
Introduction
Acute type A aortic dissection is a major cardiovascular emergency characterized by separation of the aortic wall layers with the formation of a false lumen, leading to rapid compromise of perfusion to vital organs. This condition follows a fulminant course and carries an extremely high mortality in the absence of timely intervention. Studies have shown that mortality approaches 50% within the first 48 hours and may reach up to 90% at 30 days if surgery is not performed [1]. The natural history of type A aortic dissection is catastrophic, and the 2024 EACTS/STS guidelines recommend urgent surgical intervention in nearly all patients [2].
The etiology of acute aortic dissection is most often related to uncontrolled hypertension, responsible for approximately 70% of cases [3]. The remaining 30% are attributed to factors such as pre-existing aortic aneurysms, connective tissue disorders (e.g., Marfan syndrome, Ehlers–Danlos syndrome), or thoracic trauma [4]. Although traditionally considered a disease of the elderly, recent years have seen an increasing incidence in younger patients. Recent data indicate that nearly 45% of individuals diagnosed with acute aortic dissection are under 60 years of age [4, 5]. These findings highlight the importance of maintaining a high index of clinical suspicion, prompt use of diagnostic imaging, and rapid multidisciplinary intervention to reduce morbidity and mortality associated with this critical pathology.
Nevertheless, diagnosis of aortic dissection is often delayed, which negatively influences clinical outcomes and prognosis. Differential diagnosis is challenging, with nearly half of patients initially misdiagnosed and approximately one-third receiving inappropriate treatment, most often for acute coronary syndrome due to overlapping clinical presentations [6]. According to the IRAD registry, perioperative mortality has declined with the adoption of modern standardized strategies, including careful selection for root replacement and the use of valve-sparing techniques, decreasing from 25% to 18% [7].
Several surgical strategies are available for type A aortic dissection, ranging from valve preservation to valve replacement. The choice depends on valve status, the extent of root involvement, patient profile, and a careful balance between the risks of extensive repair and the potential need for complex reintervention. Proximal treatment has evolved from supracoronary replacement with or without valve replacement (Wheat) to composite graft replacement of both the root and valve (Bentall), and more recently to valve-sparing techniques, such as remodeling (Yacoub) and reimplantation (Tirone David) [8].
According to contemporary guidelines, complete root with valve replacement is recommended in acute type A aortic dissection when the intimal tear is located at the root, in the presence of significant tissue fragility, or when the aortic valve is irreparable, while valve-sparing root replacement remains a reasonable option in carefully selected patients, provided the surgery is performed in centers with appropriate expertise [9]. Similarly, the 2024 ACC/AHA guidelines emphasize that the decision between valve-sparing root replacement and the Bentall procedure should be individualized based on cusp integrity, the extent of root involvement, and the surgical expertise of the treating center [10].
Tirone David introduced the technique of aortic root reconstruction with valve preservation in the early 1990s. Initially applied in the elective surgery of ascending aortic aneurysms, the technique was subsequently extended to acute type A aortic dissection [11, 12]. The Tirone David procedure is indicated when the cusps are normal or repairable (without significant calcification or degeneration), and the root, although dissected or dilated, can be reconstructed within a prosthetic graft to restore geometry. It is preferred in younger patients, in those with connective tissue disorders, or with a repairable bicuspid valve; however, it requires sufficient hemodynamic stability and institutional expertise [12].
The Bentall procedure is generally preferred when the aortic valve is deemed irreparable, such as in the presence of extensive calcification, cusp destruction, or severe prolapse. It is also indicated when the aortic root exhibits major structural loss or a dissecting extension that precludes reliable reconstruction, as well as in critically ill patients where operative simplicity and time efficiency are paramount [8].
In contrast, the Wheat procedure offers an alternative in situations where the valve must be replaced but the aortic root can be preserved. By maintaining the root, proximal anastomosis time is reduced, making this option particularly useful in unstable patients with favorable proximal anatomy, when the dissection is confined to the ascending aorta with an intact root and progressive dilatation is not anticipated [12].
