
Introduction
According to studies and research conducted since the beginning of 2025, this year marks a significant milestone in medical advancements across various disciplines, with notable progress in ophthalmology. A particular focus has been directed toward neurodegenerative ocular diseases. Stargardt disease, for instance, is caused by loss-of-function mutations in the ABCA4 gene, leading to progressive macular degeneration and eventual vision loss. As an incurable condition, it has posed a major therapeutic challenge. However, recent breakthroughs in 2025 have brought promising developments in gene therapy, particularly through the identification of novel therapeutic vectors capable of precisely editing ABCA4 mutations. These advancements pave the way for potential vision restoration and represent a critical step forward in the management of inherited retinal dystrophies [1].
Additional innovations published throughout the year have highlighted the role of gene therapy in the treatment of age-related macular degeneration (AMD). Notably, studies have demonstrated that a single gene therapy intervention targeting retinal pigment epithelium (RPE) cells can induce sustained production of anti-angiogenic proteins, offering a promising long-term strategy for controlling neovascularization in AMD [2].
AMD is one of the leading causes of vision loss globally among individuals over 50 years of age. This research is of significant importance, as AMD has emerged as a major public health concern. In 2020, approximately 10 million individuals were diagnosed with AMD, and current projections estimate that this number will double by 2040, emphasizing the urgent need for effective diagnostic and therapeutic strategies [3].
AMD is a polyetiological condition influenced by both modifiable and non-modifiable risk factors. According to recent studies, modifiable factors such as smoking, hypertension, diabetes mellitus, and cardiovascular diseases are significantly associated with an increased risk of AMD. Non-modifiable factors, including advanced age and male sex, also show a strong statistical correlation with disease onset. However, findings regarding body mass index (BMI), total cholesterol, and triglyceride levels remain controversial, as these variables have not demonstrated statistically significant associations [4, 5].
According to the latest research, AMD is classified into several stages: subclinical AMD, characterized by the absence of retinal pigment epithelium (RPE) depigmentation and the presence of small drusen; early AMD, which involves small to medium drusen, focal depigmentation, and impaired dark adaptation; intermediate AMD, associated with the accumulation of large drusen and more pronounced RPE changes; and advanced AMD, which is currently divided into two forms: dry AMD, also known as geographic atrophy (GA), and wet AMD, referred to as choroidal neovascularization (CNV) [6-8].
Currently, omics-based approaches – particularly the metabolomic one – are increasingly applied in the study of AMD, with a focus on the early detection of the disease through specific biomarkers and the development of personalized therapeutic targets tailored to the individual pathophysiological profile of each patient. In parallel, efforts are being made to implement efficient and early screening strategies by integrating artificial intelligence (AI) technologies into diagnostic workflows [9].
The scientific relevance of this work also lies in its analysis of existing therapeutic approaches for AMD, particularly its advanced wet form, which is associated with severe, often irreversible, vision loss. While anti-VEGF agents remain the standard of care, recent advancements have introduced complement system inhibition therapies targeting components such as C3 (pegcetacoplan) and C5 (avacincaptad pegol), the latter approved by the U.S. Food and Drug Administration in 2023 [10]. However, these treatments remain insufficient for achieving definitive disease control, and there is still no effective pharmacological therapy available for the dry (atrophic) form of AMD.
To elucidate the etiopathogenesis of AMD, enable early diagnosis through biomarkers, and identify innovative therapeutic targets, the application of omics-based approaches, particularly metabolomics and proteomics, has proven essential. Metabolomics involves the comprehensive analysis of low-molecular-weight metabolites (typically < 1500 Da), while proteomics focuses on the study of proteins involved in biochemical reactions, cellular processes, and metabolic pathways [4]. Together, these approaches provide powerful tools for the quantitative and qualitative assessment of specific biomarkers, offering insights into the pathogenetic mechanisms underlying AMD and supporting the development of targeted, personalized interventions.
The aim of this study was to identify characteristic biomarkers in patients diagnosed with age-related macular degeneration and to interpret their alterations.
