

Introduction
Bronchopulmonary dysplasia (BPD) remains one of the most challenging complications of prematurity, affecting up to 40% of infants born before 28 weeks of gestation and associated with significant long-term morbidity [1]. Globally, prolonged premature rupture of membranes (PPROM) complicates approximately 2–3% of all pregnancies and up to 30% of preterm deliveries, while chorioamnionitis affects 10–25% of these cases. However, there are limited regional data from Eastern Europe, particularly Moldova, on how PPROM-related chorioamnionitis influences neonatal lung outcomes [1]. The pathogenesis of BPD is multifactorial, involving immaturity, oxygen toxicity, ventilator-induced trauma, and antenatal inflammation [2].
Prolonged premature rupture of membranes is a leading obstetric risk factor for intrauterine infection, allowing ascending microbial invasion and triggering an inflammatory cascade [3]. Chorioamnionitis, whether clinical or histological, has been associated with increased risk of neonatal sepsis, pulmonary hemorrhage, and chronic respiratory disease. However, its relationship with respiratory distress syndrome (RDS) and BPD remains complex: some studies suggest that antenatal inflammation accelerates surfactant production and reduces RDS, while others highlight its detrimental role in alveolar and vascular development, predisposing to BPD [4, 5]. This duality – where intrauterine inflammation may transiently enhance surfactant synthesis but also impair lung development – has been termed the chorioamnionitis paradox.
This study aimed to evaluate the relationship between PPROM, chorioamnionitis, and neonatal respiratory outcomes, particularly BPD and pulmonary hypertension (PH), in a cohort of preterm infants ≤34 weeks’ gestation in Moldova.
Materials and methods
We conducted a prospective cohort study including 108 preterm infants ≤34 weeks of gestation admitted to the Neonatal Intensive Care Unit (NICU) of the Mother and Child Institute, Chișinău, between October 2023 and July 2024. The study protocol was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (Approval No. 72, 28 October 2022). The representative study sample was calculated using the EpiInfo 7.2.2.6 software, “StatCalc – Sample Size and Power” module, for an analytical observational cohort study. With a 99.9% confidence interval, the study population was divided into two groups: the chorioamnionitis (CA) group included 54 preterm infants under 34 weeks of gestation born to mothers with chorioamnionitis, and the control group included 54 preterm infants under 34 weeks of gestation born to mothers without chorioamnionitis,
Inclusion criteria were: gestational age ≤34 weeks, inborn status (born in this hospital), and NICU admission. We excluded preterm newborns greater than 34 weeks of gestation, preterm newborns transferred from another hospital and those with congenital malformations incompatible with life.
For diagnoses of chorioamnionitis were used the criteria adopted from American College of Obstetricians and Gynecologists (ACOG) (2017) – maternal temperature greater than or equal to 39.0°C or when the maternal temperature of 38.0–38.9°C and at least one additional clinical risk factor is present [6]. Clinical risk factors included: maternal tachycardia (>100 beats per minute), fetal tachycardia (>160 beats per minute), uterine tenderness on palpation, the presence of purulent or foul-smelling amniotic fluid, maternal leukocytosis (>15,000/mm³ in the absence of corticosteroid therapy), PROM >18 hours. Histological chorioamnionitis was related to the presence of neutrophilic infiltration within the fetal membranes and umbilical cord.
The subjects were categorized based on gestational age and birth weight, as described in medical literature [7]. Gestational age classification included: (a) extremely preterm (<28 weeks), (b) very preterm (28–32 weeks), and (c) moderate preterm (32–34 weeks).
Clinical data were extracted from medical records and collected to an Excel database. These included demographic data, maternal risk factors (including PPROM), neonatal characteristics (gestational age, birth weight, Apgar scores), type and duration of respiratory support (CPAP, VAP, HFOV), and pulmonary complications (RDS, BPD, pulmonary haemorrhage, PH).
Analyzed maternal risk factors were history of preterm birth, abortions, stillbirths, amniotic sac infection, fever during labor, IUGR (Intrauterine growth restriction), oligohydramnios, PROM >18 hours, MSAF (Meconium-Stained Amniotic Fluid ), TORCH (Toxoplasmosis, Rubella, Cyto-megalovirus, Herpes simplex, and Other agents like syphilis or HIV), anemia, preeclampsia, c-section. BPD diagnosis was based on clinical and radiological criteria.