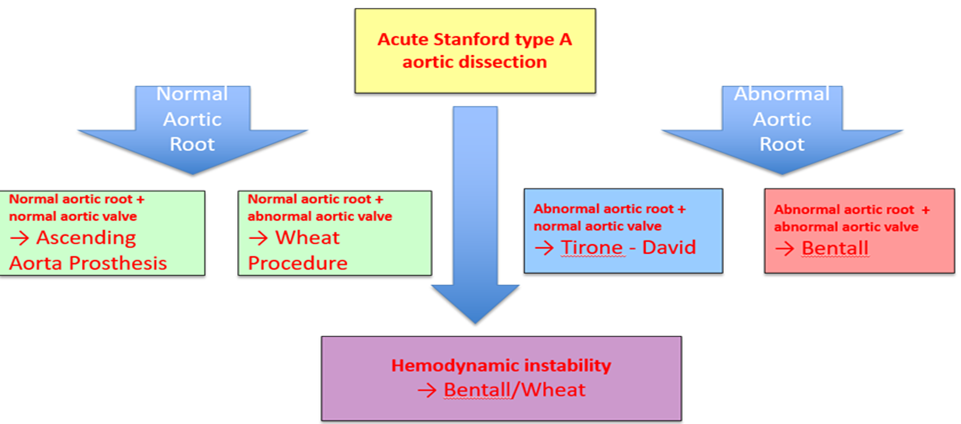 |
Fig. 1 Decisional algorithm. |
Table 1. Comparative indications: Tirone David vs Bentall. | ||
| Tirone David | Bentall |
| Aortic valve status | Anatomically normal valve or with minimal repairable lesions; no significant calcification/degeneration | Irreparable valve: calcified, severe stenosis, destroyed cusps, massive prolapse, or irreparable regurgitation |
| Root involvement in dissection | Affected/dilated root, but coaptation can be restored within a prosthetic graft (favorable geometry) | Root with major structural destruction or anatomically impossible to reconstruct |
| Patient profile | Young patient, long life expectancy; priority to avoid lifelong anticoagulation and preserve physiological hemodynamics | Critically ill patient where procedural simplicity and rapidity are essential, or where anticoagulation is not a concern |
| Connective tissue disorders (Marfan / Loeys–Dietz) | Preferred if valve is repairable; good results in experienced centers | Standard when the valve is compromised or anatomy unfavorable for reconstruction |
| Bicuspid aortic valve | Repairable bicuspid valve (favorable commissural/geometry relationships) | Irreparable or extensively calcified bicuspid valve |
| Perioperative priorities | Recommended when patient’s condition allows a more complex procedure and expertise is available for Tirone David | Preferred when a rapid/standardized solution is required (shock, visceral/neurological ischemia) or the team lacks experience |
| Postoperative anticoagulation | Avoided (native valve preserved); advantageous in patients at risk of bleeding or with contraindications to anticoagulation | Required if a mechanical prosthesis is used; biological prosthesis possible but with lower durability |
| Surgeon’s expertise | Requires high expertise in valve and root surgery; outcomes depend on center’s volume and experience | Standardized technique, shorter learning curve, applicable in most centers |
Material and methods
This is a single-center, retrospective observational study conducted at the Prof. Dr. George I.M. Georgescu Institute of Cardiovascular Diseases “” in Iași (IBCV Iași), a national reference center for cardiovascular surgery in Romania. The analysis included all cases of acute type A aortic dissection treated surgically at this institution over a 25-year period, from January 2000 to January 2025, providing a large and valuable dataset of clinical and operative information.
Depending on the anatomical and hemodynamic characteristics of each case, as well as the evolution of therapeutic protocols over time, patients were managed using one of the following surgical strategies:
Aortic root replacement with a valved conduit (Bentall procedure), the standard technique in cases where both the aortic valve and root were compromised by dissection or severe aneurysmal dilatation;
Valve-sparing aortic root replacement (Tirone David procedure), applied especially in younger patients or those with a competent tricuspid aortic valve, in order to preserve native valve function and avoid prosthetic valve implantation;
Segmental replacement of the ascending aorta, indicated when the dissection was confined to this segment without root or valve involvement;
Ascending aortic and valve replacement with preservation of the aortic bulb (Wheat procedure).
Results
Preoperative Data. A total of 256 cases of acute type A aortic dissection were surgically treated at IBCV Iași over the 25-year study period. The number of cases operated in our institution followed an upward trend, with an average of 11 interventions per year, increasing in the last decade (2014-2024) to an annual mean of 15 cases, reflecting both increased referral and improved diagnostic and surgical capacity.