Material and methods
The research was based on a pilot retrospective study involving the analysis of 80 medical records of patients admitted to the Ophthalmology Department of the "Timofei Moșneaga" Republican Clinical Hospital between 2019 and 2023. Among the 80 patients diagnosed with age-related macular degeneration (AMD), 42 were men (52.5%) and 38 were women (47.5%), with a mean age of 71.21 ± 8.81 years. Relevant data, including metabolic indices and biomarkers, were analyzed using SPSS version 23 (Statistical Package for the Social Sciences) for Windows XP. To assess statistical correlations with AMD, binomial tests, Wilcoxon Signed-Rank tests, and One-sample tests were applied.
The data obtained were compared with the results of a comprehensive analysis of the latest scientific literature on AMD. A systematic search of PubMed, MEDLINE, Web of Science, and Google Scholar was conducted to identify relevant studies published in English up to June 2025. Keywords included "age-related macular degeneration," "retinal degeneration," "metabolomics," "proteomics," "biomarkers," "oxidative stress," and "lipid metabolism."
Inclusion criteria were original research articles, reviews, and meta-analyses focusing on the AMD pathobiochemical mechanisms of ocular damage and potential marker identification by omics approaches. Data extraction and quality assessment were performed independently by two reviewers.
Results
Among the most researched etiopathogenetic mechanisms of AMD are oxidative stress (OS), nitrosative stress (NS), the complement system, lipid peroxidation (LPO), mitophagy, and mitochondrial DNA disorders [7].
The retina functions as a highly active metabolic center, with a substantial daily oxygen demand. However, exposure to various risk factors, such as psychological stress, aging, smoking, sleep deprivation, poor hygiene, and a nutritionally inadequate diet, can disturb the equilibrium between the antioxidant defense system and OS. This imbalance leads to the accumulation of reactive oxygen species (ROS), which cause oxidative damage at the level of the RPE, disrupt retinal metabolism, and contribute to progressive degeneration [9].
Additionally, with aging, lipofuscin (LF) – a cytotoxic and phototoxic component – accumulates. It contributes to the activation of drusogenesis and, upon exposure to blue light, has the property of releasing H2O2 and O2- (superoxide anion radical). Transformed into N-retinylidene-N-retinylethanolamine (A2E), it influences homeostasis and interferes with cholesterol metabolism by inducing OS, accompanied by LPO [11-13].
The hyperoxidative state within LPO initiates a vicious circle, which consequently damages DNA, proteins, and lipids, disrupting cellular functionality, survival, and proliferation, and additionally favoring the accumulation of LF [7].
Microvascular dysfunction is also involved in the deterioration of RPE function, leading to the dysregulation of nutrition and vascularization, setting up ischemia and activating angiogenesis by increasing the production of vascular endothelial growth factor (VEGF). Additionally, OS and vascular inflammation are associated, which worsen visual deficiencies, leading to pathological neovascularization, vascular damage, and disruption of the blood-retinal barrier.
Excessive production of ROS impairs the activation capacity of the antioxidant defense system and limits its ability to undergo repair. Consequently, this dysfunction leads to an energy crisis, primarily driven by damage to mitochondrial DNA [14, 15].
OS is one of the main causes of degeneration. Through pathological changes produced at the DNA level, it causes the activation of the STING (Stimulator of Interferon Genes) pathway, a cell signaling pathway located at the endoplasmic reticulum, which plays a role in detecting cytoplasmic/foreign DNA. This activation promotes chronic inflammation and, ultimately, the degeneration of RPE cells [16].
Moreover, OS triggers the activation of the PINK1/Parkin-mediated mitophagy pathway, leading to damage of the outer blood-retinal barrier. This impairment contributes to reduced choriocapillaris perfusion, resulting in ischemia and increased expression of VEGF. These events, in turn, activate the p62/Nrf2 signaling pathway, promoting dysregulated mitophagy and accumulation of dysfunctional mitochondria, thereby disrupting cellular homeostasis. Concurrently, the accumulation of PINK1 on the outer mitochondrial membrane and the subsequent recruitment of Parkin initiate the degradation of impaired mitochondria [17-19].
Similar to oxidative stress, nitrosative stress also contributes to the development of AMD through the release of peroxynitrite ‒ a cytotoxic byproduct of nitric oxide (NO) dysregulation. This leads to disturbances in choroidal microcirculation and degeneration of the retinal pigment epithelium (RPE), ultimately promoting neovascularization via upregulation of vascular endothelial growth factor (VEGF) synthesis [20].