Obtained data were analyzed using Microsoft Excel statistical tools. Continuous variables were expressed as mean ± standard deviation (SD) and 95% confidence intervals. Categorical variables were summarized as frequencies and percentages. Associations between maternal risk factors, chorioamnionitis, and neonatal pulmonary outcomes were evaluated using the Pearson chi-square test. Effect sizes for chi-square associations were quantified using Cramér’s V. To examine the independent relationship between chorioamnionitis and respiratory complications such as BPD and PH, binary logistic regression was applied. Odds ratios (OR) and 95% confidence intervals (CI) were calculated. Examined confounders were gestational age and birth weight. Analyses were performed using the logistic regression module available in Microsoft Excel. No data were missing. A p-value <0.05 was considered statistically significant.
Results
A total of 108 preterm infants born at ≤34 weeks of gestation were included in the study, divided equally between the chorioamnionitis (CA) group (n = 54) and the control group (n = 54). The distribution by gestational age and sex was relatively uniform between the two groups, ensuring comparability. However, the CA group included a higher proportion of extremely preterm infants (<28 weeks) compared to controls (25.9% vs. 11.1%, p<0.05). The proportion of female infants was slightly higher in the control group (59.3% vs. 48.1%, not significant) (Table 1).
Table 1. Characteristics of the study population | |||||||
| CA | Control | Total | ||||
n (54) | % | n (54) | % | n (108) | % | ||
Term of gestation | <28 weeks | 14* | 25.9 | 6 | 11.1 | 20 | 18.5 |
28-32 weeks | 31 | 57.4 | 31 | 57.4 | 62 | 57.4 | |
>32 weeks | 9 | 16.7 | 17 | 31.5 | 26 | 24.1 | |
Gender | Female | 26 | 48.1 | 32 | 59.3 | 58 | 53.7 |
Male | 28 | 51.9 | 22 | 40.7 | 50 | 46.3 | |
Note: Data are expressed as number and percentage [n (%)]. Statistical comparison between groups was performed using the Chi-square test; p < 0.05 was considered significant (*). CA – chorioamnionitis; n – number of subjects. | |||||||
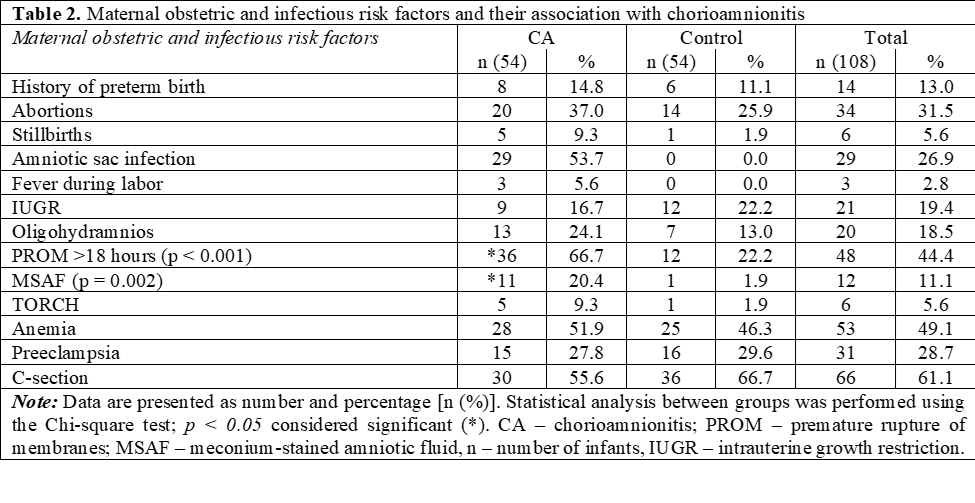
Analysis of maternal and obstetric characteristics revealed several significant differences between groups (Table 2). Prolonged premature rupture of membranes (PROM > 18 hours) was markedly more frequent among mothers with chorioamnionitis (66.7% vs. 22.2%, χ² = 21.6, p<0.001), confirming a strong association between PPROM and intrauterine infection. Meconium-stained amniotic fluid (MSAF) was also significantly more frequent in the CA group (20.4% vs. 1.9%, χ2 = 9.38, p = 0.002).
