 at the Institute of Cardiology. Inclusion criteria comprised a confirmed diagnosis of CHF, frailty identified using the 11-item Edmonton Frail Scale and signed informed consent (approval № 48, issued on 23 May 2024). Exclusion criteria included acute exacerbations of comorbidities, conditions interfering with anthropometric evaluation (e.g., pressure ulcers, significant edema, recent thrombosis, or lower limb deformities) and cognitive impairment precluding reliable assessment.
Data were collected using a structured questionnaire encompassing demographic characteristics (including marital status: single, married, divorced, widowed), anthropometric measurements, cardiovascular risk factors, comorbidities, laboratory parameters (serum glucose, lipid profile, NT-proBNP, creatine kinase – CK, and C-reactive protein – CRP), as well as instrumental findings such as a resting electrocardiogram (ECG).
Comorbidities were evaluated using the Charlson Comorbidity Index, which stratifies patients as follows: 0 points (no comorbidities), 1-2 points (low), 3-4 points (moderate), and ≥5 points (high comorbidity burden). Sarcopenia assessment was conducted in accordance with EWGSOP2 recommendations, applying the F-A-C-S algorithm (Find-Assess-Confirm-Severity). Initial screening involved the SARC-Calf questionnaire, and patients scoring ≥4 underwent further evaluation, including muscle strength via the chair stand test, muscle mass by calf circumference (CC), and physical performance through the Timed Up and Go (TUG) test and gait speed. Calf circumference was the primary indicator of muscle mass, with thresholds of <34 cm for men and <33 cm for women indicating low muscle mass. Measurements were taken with the patient seated, knee flexed at 90°, and the muscle relaxed at the widest point of the calf. Each measurement was performed twice, with the highest value recorded.
Patients were categorized into three groups: Study Group 1 (G1) – mild frailty, Study Group 2 (G2) – moderate frailty, and Study Group 3 (G3) – severe frailty. Comparative and correlational analyses were conducted across groups, evaluating sociodemographic, clinical, biological, and instrumental variables, alongside risk factors, comorbidities, and treatment regimens. Logistic regression models were used to analyse the associations between clinical data, functional and laboratory parameters, and the presence of sarcopenia in frail CHF patients. Odds Ratios (OR) and 95% Confidence Intervals (CI) were reported, and a p < 0.05 was considered statistically significant. Data analysis was performed using SPSS software.
Results
The study included 44 patients with a mean age of 67.3 ± 8.9 years (range: 43-82 years), of whom 32 (72.7%) were female and 12 (27.3%) were male. Marital status distribution included 25 (56.8%) married individuals, 14 (31.8%) widowed, 3 (6.8%) divorced, and 2 (4.5%) single. Regarding social status, most participants were retired (61.4%), followed by those with varying degrees of disability (20.5%), employed individuals (15.9%), and a single unemployed patient (2.3%). Regarding heart failure etiology, ischemic heart disease was identified in 70.5% of patients, while 29.5% had a non-ischemic origin, primarily of valvular etiology (accounting for 69.2% of non-ischemic cases). Heart failure phenotypes were predominantly represented by patients with reduced ejection fraction (HFrEF, 45.5%), followed by those with preserved ejection fraction (HFpEF, 40.9%) and mildly reduced ejection fraction (HFmrEF, 13.6%). Using the SARC-Calf questionnaire, 25 (56.8%) patients were identified as being at increased risk of sarcopenia (OR = 4.11; 95% CI: 0.62-27.10; p = 0.048), and 7 (15.9%) were diagnosed with severe sarcopenia based on the EWGSOP2 algorithm. Comorbidities were assessed using the Charlson Comorbidity Index, which showed a mean score of 4.8 (range 1-9), indicating a high burden of associated chronic conditions.
Patients were stratified into three groups based on frailty severity, assessed by the Edmonton Frail Scale: Study Group 1 (G1) – mild frailty (8-9 points), included 27 (61.4%) patients; Study Group 2 (G2) – moderate frailty (10-11 points), included 12 (27.3%) patients; and Study Group 3 (G3) - severe frailty (12-17 points), included 5 (11.7%) patients.