The enhanced risk of developing degeneration is also marked by aberrant activation of the complement system, with the alternative pathway being the primary one involved. These processes lead to the dysregulation of cellular turnover. This hypothesis was supported by research on donor eyes, where the presence of C3b deposits and membrane attack complex (MAC) accumulations in the choriocapillaris and RPE was confirmed, and components of this system were detected within drusen structures [21].
Along with etiopathogenetic mechanisms, significant changes are also observed at the level of cellular metabolism. Approximately 80%-89% of metabolic alterations involve lipids, for which the following biomarkers are characteristic: total cholesterol, HDL-cholesterol, LDL-cholesterol, triglycerides, ApoA1, and ApoB. Very low-density lipoproteins (VLDL) show reduced values, in contrast to HDL, whose levels are elevated [22]. In the literature, increased activity of the complement system alongside reduced cholesterol level and a quantitative reduction of glycerophospholipids, which promotes the risk of developing AMD as well as other degenerative pathologies. Some epidemiological studies have concluded that increased HDL levels and reduced triglycerides (TAG) are more characteristic of patients diagnosed with AMD [23-25].
In addition to changes in lipid metabolism, there are also changes in amino acid metabolism. Thee EF et al. (2023), in the conducted studies, concluded that the following amino acids had lower levels: histidine, citrate, alanine, phenylalanine, tyrosine, leucine, and valine, and, conversely, the ketone bodies, acetoacetate and 3-hydroxybutyrate, were elevated [22]. Also, hyperhomocysteinemia considerably increases the risk of AMD development via the inflammatory processes caused, OS, cell apoptosis, and epigenetic changes, which lead to degeneration [26]. Additionally, it increases the level of glutamate, which induces neurotoxicity, promoting mitochondrial dysfunction and OS, resulting in cell death [27]. Mitochondrial dysfunction has also been found in the case of disorders of alanine, glycine, and serine metabolism [28].
As previously mentioned, the retina is an active metabolic center, and relies on glucose as an energy substrate, meaning that glucose metabolism cannot be overlooked in the case of AMD. Thus, the following changes in glucose metabolism have been observed: elevation of citrate and isocitrate, and a decrease in succinate, glutamine, and α-ketoglutarate, which promote the secretion of VEGF, responsible for macular neovascularization in AMD [29]. Hyperglycemia promotes the accumulation of advanced glycation end products (AGEs) which in turn trigger OS and pro-inflammatory pathways, ultimately leading to RPE dysfunction. At the same time, hyperglycemia stimulates VEGF expression and favors the development of the wet form of AMD [30].
Although there are multiple and varied controversies regarding the disorders detected in hemostatic metabolism, researchers support the idea that elevated fibrinogen concentrations may increase the risk of developing AMD, particularly its wet form. A few studies suggest that plasminogen activator inhibitor-1 is correlated with the occurrence of AMD. However, due to disputes in this area, the factors involved in hemostatic metabolism cannot yet be considered potential biomarkers for AMD [31].
In this study, the pilot retrospective analysis was considered relevant for comparing the data obtained from a selected patient cohort with findings reported in clinical studies. The investigation involved the review and evaluation of 80 medical records of patients admitted to the Ophthalmology Department of the "Timofei Moșneaga" Republican Clinical Hospital between 2019 and 2023. All patients included in the study were diagnosed with AMD, comprising 42 males (52.5%) and 38 females (47.5%), with a mean age of 71.21 ± 8.81 years. Relevant available data were extracted from the patients’ medical records, including age, sex, laboratory indices, primary diagnosis, and comorbidities. These variables were analyzed using binomial tests, One-sample tests, and Wilcoxon Signed-Rank tests in SPSS to determine their statistically significant correlations with AMD. The binomial test, One-sample test, and Wilcoxon Signed-Rank test were applied to assess the statistical significance of categorical and continuous variables, allowing for the comparison of observed data with theoretical or clinical reference values, particularly where normal distribution could not be assumed.