Although other maternal factors, including maternal history of preterm birth was more prevalent in the CA group (14,8% vs 11,1%), abortion (37.0% vs 25.9%), stillbirths (9.3% vs 1,9%), these differences were not statistically significant. The incidence of amniotic sac infection was notable in our population 26,9%, but statistical comparison was not possible as this finding was exclusive to the CA group. Also, maternal fever was observed in 5.6% of the CA group.
Infants born to mothers with chorioamnionitis demonstrated poorer adaptation at birth (Table 3). At 1 minute, 74.1% of CA-exposed infants had Apgar scores between 4–6, compared with 50.0% in controls, while only9.3% achieved scores ≥7 compared to42.6% in controls (p < 0.05). By 5 minutes, although most infants improved, 85.2% of the CA group had Apgar scores 7–8 vs 37.0% of controls, confirming delayed neonatal adaptation (p < 0.05).
Table 3. Apgar Score at 1 and 5 minutes of the subjects included in the study | |||||||
| CA | Control | Total | ||||
n (54) | % | n (54) | % | n (108) | % | ||
1 minute | 1-3 | 9 | 16.7 | 4 | 7.4 | 13 | 12.0 |
4-6 | *40 | 74.1 | 27 | 50.0 | 67 | 62.0 | |
7-8 | 5 | 9.3 | *23 | 42.6 | 28 | 25.9 | |
5 minutes | 1-3 | 0 | 0.0 | 3 | 5.6 | 3 | 2.8 |
4-6 | 8 | 14.8 | *31 | 57.4 | 39 | 36.1 | |
7-8 | *46 | 85.2 | 20 | 37.0 | 66 | 61.1 | |
Note: Data are presented as number and percentage [n (%)]. Statistical analysis was performed using the Chi-square test; p < 0.05 considered significant (*). CA – chorioamnionitis; n – number of infants. | |||||||
The need for respiratory support was universal among preterm infants but differed in intensity and duration between groups (Table 4). Infants in the CA group required significantly longer invasive ventilation (5.9 ± 10.6 days vs. 2.2 ± 4.8 days, p < 0.05) and had longer total hospital stays (32.6 ± 28.2 days vs. 25.0 ± 16.6 days). The duration of CPAP and HFOV use did not differ significantly, although a higher mean use was observed in the CA group.
These findings indicate that exposure to maternal infection was associated with more severe respiratory compromise and prolonged hospitalization.
Table 4. Days on respiratory support (HFOV, VAP, CPAP) | |||||||||
| n | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | ||
Lower Bound | Upper Bound | ||||||||