Most patients were male (69%), presenting at significantly younger ages compared to women (mean age 50.3 vs. 58.2 years). The overall mean age of the cohort was 55.8 years, lower than that reported in international literature, which may reflect a predisposition of the Romanian population to develop aortic dissections at younger ages, possibly associated with low adherence to antihypertensive therapy.
Regarding timing of presentation, the majority of patients arrived at our institution within 6-12 hours from symptom onset, a favorable factor for early surgical intervention. Arterial hypertension was the main identified risk factor, present in 75% of patients, followed by ascending aortic aneurysm associated with bicuspid aortic valve.
Table 2. Preoperative parameters. | |
Parameter | Value |
Mean age (years) | 55.8 |
Male sex | 69% |
Arterial hypertension | 75% |
Cardiogenic shock at presentation | 18.3% |
Pericardial effusion | 20% |
Oliguria | 16.9% |
Severe aortic regurgitation | 48% |
Ascending aorta diameter (mm) | 45 |
Aortic annulus diameter (mm) | 24.5 |
Symptom onset to admission interval | 6–12 hours |
Left ventricular ejection fraction (%) | 51 |
Echocardiographic data.
Preoperative evaluation revealed that 20% of patients presented with pericardial effusion, with or without signs of cardiac tamponade, 18.3% were in cardiogenic shock, and 16.9% had oliguria. The mean left ventricular ejection fraction was 51%, and 48% of patients exhibited grade III-IV aortic regurgitation. The mean diameter of the ascending aorta was 45 mm, while the aortic annulus measured an average of 24.5 mm.
Surgical technique.From a technical standpoint, most procedures aimed at preserving the native aortic valve (73%), while 10% of patients underwent the Bentall procedure and 17% the Wheat operation. A rising trend in valve-sparing procedures was observed, reaching 84% over the past four years.
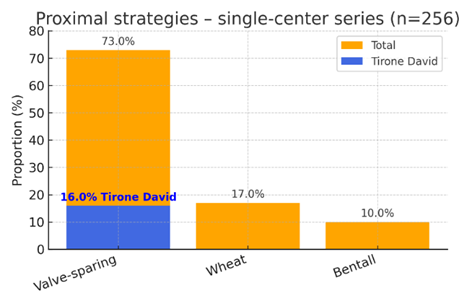 |
Fig. 2 Operative strategy. |
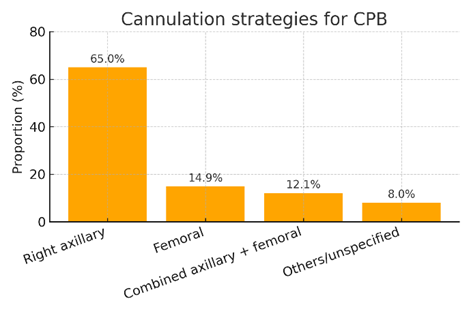
With regard to arterial cannulation strategy for cardiopulmonary bypass, the right axillary approach was considered the standard, employed in 65% of interventions, followed by femoral cannulation (14.9%) and combined axillary-femoral cannulation (12.1%). Myocardial protection was provided in most cases using combined antegrade and retrograde cardioplegia, with a mean cardiopulmonary bypass time of 264 minutes and a mean aortic cross-clamp time of 160 minutes.
|
Fig. 3 Cannulation strategies |
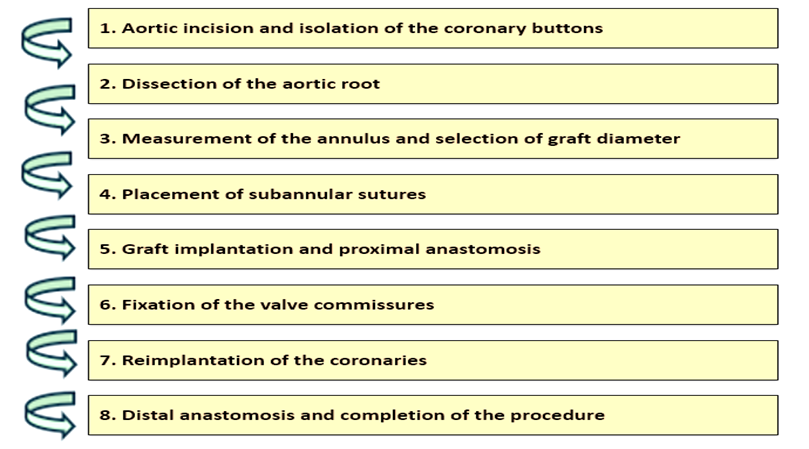 |
Fig. 4 Surgical Protocol Steps – Tirone David Procedure |
The following summarizes the operative protocol for the Tirone David technique (Figure 4)
Aortic incision and evaluation of the aortic valve cusps
The dilated ascending aorta is resected, leaving approximately 7-8 mm of aortic tissue at the base of the cusps.