A progressive increase in age was noted across frailty categories, with mean ages of 66.2 ± 8.7 years in G1, 68.0 ± 10.4 years in G2, and 71.6 ± 6.7 years in G3, indicating a positive correlation between advancing age and frailty severity. Female patients predominated in all groups, accounting for 40.9% in G1, 22.7% in G2, and 9.1% in G3, while male representation declined with increasing frailty. Social dependency also showed a proportional rise with frailty. In G1, 13.6% of patients were employed, 2.3% unemployed, 31.8% retired, and 13.6% reported disability. In G2, only 2.3% remained employed, while 20.5% were retired and 4.5% disabled. All G3 patients were either retired (9.1%) or disabled (2.3%). Marital status distribution revealed a predominance of married individuals in the mild frailty group (38.6%), whereas widowed individuals were more common in the moderate (15.9%) and severe (4.5%) frailty groups, suggesting a possible association between living alone and increased frailty.
The baseline patient characteristics are summarized in Table 1.
Table 1. Association of clinical parameters with sarcopenia risk and severe sarcopenia according to frailty severity. | |||||||||||||
Parameter | OR L1 | Risc L2 | OR L2 | Risc L3 | OR L3 | Sarc L1 | OR L1 | Sarc L2 | OR L2 | Sarc L3 | OR L3 | p | Risc L1 |
QUALITATIVE | |||||||||||||
| 1.Hypertension | 13 | 0.39 | 8 | 1,7 | 4 | 3,4 | 5 |
| 2 | 0 | 0 |
|
|
| 2. Obesity | 8 | 1.6 | 6 | 3.0 | 3 | 2,6 | 4 | 8.0 | 2 | 0 | 0 | 0 | 0.44 |
| 3.Dislipidemia | 5 | 0.6 | 2 | 0 | 0 | 0,4 | 3 | 0.75 | 0 | 0 | 0 | 0 |
|
| 4. Diabetes mellitus | 2 | 0.66 | 2 | 1.8 | 0 | 0.4 | 2 | 0 | 2 | 0 | 0 | 0 | 0.21 |
| 5. Smoking | 12 |
| 8 | 0 | 4 | 3,8 | 0 | 0 | 0 | 0 | 0 | 0 | 0.71 |
| 6. Preserved physical activity | 8 | 0.88 | 6 | 1.0 | 3 |
| 2 | 0.7 | 2 | 0 | 0 | 0 |
|
| 7. Reduced muscle strength | 14 | 0.3 | 9 | 1.0 | 4 | 2,8 | - | - | - | - | - | - | 0.12 |
| 8. Impaired physical performance | 11 | 0.4 | 11 | 0 | 5 | 1,14 | - | - | - | - | - | - | 0.79 |
| 9. Sleep duration < 5 hours | 3 | 0,22 | 4 | 0.33 |
|
| 4 | 0 | 2 | 0 | 0 | 0 |
|
| 10. Charlson Index ≥5 | 10 | 0.8 | 5 | 0.33 | 4 | 6,4 |
| 0 |
| 0 |
| 0 | 0.17 |
| 11. Metformin use | 0 |
| 3 | 1.8 | 3 |
| 5 | 0 | 2 | 0 | 0 | 0 | 0.008 |
| 12. Statine use | 11 | 0.33 | 4 | 0 | 2 |
| 4 | 0 | 0 | 0 | 0 | 0 | 0.07 |
QUANTITATIVE | |||||||||||||
| 1. Mean age ± SD (years) | 65,2 ± 8,7 |
| 70,0 ± 10,4 |
| 72,75 ± 6,7 |
| 65,4 ± 8,6 |
| 76,5 ± 2,1 |
| - |
|
|
| 2. CRP (> 6 mg/L) | 2 | 0.45 | 4 | 1.0 | 2 | 3,67 | 2 | 0.5 | 2 | 0 | 0 | 0 | 0.03 |
| 3. NT-proBNP (≥300 pq/ml) | 4 | 0.91 | 2 | 2.33 | 0 |
| 4 | 2.0 | 2 | 0 | 0 | 0 | 0.77 |
| 4.Reduced muscle mass | 5 | 2,29 | 2 | 0 | 0 |
| - |
| - |
| - |
| 0.12 |
Note: * L1 – mild frailty; L2 – moderate frailty; L3 – severe frailty; OR – odds ratio; p – statistical significance value (p < 0.05 considered significant); “Sarc” – severe sarcopenia according to EWGSOP2 criteria. Chi-square test was used and the Odds Ratio (OR) with 95% Confidence Intervals (CI) was calculated to evaluate risk factors | |||||||||||||
Cardiovascular risk factors were analyzed across the study groups. Physical activity of at least 30 minutes per day was reported by 62.9% of patients in G1, 25.0% in G2, and 20.0% in G3, suggesting a significant association between hypodynamia and frailty (adjusted OR = 2.52; 95% CI: 1.07-5.95; p = 0.016). Dyslipidemia was diagnosed in 44.4% of G1 patients, 16.7% of G2, and none in G3, supporting a potential inverse association between dyslipidemia and advanced frailty stages (adjusted OR = 0.34; 95% CI: 0.09-1.28; p = 0.019). Diabetes mellitus was most prevalent in G3 (40.0%), followed by G2 (33.3%) and G1 (18.5%). Obesity was distributed across all groups, with the highest frequency in G3 (80.0%), then G2 (66.7%) and G1 (55.5%). Sleep deprivation (≤5 hours/night) was reported in 40.7% of G1, 66.7% of G2, and 80.0% of G3 patients (p = 0.022). High comorbidity burden (Charlson Index ≥5) was noted in 63.0% of G1, 83.3% of G2, and 60.0% of G3 patients. Hospitalization frequency increased with frailty severity: ≥1 hospitalization/year was recorded in 41.1% of G1, 66.7% of G2, and 80.0% of G3.