Days of hospital stay | CA | 54 | 32.59 | 28.200 | 3.838 | 24.90 | 40.29 | 1 | 162 |
Control | 54 | 24.98 | 16.609 | 2.260 | 20.45 | 29.51 | 3 | 70 | |
Total | 108 | 28.79 | 23.349 | 2.247 | 24.33 | 33.24 | 1 | 162 | |
HFOV (days) | CA | 54 | .37 | .917 | .125 | .12 | .62 | 0 | 4 |
Control | 54 | .22 | .664 | .090 | .04 | .40 | 0 | 3 | |
Total | 108 | .30 | .800 | .077 | .14 | .45 | 0 | 4 | |
VAP (days) | CA | 54 | *5.94 | 10.609 | 1.444 | 3.05 | 8.84 | 0 | 63 |
Control | 54 | 2.24 | 4.825 | .657 | .92 | 3.56 | 0 | 30 | |
Total | 108 | 4.09 | 8.411 | .809 | 2.49 | 5.70 | 0 | 63 | |
CPAP (days) | CA | 54 | 4.65 | 7.159 | .974 | 2.69 | 6.60 | 0 | 38 |
Control | 54 | 3.48 | 4.041 | .550 | 2.38 | 4.58 | 0 | 24 | |
Total | 108 | 4.06 | 5.815 | .560 | 2.96 | 5.17 | 0 | 38 | |
Note: Data are presented as mean ± standard deviation (SD). Group comparisons were assessed using the independent-samples t-test; p < 0.05 considered significant (*). HFOV – high-frequency oscillatory ventilation; VAP – invasive ventilation; CPAP – continuous positive airway pressure; CA – chorioamnionitis, n – number of infants. | |||||||||
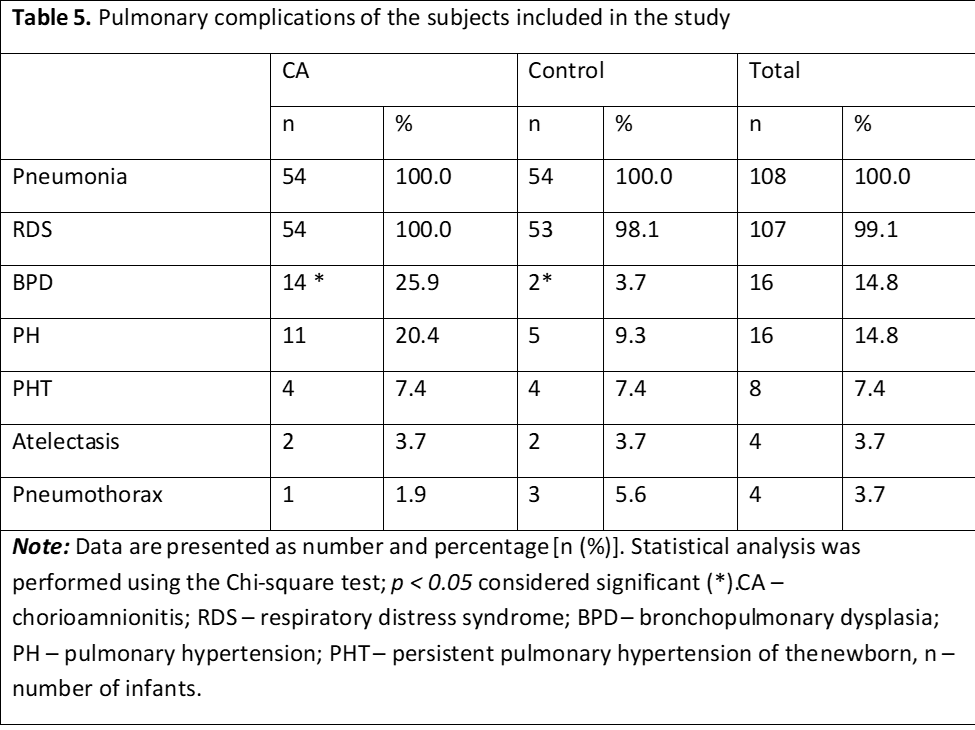
Pulmonary complications were common in both groups (Table 5). Respiratory distress syndrome (RDS) occurred in almost all infants (99%), with no significant difference between groups. However, bronchopulmonary dysplasia (BPD) was significantly more frequent among infants exposed to chorioamnionitis (25.9% vs. 3.7%, p < 0.05). The odds ratio for developing BPD in the CA group was approximately 9.1 (95% CI 1.9–42.3, p < 0.05), confirming a strong association between antenatal infection and chronic lung disease.
Pulmonary hypertension (PH) was also more prevalent in the CA group (20.4% vs. 9.3%), although this difference did not reach statistical significance (p > 0.05). Other complications such as atelectasis and pneumothorax occurred rarely and with similar frequency between groups.
Chi-square and Fisher’s exact tests confirmed the statistically significant correlation between chorioamnionitis and BPD (p = 0.001, Table 6, Figure 1). This relationship remained consistent after adjusting for gestational age and birth weight in logistic regression analysis, suggesting that intrauterine inflammation independently contributes to long-term pulmonary morbidity in preterm infants.