The coronary buttons (left and right) are excised and mobilized, then retracted with stay sutures.
Isolation of the coronary buttons (Figure 5)
The ostia of the coronary arteries are identified.
The coronary buttons are isolated with a margin of 4-5 mm of aortic tissue.
Dissection of the aortic root (Figure 5)
The aortic root is carefully separated from the pulmonary artery.
Dissection is continued circumferentially down to the level of the aortic annulus, sometimes slightly below it.
 |
Fig. 5 Aortic root dissection and isolation of the coronary buttons |
Graft measurement and selection (Figure 6)
A Hegar dilator is passed through the valve to determine the diameter of the left ventricular outflow tract.
Several methods are available for estimating the optimal prosthetic diameter. The simplest approach is to select a Dacron graft whose size equals the dilator diameter plus approximately 11 mm.
In practice, the final graft diameter usually ranges from 32 to 38 mm.
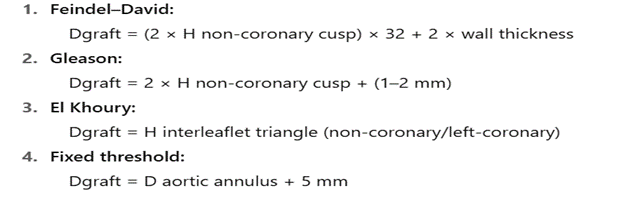 |
Fig. 6 Methods for estimating the optimal prosthetic diameter |
Placement of subannular sutures (Figure 7)
Twelve to fifteen circumferential mattress sutures (2-0 Ethibond/Astralene) are placed beneath the aortic annulus, with one suture positioned under each commissure.
Care should be taken to avoid penetrating the endothelium, while ensuring even spacing of the sutures.
 |
Fig, 7 Subannular sutures placement |
Graft implantation
The graft is marked at 120° and the subannular sutures are passed through it. It is then lowered so that the annulus and valve are completely included within.
The sutures are tied progressively, while maintaining the Hegar dilator in place to prevent narrowing of the outflow tract.
Resuspension of the valve commissures (Figure 8)
The valve cusps are repositioned, and each commissure is anchored to the graft with 4-0 polypropylene sutures.
Cusp coaptation is verified by irrigating with cold solution; if prolapse is present, the commissure position is adjusted or the affected cusp is suspended.
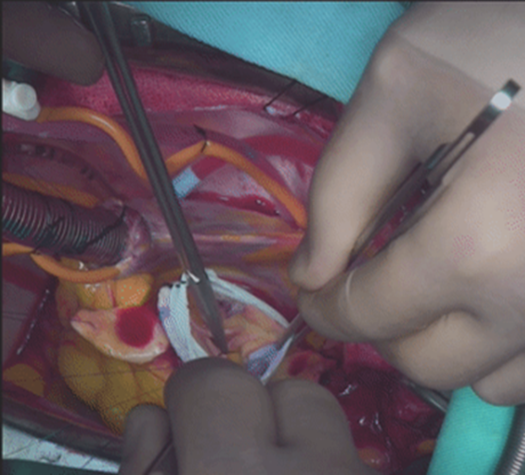 |
Fig. 8 Resuspension of the valve commissures |
Reimplantation of the coronary arteries (Figure 9)
Openings (neo-sinuses) are created in the graft for the coronary buttons.
Coronary anastomoses are performed with fine sutures (5-0 polypropylene), ensuring uniform and watertight suture lines.
If necessary, an external biological adhesive is applied for sealing.