Application of the binomial test identified the presence of statistically significant biomarkers with values of p<0.05, as outlined below: glucose (p=0.022); prothrombin (p<0.001); fibrinogen (p<0.001); triglycerides (p=0.031); platelet count (p=0.000); leukocyte count (p<0.001); and ESR (p=0.017). Statistically insignificant were the values of INR (p=0.203), total cholesterol (p=0.458), HDL-cholesterol (p=1.000), LDL-cholesterol (p=0.289), and lymphocyte count (p=0.110) (Table 1).
Table 1. Results obtained from the analysis of various biomarkers using the binomial and Wilcoxon Signed-Rank tests. | ||
Parameter | Binomial test | Wilcoxon Signed-Rank test |
Glucose | p<0.022 * | p=0.004 ** |
Prothrombin | p<0.001 *** | p=<0.001 *** |
Fibrinogen | p<0.001 *** | p<0.001 *** |
INR | p=0.203 ns | p<0.001 *** |
Triglycerides | p=0.031 * | p=0.009 ** |
Total cholesterol | p=0.458 ns | p=0.041 * |
HDL-cholesterol | p=1.000 ns | p=0.541 ns |
LDL-cholesterol | p=0.289 ns | p=0.208 ns |
Platelet count | p=<0.001 *** | p<0.001 *** |
Leukocyte count | p<0.001 *** | p<0.001 *** |
Lymphocyte count | p=0.110 ns | p=0.003 ** |
ESR | p=0.017 * | p=0.309 ns |
Note: Statistical significance compared to the control group: * − p < 0,05; ** − p < 0.01; *** − p < 0.001; ns – not significant. ESR – erythrocyte sedimentation rate; INR – international normalized ratio. | ||
Compared to the results of the Wilcoxon Signed-Rank test, some discrepancies were observed. Statistically significant laboratory indices in this test included fibrinogen, prothrombin, INR, platelet count, and leukocyte count, all with p-values < 0.001. Total cholesterol was also significant with p=0.041, though close to the significance threshold. Additionally, triglycerides (p=0.009), glucose (p=0.004), and lymphocyte count (p=0.003) showed statistical significance. The biomarkers found to be statistically insignificant in this test were ESR (p=0.309), HDL-cholesterol (p=0.541), and LDL-cholesterol (p=0.208) (Table 1).
These deviations may be due to study limitations, such as the relatively small number of patients involved, given that the pathology is not very common in the Republic of Moldova, incomplete laboratory data, lacunar diagnosis, and the lack of stratification according to the wet or dry form of AMD.
Another test used to investigate biomarkers associated with AMD is the One-sample test (Fig. 1). Regarding this test, it was observed that glucose has a lower mean value of 1.7053 and an upper mean of -0.2755, indicating asymmetry in the data and suggesting that it is statistically significant, thus showing a moderate but meaningful deviation. Prothrombin has a lower mean value of 22.0073 and an upper mean of -37.5641, both significant as they lie outside the reference range, indicating major deviations from the mean. For fibrinogen, the lower mean is 1.2843 (positive), and the upper mean is -0.7249 (negative); these data suggest asymmetry and a potential imbalance in data distribution. Additionally, deviations were noted for ESR, with a lower mean of 11.3533 and an upper mean of -0.3133, not necessarily significant on both sides, indicating slight asymmetry. A comparable pattern was observed for triglycerides, with a lower mean of 1.3061 and an upper mean of -0.4189, suggesting a slight deviation from reference values. In this test, insignificant deviations were found for total cholesterol and LDL-cholesterol, as presented in Fig.1.