Table 6. Chi-Square Tests | ||||||
| Value | df | Asymptotic Significance (2-sided) | Exact Sig. (2-sided) | Exact Sig. (1-sided) | Point Probability |
Pearson Chi-Square | 10.565a | 1 | 0.001 | 0.002 | 0.001 | |
Continuity Correctionb | 8,878 | 1 | 0.003 | |||
Likelihood Ratio | 11,694 | 1 | 0.001 | 0.002 | 0.001 | |
Fisher's Exact Test | 0.002 | 0.001 | ||||
Linear-by-Linear Association | 10.467c | 1 | 0.001 | 0.002 | 0.001 | 0.001 |
N of Valid Cases | 108 | |||||
Note: Statistical output showing association between chorioamnionitis and BPD. Pearson Chi-square and Fisher’s exact tests were applied; p < 0.05 considered statistically significant. CA – chorioamnionitis; BPD – bronchopulmonary dysplasia. | ||||||
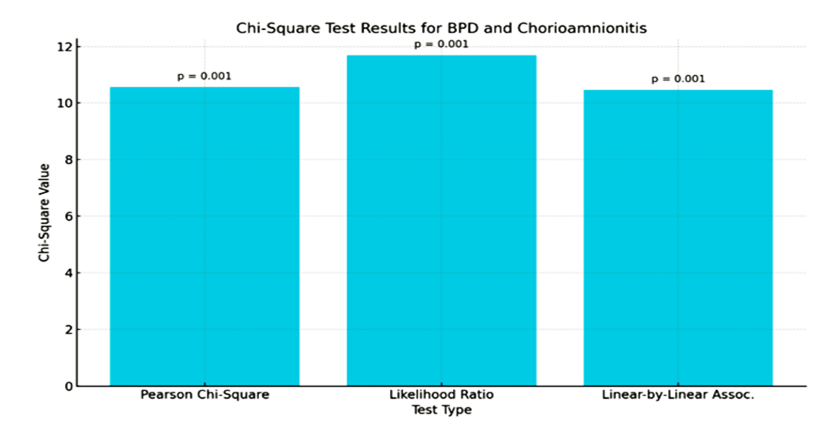 |
Fig. 1 Chi-square test for BPD and CA Note: Figure 1 represents association between chorioamnionitis and bronchopulmonary dysplasia in preterm infants. The figure demonstrates a significantly higher proportion of BPD in the CA-exposed group compared with controls (p < 0.05, Chi-square test). CA – chorioamnionitis; BPD – bronchopulmonary dysplasia. |
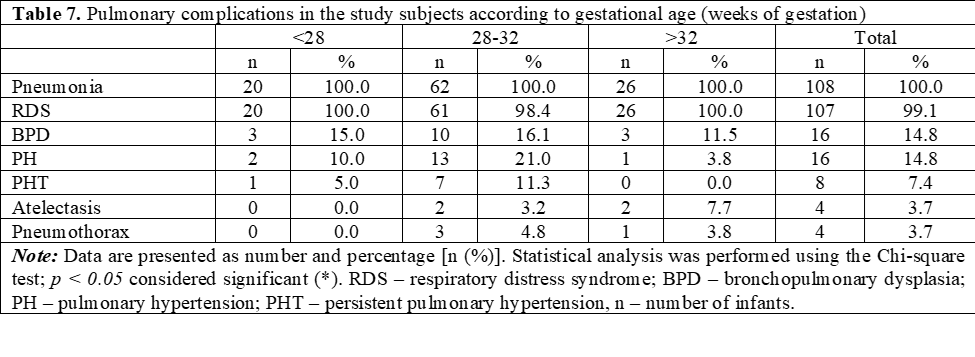
When stratified by gestational age (Table 7), RDS was similar in both groups (>98%). BPD occurred most frequently among very preterm infants (28–32 weeks, 16.1%), while PH was also predominant in this gestational subgroup (21.0%). These findings support the concept that both immaturity and antenatal inflammation contribute to disease severity.
Overall mortality did not differ significantly between groups (27.8% vs. 22.2%, p>0.05; Table 8). The majority of deaths occurred during theearly neonatal period (<7 days), accounting for 55.6% of all deaths, followed bylate neonatal deaths (40.7%). Only one death occurred in the post-neonatal period (>28 days). Although mortality rates were comparable, infants in the CA group showed a trend toward more severe respiratory morbidity and prolonged ventilation prior to death.
Table 8. Death of the subjects included in the study | ||||||
CA | Control | Total | ||||
n | % | n | % | n | % | |
No | 39 | 72.2 | 42 | 77.8 | 81 | 75.0 |
Yes | 15 | 27.8 | 12 | 22.2 | 27 | 25.0 |
<7 days | 7 | 46.7 | 8 | 66.7 | 15 | 55.6 |
8-28 days | 7 | 46.7 | 4 | 33.3 | 11 | 40.7 |
>28 days | 1 | 6.7 | 0 | 0.0 | 1 | 3.7 |
Total | 15 | 100.0 | 12 | 100.0 | 27 | 100.0 |
Note: Data are presented as number and percentage [n (%)]. Statistical analysis was performed using the Chi-square test; p < 0.05 considered significant (*). CA – chorioamnionitis; n – number of infants. | ||||||
Discussion
Our findings highlight a strong association between chorioamnionitis and adverse respiratory outcomes in preterm infants, particularly bronchopulmonary dysplasia (BPD). In our cohort, infants exposed to chorioamnionitis had a nearly nine-fold higher risk of BPD compared with controls, alongside lower Apgar scores, longer need for invasive ventilation, and prolonged hospitalization. Although the incidence of respiratory distress syndrome (RDS) was similar in both groups, the risk of long-term pulmonary morbidity was significantly increased in the chorioamnionitis group.