NT-proBNP elevation was found in 85.1% of G1, 83.3% of G2, and 80.0% of G3. Low creatine kinase (CK) levels were noted in 85.2% of G1, 91.6% of G2, and 80.0% of G3. Elevated CRP was observed in G3 (60.0%), G2 (50.0%), and G1 (18.5%) (p = 0.039).
Atrial fibrillation was more common in G3 (80.0%), followed by G1 (55.5%) and G2 (50.0%). HFrEF was more frequent in G1 (48.1%), while HFpEF predominated in G2 (50.0%) and G3 (60.0%).
Metformin was used by 6.8% of G1, 9.1% of G2, and 6.8% of G3 patients (p = 0.008). Statin use was more common in G1 (69.0%) than in G2 (24.1%) or G3 (6.9%).
Sarcopenia risk (SARC-Calf ≥4) was identified in 48.1% of G1, 66.7% of G2, and 80.0% of G3. Severe sarcopenia occurred in 18.5% of G1 and 16.7% of G2 (OR = 4.11; p = 0.048), all in women. Mean age of sarcopenic patients was lower in G1 (65.4 ± 8.6 years) than in G2 (76.5 ± 2.1 years).
Hypertension was present in 48.1% (G1), 66.7% (G2), and 80.0% (G3) of sarcopenic patients. Obesity and diabetes were also more common in advanced frailty. Dyslipidemia was found in G1 and G2, but was absent in G3. All sarcopenic patients were non-smokers.
Reduced muscle strength was recorded in 51.8% (G1), 75.0% (G2), and 80.0% (G3). Physical performance impairment was present in 88.9% (G1), 91.7% (G2), and 100% (G3). Reduced calf circumference was seen in G1 (29.6%) and G2 (16.7%).
Elevated CRP (>6 mg/L) was more frequent in G2 (33.3%) and G3 (40.0%) than in G1 (7.4%) (adjusted OR = 3.67; 95% CI: 0.5–26.81; p = 0.039). Increased NT-proBNP levels associated with sarcopenia risk were noted in G1 (14.8%) and G2 (16.7%).
Metformin appeared protective in G1 (no sarcopenia cases) versus G2 (25.0%) and G3 (60.0%) (adjusted OR = 102.0; 95% CI: 3.7-2810; p = 0.008). Statin therapy was associated with a higher risk of sarcopenia in G1 (40.7%), G2 (33.3%) and G3 (40.0%).
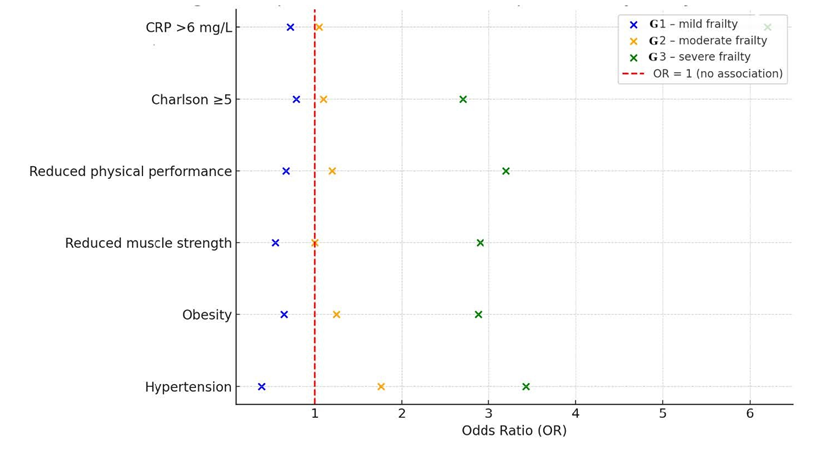
The comparative analysis of OR values for risk factors by frailty severity is presented in Fig. 1.