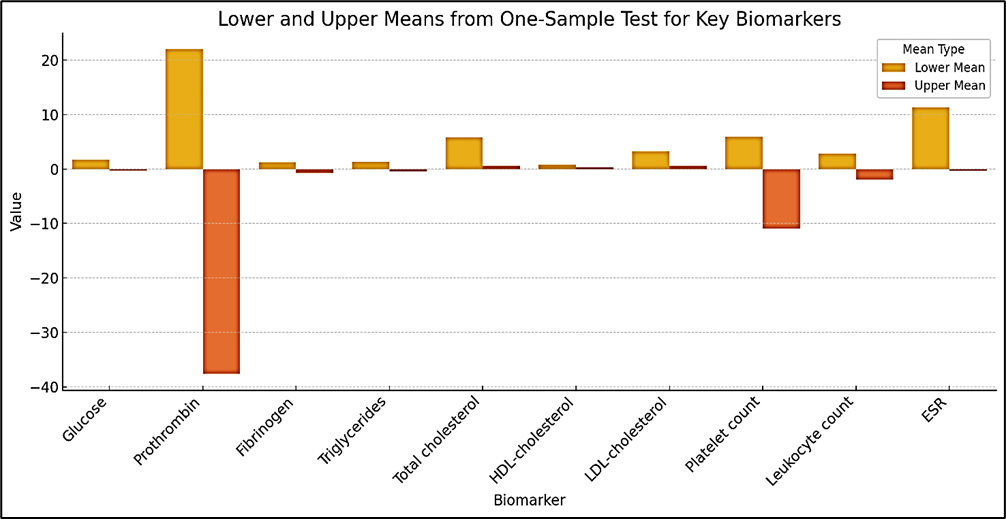 |
Fig. 1 Lower and upper mean estimates of key biomarkers in AMD patients as identified by the One-sample test Note: a) Data are expressed as estimated mean differences. b) The One-sample test was used to assess whether the sample mean significantly deviates from the clinical reference value for each biomarker. Positive or negative mean values indicate the direction and magnitude of deviation from the reference mean. c) ESR – erythrocyte sedimentation rate. |
As a result of the comprehensive investigation of the obtained data, we can conclude that acquired biomarkers can be divided into 3 categories: statistically significant biomarkers, dual biomarkers, and statistically insignificant biomarkers.
Among the statistically significant biomarkers are glucose, triglycerides, prothrombin, fibrinogen, platelet count, and leukocyte count. These data confirm the involvement of glucose and lipid metabolism disorders–represented by triglycerides–in the etiopathogenesis of AMD; hemostatic metabolism imbalances, evidenced by changes in fibrinogen and prothrombin levels, indicating possible coagulation disorders along with platelet count; and last but not least, systemic inflammatory process, chronically represented by leukocyte count, which suggest an association with the risk of progression of macular lesions. These biomarkers thus become pathognomonic factors for AMD.
Among the dual biomarkers are total cholesterol, ESR, and lymphocyte count. ESR is statistically significant in the binomial test (p=0.017) and the One-sample test but is insignificant in Wilcoxon Signed-Rank test (p=0.309), likely due to differences in sensitivity to data distribution. Total cholesterol is insignificant (p=0.458) in the binomial test and significant, but close to the threshold (p=0.041) in Wilcoxon Signed-Rank test, indicating unclear deviations from the proportion. Additionally, lymphocyte count is insignificant (p=0.110) in the binomial test, but significant (p=0.003) in Wilcoxon Signed-Rank test, suggesting that the proportion does not differ from the clinical reference range, while the median level shows discrepancies.
Representatives of the subgroup of statistically insignificant biomarkers are HDL-cholesterol, LDL-cholesterol, and INR. Despite studies indicating the active involvement of hyperlipidemia in the etiopathogenesis of the disease and vascular risk at the ocular level, in the studied population we observe the opposite. The possible reason is that these biomarkers are not directly correlated with AMD.
Thus, to minimize the discrepancies observed in the study, it is necessary to apply several statistical methods to avoid presenting erroneous data. At the same time, we conclude that the study detected significant biomarkers correlated with AMD, such as glucose, triglycerides, and fibrinogen, indicating that these indices could be promising for assessing AMD risk, as they are associated with metabolic and inflammatory disorders specific to degeneration. However, to confirm these results, paraclinical imaging data of the patients involved in the study are also necessary, in particular those obtained by optical coherence tomography, as well as their medical history (diabetes mellitus, hypertension).
Discussions
In recent years, degeneration has gained momentum practically on all continents, with research demonstrating inevitable, progressive, and irreversible damage to the visual system, resulting in an unfavorable prognosis for this pathology.
As a result of this study, as well as those researched in scientific databases, we conclude the importance of modifiable and non-modifiable risk factors, environmental influences, lifestyle, and genetic factors in the evolution and manifestation of degeneration. These data are necessary for identifying potential effective therapeutic targets. We have presented their impact on health and the devastating consequences that lead to disability [5].
The burden imposed by this condition on individual health and societal systems has led the medical community to recognize AMD as a public health priority, for which early diagnosis and effective treatment are critically needed [3].