These results are consistent with international evidence from large systematic reviews and meta-analyses [5, 8-10]. A comprehensive meta-analysis including more than 244,000 infants found that both clinical and histological chorioamnionitis were associated with an increased risk of BPD, supporting the hypothesis that intrauterine inflammation predisposes the preterm lung to chronic injury [9]. Similarly, a 2024 systematic review and meta-regression confirmed that exposure to chorioamnionitis significantly increases the odds of BPD in preterm infants, irrespective of the specific diagnostic criteria used [5]. Another meta-analysis of 27 studies (~6,099 preterm infants) demonstrated that histologic chorioamnionitis (HCA) increases the risk of BPD (RR ~1.68; 95% CI 1.19–2.36). This supports our observation that histologic or more severe/inflammatory CA is more strongly linked to BPD [10].
Mechanistically, these associations can be explained by the concept of the “fetal inflammatory response syndrome.” Intrauterine infection induces the release of pro-inflammatory cytokines, which may stimulate surfactant production and transiently reduce RDS severity but simultaneously disrupt alveolar and vascular development. This dual effect has been termed the “chorioamnionitis paradox” [3]. Our findings reflect this paradox: although nearly all infants developed RDS regardless of exposure, those with chorioamnionitis progressed more frequently to BPD and pulmonary hypertension, suggesting that antenatal inflammation amplifies vulnerability to long-term respiratory complications.
Despite the strong association between CA and BPD in our study we did not observe a significant difference in mortality rates between groups. This contrasts with other studies, such as [4], which identify CA as a risk factor for combined adverse outcomes. In that study, infants born to mothers with acute and severe HCA had significantly higher rates of the composite outcome of BPD or death (60% vs 27%, p = 0.012) than infants without HCA. This finding helps illustrate the high burden when CA is severe.
Taken together, these data underscore the importance of early recognition and management of prolonged premature rupture of membranes and chorioamnionitis in obstetric practice, as well as the need to minimize invasive ventilation in affected neonates. Preventive strategies such as timely maternal antibiotic therapy, antenatal corticosteroids, and coordinated obstetric-neonatal management remain essential to reduce the burden of BPD [11].
Conclusions
Prolonged premature rupture of membranes is strongly associated with maternal chorioamnionitis, which significantly increases the risk of bronchopulmonary dysplasia and pulmonary hypertension in preterm infants. Early recognition, preventive strategies, and interdisciplinary management are essential to mitigate long-term respiratory morbidity.
Competing interests
None declared.
Authors’ contributions
LC contributed substantially to the conception and design of the study and also approved the final version to be published. LD contributed to acquisition of the data, substantial contributed to the analysis and interpretation of the collected data, drafting the article and taking responsibility for all aspects of the work. AC and LO also contributed to the analysis and interpretation of the data. ZS reviewed the article for intellectual content. The final approval was provided by NR and LC. All authors critically reviewed the work and approved the final version of the manuscript.
Acknowledgements and funding
No external funding
Ethics approval
The study protocol was approved by the Research Ethics Committee of Nicolae Testemițanu State University of Medicine and Pharmacy (decision No. 4/3.4 dated June 28, 2023).
Patient consent
Obtained.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Limitations of the study
This study has several limitations that should be acknowledged. First, the sample size was relatively small, and although all eligible preterm infants ≤34 weeks were included, the limited number of cases may reduce the statistical power, particularly for subgroup analyses. Second, this was a single-center study conducted in a Level III perinatal facility in Moldova, which may limit the generalizability of the findings to other settings or populations. Additionally, important inflammatory biomarkers (e.g., IL-6, IL-8, TNF-α) were not assessed, which limits the mechanistic interpretation of the association between chorioamnionitis and pulmonary outcomes. Potential confounding factors—including birth weight, gestational age distribution, ventilation strategies, nutritional practices, and timing of antenatal corticosteroid administration—may have influenced the risk of BPD despite adjustment attempts. Finally, follow-up was restricted to the NICU hospitalization period, and long-term respiratory or neurodevelopmental outcomes were not evaluated.