|
Fig. 1 Comparative analysis of Odds Ratio (OR) values for sarcopenia risk according to frailty severity: mild (G1), moderate (G2), severe (G3). (Each point represents the effect value estimated for a specific parameter. The vertical red line marks the reference threshold (OR = 1), indicating no association. Parameters with OR values >1 suggest a positive association with sarcopenia risk, while subunitary ORs may indicate a protective role or inverse association). |
Subsequently, the analysis focused on clinically confirmed sarcopenia, based on the three clinical and instrumental criteria recommended by EWGSOP2.
An association between arterial hypertension and confirmed sarcopenia was observed in G1 - 5 (18.5%) cases (OR = 1.70; 95% CI: 0.29-9.97), G2 - 2 (16.7%) (OR = 1.08; 95% CI: 0.18-6.49), and no cases in G3 (0%), which may indicate a potential role of hypertension in the development of sarcopenia among frail patients. Dyslipidemia was associated with sarcopenia exclusively in G1 – 1 (3.7%) case, representing an atypical finding, possibly influenced by underlying metabolic factors or lipid-lowering therapy. Diabetes mellitus was identified in four sarcopenic patients, with higher prevalence in G2 – 2 (16.7%) cases, compared to G1 – 2 (7.4%) cases. Physical activity analysis among sarcopenic patients revealed reduced activity in G1 – 2 (7.4%) and G2 – 2 (16.7%) cases, suggesting that functional decline may be an early clinical marker of sarcopenia (adjusted OR = 3.75; 95% CI: 0.45-30.91; p = 0.016).
Elevated C-reactive protein (CRP) levels were observed in G1 – 2 (7.4%) and G2 – 2 (16.7%) sarcopenic patients, with no cases recorded in G3, supporting the hypothesis of early systemic inflammation involvement in sarcopenia pathogenesis (adjusted OR = 2.75; 95% CI: 0.33-22.92; p = 0.039). Increased NT-proBNP levels were reported in G1 – 4 (14.8%) and G2 – 2 (16.7%) sarcopenic patients, but were absent in G3, reinforcing the link between cardiac dysfunction and muscle mass decline.
Metformin use was reported in 5 (18.5%) patients in G1 and 2 (16.7%) patients in G2, supporting a potential protective effect of this drug on skeletal muscle (adjusted OR = 1.35; 95% CI: 0.22-8.33; p = 0.008). Statin use among sarcopenic patients was documented in G1 – 4 (14.8%) cases, with no such cases in G2 or G3, suggesting a possible link between statin therapy and early muscular impairment.
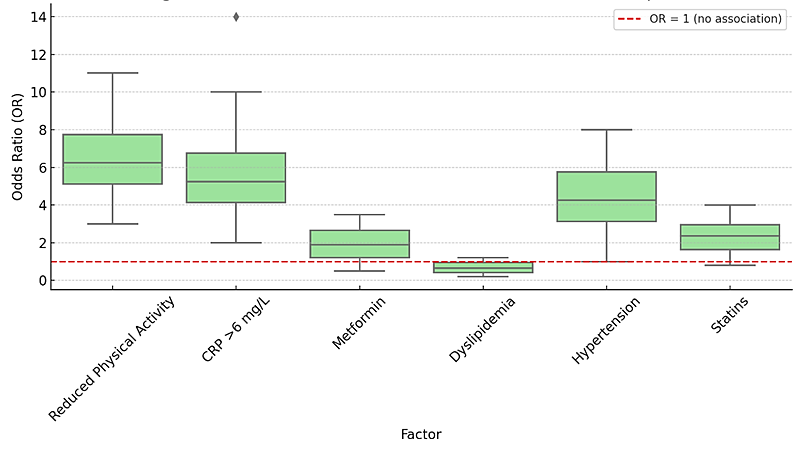
The estimated distribution of effect sizes associated with severe sarcopenia, based on the conducted analysis, is illustrated in Fig. 2.