The integration of omics technologies, particularly metabolomics and proteomics, has significantly advanced our understanding of AMD pathogenesis. Metabolomics enables the identification of small-molecule metabolic signatures associated with disease progression, while proteomics allows characterization of changes in protein expression, structure, and interactions within retinal tissues. These approaches have uncovered new biomarkers and potential therapeutic targets, emphasizing their importance in both early diagnosis and personalized medicine strategies for AMD [4].
After understanding the etiopathogenetic mechanisms of AMD, researchers have identified that restoring the compromised antioxidant system can be achieved through supplementation with exogenous antioxidants, such as β-carotene, vitamins C and E, copper, and zinc. The consumption of these antioxidants results in approximately a 25% decrease in the progression of the neovascular form of AMD over 5 years. Additionally, administration of lutein and zeaxanthin reduces the risk of progression to late AMD. Furthermore, consumption of acetyl L-carnitine, ω-3 fatty acids, and coenzyme Q10 has demonstrated considerable improvement in visual function in patients diagnosed with AMD [32].
Future research directions focus on gene and cell therapy, AI, and the development of targeted, individualized treatments aimed at monitoring, exploring, and managing the disease. For example, one promising therapy is intravitreal gene therapy with ADVM-022, which enables continuous production of aflibercept in retinal cells through a single injection, effectively inhibiting neovascularization [33].
Anti-VEGF therapy remains the standard treatment for wet AMD but has limitations in cases with macular fibrosis and carries side effects, including treatment resistance. Additionally, complement system inhibitors (pegcetacoplan, avacincaptad pegol) have shown promising results in AMD therapy but pose a risk of intraocular inflammation, particularly in geographic atrophy cases [34].
Thus, the omics approach opens new perspectives for the identification of AMD biomarkers and the development of effective therapies, but further studies are needed to optimize treatments and prevent disease progression.
In conclusion, we support the idea that, as a result of this pilot retrospective study, we identified some omics-derived indices as potential biomarkers for AMD risk assessment and monitoring. However, given the complexity of this pathology, a multidisciplinary approach that includes targeted metabolomic and proteomic investigations is essential. Additionally, to reduce the limitations encountered during the study, it is recommended to increase the sample size and extend the spectrum of monitored and analyzed parameters to avoid deficiencies.
Conclusions
The study highlighted the involvement of several biomarkers in the pathogenesis and progression of age-related macular degeneration (AMD), particularly those related to lipid metabolism (e.g., total cholesterol, LDL-cholesterol, HDL-cholesterol, triglycerides, apolipoprotein B, apolipoprotein A1), glucose metabolism, and hemostatic imbalance (e.g., fibrinogen, prothrombin). Among these, our pilot retrospective study confirmed the statistical significance of glucose, triglycerides, fibrinogen, prothrombin, platelet count, and leukocyte count, supporting their potential role as biomarkers for AMD risk assessment and disease monitoring.
These findings suggest that omics-derived indices, particularly from metabolomics and proteomics, could help in identifying personalized diagnostic and therapeutic targets. However, further large-scale, stratified studies are required to validate these associations, integrate imaging findings, and address current limitations related to data completeness and AMD subtype differentiation.
Competing interests
None declared.
Authors’ contributions
EP and AU collected and analyzed the data and drafted the manuscript. AU and EP conceived the study, participated in study design, statistical analysis, and assisted in drafting the manuscript. SP and AA analyzed the data and critically revised the manuscript. OT critically evaluated the results, assessed their applicability, and critically revised the manuscript. All authors reviewed the work critically and approved the final version of the manuscript.
Informed consent for publication
Obtained.
Acknowledgements and funding
No external funding
Ethics approval
The study protocol was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (approval no. 58, dated June 20, 2024).
Provenance and peer review
Not commissioned, externally peer-reviewed.
Authors’ ORCID IDs
Ecaterina Pavlovschi – https://orcid.org/0000-0003-0385-4805
Angela Untila – https://orcid.org/0000-0002-3835-3341
Svetlana Protopop – https://orcid.org/0000-0003-1660-3343
Ala Ambros – https://orcid.org/0000-0001-8545-8501
Olga Tagadiuc – https://orcid.org/0000-0002-5503-8052
References
Muller A, Sullivan J, Schwarzer W, et al. High-efficiency base editing in the retina in primates and human tissues. Nat Med. 2025;31(2):490-501. doi: 10.1038/s41591-024-03422-8.