Authors’ ORCID IDs
Liuba Dascaliuc – https://orcid.org/0009-0002-0567-1762
Larisa Crivceanscaia – https://orcid.org/0000-0003-4388-374X
Ludmila Oclanscaia – https://orcid.org/0000-0001-7541-840X
Ninel Revenco – https://orcid.org/0000-0002-5229-7841
Angela Cracea – https://orcid.org/0000-0002-5283-1178
Zinaida Sârbu – https://orcid.org/0000-0003-3916-5630
References
Moreira A, Noronha M, Joy J, Bierwirth N, Tarriela A, Naqvi A, Zoretic S, Jones M, Marotta A, Valadie T, Brick J. Rates of bronchopulmonary dysplasia in very low birth weight neonates: a systematic review and meta-analysis. Respir Res. 2024 May 24;25(1):219. doi: 10.1186/s12931-024-02850-x.
Ito M, Kato S, Saito M, Miyahara N, Arai H, Namba F, Ota E, Nakanishi H. Bronchopulmonary dysplasia in extremely premature infants: a scoping review for identifying risk factors. Biomedicines. 2023 Feb 14;11(2):553. doi: 10.3390/biomedicines11020553.
Yu H, Li D, Zhao X, Fu J. Fetal origin of bronchopulmonary dysplasia: contribution of intrauterine inflammation. Mol Med. 2024 Sep 3;30(1):135. doi: 10.1186/s10020-024-00909-5.
Costa S, Fattore S, De Santis M, Lanzone A, Spanu T, Arena V, Tana M, Trapani M, Sanguinetti M, Barnea ER, Vento G. Effect of acute histologic chorioamnionitis on bronchopulmonary dysplasia and mortality rate among extremely low gestational age neonates: A retrospective case–control study. Int J Gynecol Obstet. 2024 Jun;165(3):1040-6. doi: 10.1002/ijgo.15290.
Liu WL, Zhou Y, Zhang C, Chen J, Yin XF, Zhou FX, Chen SJ. Relationship between chorioamnionitis or funisitis and lung injury among preterm infants: meta-analysis involved 16 observational studies with 68,397 participants. BMC Pediatr. 2024 Mar 5;24(1):157. doi: 10.1186/s12887-024-04626-0.
Committee on Obstetric Practice. Committee opinion no. 712: intrapartum management of intraamniotic infection. Obstet Gynecol. 2017;130(2):e95-101. doi: 10.1097/AOG.0000000000002236.
Goldenberg RL, Culhane JF, Iams JD, Romero R. Epidemiology and causes of preterm birth. Lancet. 2008;371(9606):75-84. doi: 10.1016/S0140-6736(08)60074-4.
Yu Z, Wang L, Wang Y, Zhang M, Xu Y, Liu A. Development and validation of a risk scoring tool for bronchopulmonary dysplasia in preterm infants based on a systematic review and meta-analysis. Healthcare (Basel). 2023;11(5):778. doi: 10.3390/healthcare11050778.
Carter SW, Neubronner S, Su LL, Dashraath P, Mattar C, Illanes SE, Choolani MA, Kemp MW. Chorioamnionitis: an update on diagnostic evaluation. Biomedicines. 2023 Oct 28;11(11):2922. doi: 10.3390/biomedicines11112922.
Jain VG, Parikh NA, Rysavy MA, Shukla VV, Trotta M, Jobe A, Carlo WA, Ambalavanan N. Histological chorioamnionitis increases the risk of bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2024 May 15;209(10):1272-5. doi: 10.1164/rccm.202311-2084LE.
Pereira-Fantini PM, Tingay D, Lakshminrusimha S. A complex inflammatory mix: chorioamnionitis, antenatal steroids and early postnatal budesonide. Pediatr Res. 2024 Aug;96(3):560-2. doi: 10.1038/s41390-024-03219-y.