|
Fig. 2 Distribution of effect estimates for factors associated with severe sarcopenia (Reduced physical activity and elevated CRP levels (>6 mg/L) exhibited median OR values above the reference threshold, supporting a positive association with sarcopenia. In contrast, dyslipidemia showed subunitary values, suggesting a potential inverse relationship). |
Discussion
The frailty syndrome represents an emerging paradigm in cardiology, increasingly recognized for its major clinical impact. Defined as a state of high vulnerability and diminished homeostatic reserves, frailty reflects not only biological aging but also multisystem dysfunction that affects patient autonomy. As opposed to chronological age, frailty has proven to be a more accurate predictor of severe complications, increased morbidity and mortality in chronic diseases. In patients with CHF, frailty plays a crucial role, influencing both prognosis and therapeutic decision-making. Literature data highlight the association between frailty and higher hospitalization rates, more frequent decompensations and increased mortality risk among CHF patients [8].
Sarcopenia, characterized by the loss of muscle mass and strength, is closely linked to frailty and contributes to the worsening functional status of patients with CHF. In our study, severe sarcopenia was identified in 15.9% of frail CHF patients, aligning with existing literature data where reported prevalence ranges between 10% and 34%, depending on the population, diagnostic criteria and assessment methods used. The exclusive presence of sarcopenia among women, predominantly in mild and moderate frailty stages, supports current data about a higher vulnerability of elderly women in the context of cardiovascular disease [9].
A significant association between sarcopenia and systemic inflammation markers, particularly C-reactive protein (CRP > 6 mg/L in 100% of cases, p = 0.039) was observed. This finding is consistent with multiple studies in which chronic inflammation was identified as a central mechanism in the pathogenesis of both sarcopenia and frailty in CHF patients, through impairment of muscle metabolism and mitochondrial dysfunction. Moreover, elevated NT-proBNP levels (≥300 pg/mL in 85.7% of sarcopenic cases) confirm the link between cardiac dysfunction severity and muscle wasting, as previously demonstrated in cohorts such as FRAGILE-HF [10-12].
The high prevalence of hypertension (71.4%), diabetes mellitus (57.1%) and obesity (42.8%) among patients with sarcopenia reflects current research findings on the interplay between metabolic syndrome components and muscle deterioration in CHF. A notable result of this study is the complete absence of sarcopenia among patients treated with metformin (p = 0.008), suggesting a potential protective effect. Similar findings have been reported in NHANES observational studies, in which metformin use was associated with increased muscle strength and reduced sarcopenia risk in diabetic patients, possibly due to indirect anti-inflammatory mechanisms [13]. Statin use was more frequent among patients with sarcopenia (57.1%). Although this association did not reach statistical significance (p = 0.075), recent data suggest a possible link between lipid-lowering therapy and early muscle decline in frail individuals [14].
These results support the importance of early functional screening for sarcopenia in frail CHF patients. Simple tools such as the SARC-Calf questionnaire, the Timed Up and Go test (TUG), and calf circumference measurement may be effectively used in clinical practice to identify at-risk patients and enable early, targeted interventions, both pharmacological and functional, to reduce the risks of decompensation, disability, and mortality in this population.
Conclusions
More than half of frail patients with chronic heart failure are at risk of developing sarcopenia (56.8%), while severe sarcopenia was confirmed in 15.9%, predominantly among women with frailty syndrome. Elevated NT-proBNP and CRP levels in sarcopenic patients highlight the central role of cardiac dysfunction and systemic inflammation in the pathogenesis of sarcopenia. Early screening for sarcopenia, along with optimal management of hypertension, diabetes and obesity is essential for the prevention and clinical management of sarcopenia in frail women with chronic heart failure.
Competing interests
None declared.
Authors’ contributions
AI conceived the study, performed data collection and analysis. LMN contributed to critical manuscript revision. VS provided methodological support and assisted in interpretation of parameters. LG supervised data analysis and contributed to the clinical interpretation of findings. SV coordinated study design and data interpretation, drafted the manuscript and critically reviewed it for intellectual content. All authors read and approved the final version of the manuscript.
Ethics approval
The study protocol was approved by the Research Ethics Committee of the Nicolae Testemițanu State University of Medicine and Pharmacy (minutes no. 48, issued on 23 May 2024).
Patient consent
Obtained.
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer reviewed.