Hushmandi K, Lam HY, Wong WM, et al. Gene therapy for age-related macular degeneration: a promising frontier in vision preservation. Cell Commun Signal. 2025;23(1):233. doi: 10.1186/s12964-025-02246-4.
Thomas CJ, Mirza RG, Gill MK. Age-related macular degeneration. Med Clin North Am. 2021;105(3):473-491. doi: 10.1016/j.mcna.2021.01.003.
Laíns I, Gantner M, Murinello S, et al. Metabolomics in the study of retinal health and disease. Prog Retin Eye Res. 2019;69:57-79. doi: 10.1016/j.preteyeres.2018.11.002.
Babaker R, Alzimami L, Al Ameer A, et al. Risk factors for age-related macular degeneration: updated systematic review and meta-analysis. Medicine (Baltimore). 2025;104(8):e41599. doi: 10.1097/MD.0000000000041599.
Spaide RF, Jaffe GJ, Sarraf D, et al. Consensus Nomenclature for Reporting Neovascular Age-Related Macular Degeneration Data: Consensus on Neovascular Age-Related Macular Degeneration Nomenclature Study Group. Ophthalmology. 2020;127(5):616-636. doi: 10.1016/j.ophtha.2019.11.004. Eratum in: Ophthalmology 2020 Oct;127(10):1434-1435. doi: 10.1016/j.ophtha.2020.07.019.
Bondy S, Maiese K, editors. Aging and age-related disorders. New York: Humana Press; 2010. 472 p. doi: 10.1007/978-1-60761-602-3. (Oxidative stress in applied basic research and clinical practice).
Li X, Cai S, He Z, et al. Metabolomics in retinal diseases: an update. Biology (Basel). 2021;10(10):944. doi: 10.3390/biology10100944.
Deng Y, Qiao L, Du M, et al. Age-related macular degeneration: epidemiology, genetics, pathophysiology, diagnosis, and targeted therapy. Genes Dis. 2021;9(1):62-79. doi: 10.1016/j.gendis.2021.02.009.
Trincão-Marques J, Ayton LN, Hickey DG, et al. Gene and cell therapy for age-related macular degeneration: a review. Surv Ophthalmol. 2024;69(5):665-676. doi: 10.1016/j.survophthal.2024.05.002.
Pugazhendhi A, Hubbell M, Jairam P, Ambati B. Neovascular macular degeneration: a review of etiology, risk factors, and recent advances in research and therapy. Int J Mol Sci. 2021;22(3):1170. doi: 10.3390/ijms22031170.
Brown CN, Green BD, Thompson RB, den Hollander AI, Lengyel I; EYE-RISK consortium. Metabolomics and age-related macular degeneration. Metabolites. 2018;9(1):4. doi: 10.3390/metabo9010004.
Rajanala K, Dotiwala F, Upadhyay A. Geographic atrophy: pathophysiology and current therapeutic strategies. Front Ophthalmol (Lausanne). 2023;3:1327883. doi: 10.3389/fopht.2023.1327883.
Kaarniranta K, Uusitalo H, Blasiak J, et al. Mechanisms of mitochondrial dysfunction and their impact on age-related macular degeneration. Prog Retin Eye Res. 2020;79:100858. doi: 10.1016/j.preteyeres.2020.100858.
Hyttinen JMT, Blasiak J, Kaarniranta K. Non-coding RNAs regulating mitochondrial functions and the oxidative stress response as putative targets against age-related macular degeneration (AMD). Int J Mol Sci. 2023;24(3):2636. doi: 10.3390/ijms24032636.
Zou M, Ke Q, Nie Q, et al. Inhibition of cGAS-STING by JQ1 alleviates oxidative stress-induced retina inflammation and degeneration. Cell Death Differ. 2022;29(9):1816-1833. doi: 10.1038/s41418-022-00967-4.
Tisi A, Feligioni M, Passacantando M, Ciancaglini M, Maccarone R. The impact of oxidative stress on blood-retinal barrier physiology in age-related macular degeneration. Cells. 2021;10(1):64. doi: 10.3390/cells10010064.
Zhao B, Zhu L, Ye M, et al. Oxidative stress and epigenetics in ocular vascular aging: an updated review. Mol Med. 2023;29(1):28. doi: 10.1186/s10020-023-00624-7.
Zhang SM, Fan B, Li YL, Zuo ZY, Li GY. Oxidative stress-involved mitophagy of retinal pigment epithelium and retinal degenerative diseases. Cell Mol Neurobiol. 2023;43(7):3265-3276. doi: 10.1007/s10571-023-01383-z.
Toma C, De Cillà S, Palumbo A, Garhwal DP, Grossini E. Oxidative and nitrosative stress in age-related macular degeneration: a review of their role in different stages of disease. Antioxidants (Basel). 2021;10(5):653. doi: 10.3390/antiox10050653.
Maugeri A, Barchitta M, Mazzone MG, Giuliano F, Agodi A. Complement system and age-related macular degeneration: implications of gene-environment interaction for preventive and personalized medicine. Biomed Res Int. 2018;2018:7532507. doi: 10.1155/2018/7532507.
Thee EF, Acar İE, Colijn JM, et al. Systemic metabolomics in a framework of genetics and lifestyle in age-related macular degeneration. Metabolites. 2023;13(6):701. doi: 10.3390/metabo13060701.
Acar İE, Lores-Motta L, Colijn JM, et al. Integrating metabolomics, genomics, and disease pathways in age-related macular degeneration: the EYE-RISK Consortium. Ophthalmology. 2020;127(12):1693-1709. doi: 10.1016/j.ophtha.2020.06.020.
Lo Faro V. Answer to the Hamlet-like dilemma of lipid metabolites causing senile macular degeneration. Cell Rep Med. 2023;4(7):101077. doi: 10.1016/j.xcrm.2023.101077.
Tan LX, Germer CJ, La Cunza N, Lakkaraju A. Complement activation, lipid metabolism, and mitochondrial injury: converging pathways in age-related macular degeneration. Redox Biol. 2020;37:101781. doi: 10.1016/j.redox.2020.101781.
Tawfik A, Samra YA, Elsherbiny NM, Al-Shabrawey M. Implication of hyperhomocysteinemia in blood retinal barrier (BRB) dysfunction. Biomolecules. 2020;10(8):1119. doi: 10.3390/biom10081119.
Xia M, Zhang F. Amino acids metabolism in retinopathy: from clinical and basic research perspective. Metabolites. 2022;12(12):1244. doi: 10.3390/metabo12121244.
Mitchell SL, Ma C, Scott WK, et al. Plasma metabolomics of intermediate and neovascular age-related macular degeneration patients. Cells. 2021;10(11):3141. doi: 10.3390/cells10113141.
Han G, Wei P, He M, Teng H. Glucose metabolic characterization of human aqueous humor in relation to wet age-related macular degeneration. Invest Ophthalmol Vis Sci. 2020;61(3):49. doi: 10.1167/iovs.61.3.49.
Lee H, Han KD, Shin J. Association between glycemic status and age-related macular degeneration: a nationwide population-based cohort study. Diabetes Metab. 2023;49(3):101442. doi: 10.1016/j.diabet.2023.101442.
Kersten E, Paun CC, Schellevis RL, et al. Systemic and ocular fluid compounds as potential biomarkers in age-related macular degeneration. Surv Ophthalmol. 2018;63(1):9-39. doi: 10.1016/j.survophthal.2017.05.003.
Basyal D, Lee S, Kim HJ. Antioxidants and mechanistic insights for managing dry age-related macular degeneration. Antioxidants (Basel). 2024;13(5):568. doi: 10.3390/antiox13050568.
Blasiak J, Pawlowska E, Ciupińska J, Derwich M, Szczepanska J, Kaarniranta K. A new generation of gene therapies as the future of wet AMD treatment. Int J Mol Sci. 2024;25(4):2386. doi: 10.3390/ijms25042386.
Xu H, Yi C, Chen M. The complement pathway as a therapeutic target for neovascular age-related macular degeneration-mediated subretinal fibrosis. Curr Opin Pharmacol. 2024;76:102448. doi: 10.1016/j.coph.2024.102448.