Authors’ ORCID IDs
Anastasia Ivanes – https://orcid.org/0009-0008-5964-9003
Lucia Mazur-Nicorici – https://orcid.org/0000-0003-3983-8292
Virginia Șalaru – https://orcid.org/0000-0003-2683-6917
Livi Grib – https://orcid.org/0000-0001-6913-0864
Snejana Vetrilă – https://orcid.org/0000-0003-0834-8901
References
Vetrilă S, Grib L, Ivanes A. The pattern of the frailty syndrome in chronic heart failure. Ro J Med Pract. 2023;18(2):59-65. doi: 10.37897/RJMP.2023.2.2.
Kitamura A, Seino S, Abe T, Nofuji Y, Yokoyama Y, Amano H, Nishi M, Taniguchi Y, Narita M, Fujiwara Y, Shinkai S. Sarcopenia: prevalence, associated factors, and the risk of mortality and disability in Japanese older adults. J Cachexia Sarcopenia Muscle. 2021 Feb;12(1):30-38. doi: 10.1002/jcsm.12651.
Liu Y, Su M, Lei Y, Tian J, Zhang L, Xu D. Sarcopenia predicts adverse prognosis in patients with heart failure: a systematic review and meta-analysis. Rev Cardiovasc Med. 2023;24(9):273. doi: 10.31083/j.rcm2409273.
Boshnjaku A, Krasniqi E. Diagnosing sarcopenia in clinical practice: international guidelines vs. population-specific cutoff criteria. Front Med (Lausanne). 2024;11:1405438. doi: 10.3389/fmed.2024.1405438.
Kim HJ, Kim JY, Kim SH. Performance of calf circumference in identifying sarcopenia in older patients with chronic low back pain: a retrospective cross-sectional study. BMC Geriatr. 2024;24(1):674. doi: 10.1186/s12877-024-05263-z.
Voulgaridou G, Tyrovolas S, Detopoulou P, Tsoumana D, Drakaki M, Apostolou T, et al. Diagnostic criteria and measurement techniques of sarcopenia: a critical evaluation of the up-to-date evidence. Nutrients. 2024;16(3):436. doi: 10.3390/nu16030436.
Kiss CM, Bertschi D, Beerli N, Berres M, Kressig RW, Fischer AM. Calf circumference as a surrogate indicator for detecting low muscle mass in hospitalized geriatric patients. Aging Clin Exp Res. 2024;36(1):25. doi: 10.1007/s40520-024-02694-x.
Denfeld QE, Winters-Stone K, Mudd JO, Gelow JM, Kurdi S, Lee CS. The prevalence of frailty in heart failure: A systematic review and meta-analysis. Int J Cardiol. 2017 Jun 1;236:283-289. doi: 10.1016/j.ijcard.2017.01.153.
Marzetti E, Calvani R, Tosato M, Cesari M, Di Bari M, Cherubini A, Collamati A, D'Angelo E, Pahor M, Bernabei R, Landi F; SPRINTT Consortium. Sarcopenia: an overview. Aging Clin Exp Res. 2017 Feb;29(1):11-17. doi: 10.1007/s40520-016-0704-5.
Pothier K, Gana W, Bailly N, Fougère B. Associations between frailty and inflammation, physical, and psycho-social health in older adults: a systematic review. Front Psychol. 2022;13:805501. doi: 10.3389/fpsyg.2022.805501.
Sato R, Vatic M, da Fonseca GWP, von Haehling S. Sarcopenia and frailty in heart failure: is there a biomarker signature? Curr Heart Fail Rep. 2022 Dec;19(6):400-411. doi: 10.1007/s11897-022-00575-w.
Matsue Y, Kamiya K, Saito H, Saito K, Ogasahara Y, Maekawa E, et al. Prevalence and prognostic impact of the coexistence of multiple frailty domains in elderly patients with heart failure: the FRAGILE-HF cohort study. Eur J Heart Fail. 2020;22(11):2112-2119. doi: 10.1002/ejhf.1926.
Hu Y, Lu S, Xue C Hu Z, Wang Y, Zhang W, et al. Exploring the protective effect of metformin against sarcopenia: insights from cohort studies and genetics. J Transl Med. 2025;23(1):356. https://doi.org/10.1186/s12967-025-06357-x.
Huang ST, Otsuka R, Nishita Y, Meng LC, Hsiao FY, Shimokata H, et al. Risk of sarcopenia following long-term statin use in community-dwelling middle-aged and older adults in Japan. J Cachexia Sarcopenia Muscle. 2025;16(1):e13660. doi: 10.1002/jcsm.13660.