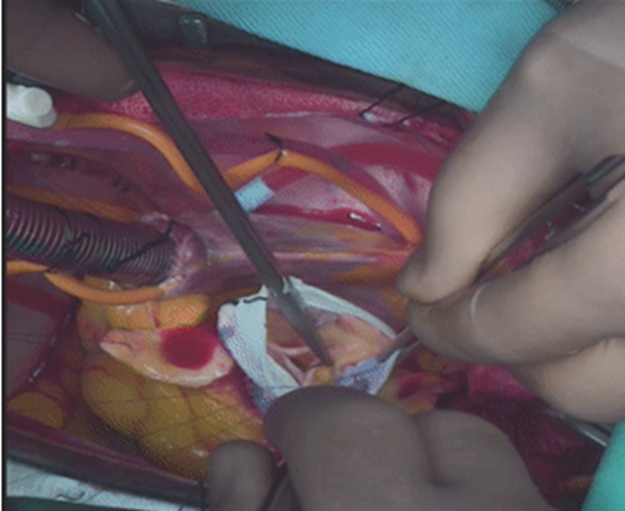 |
Fig. 9 Reimplantation of the coronary arteries |
Completion of the procedure (Figure 10)
The integrity of the reconstruction, valve coaptation, and absence of regurgitation are verified.
Continuity with the distal aorta is restored, usually by means of a hemi-arch or ascending aortic anastomosis.
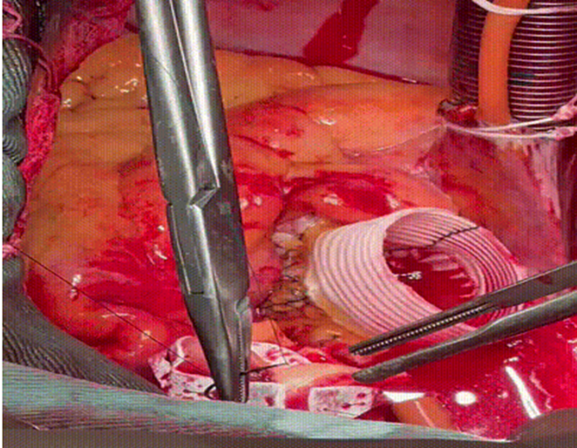 |
Fig. 10 Distal anastomosis |
Postoperative results.
The presented data show that surgical intervention is associated with significant postoperative morbidity, with the most frequent complications being acute renal insufficiency (21.47%) and the need for hemodialysis (16.77%), highlighting the major impact on renal function and hemodynamic balance. Arrhythmias complicated the postoperative course in 18% of patients, the most common being atrial fibrillation. Infections, both respiratory (14.14%) and other types (17.17%), occurred in a substantial proportion of patients, reflecting postoperative vulnerability and prolonged hospitalization. Neurological (9.95%) and hemorrhagic (11.32%) complications were less frequent but potentially severe. The mean intensive care unit stay of 9.81 days and the total hospital stay of 17.09 days confirm the complexity of these cases and emphasize the need for dedicated preventive and management strategies to reduce renal, infectious, and arrhythmic risks in order to improve patient prognosis.
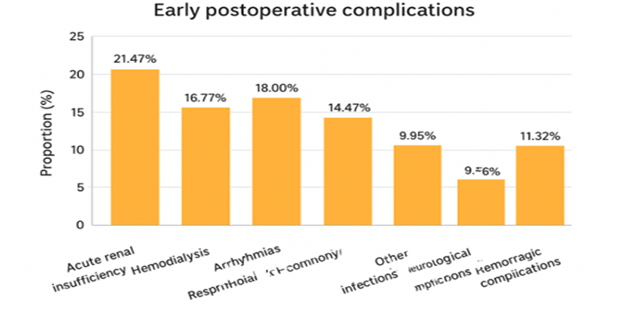 |
Fig. 11 Early postoperative complications |
In the analyzed cohort, mortality was 13.7%, with a decreasing trend observed in recent years, reflecting progressive improvement in therapeutic outcomes achieved in our center.
Table 3. Early postoperative complications | |
Parameter | Value |
| Perioperative mortality | 13.7 % |
| Acute renal insufficiency | 21.5 % |
| Hemodialysis | 16.8 % |
| Atrial fibrillation | 18 % |
| Respiratory infection | 14.14 % |
| Other infections | 17.17 % |
| Neurological complications | 9.95 % |
| Bleeding requiring re-exploration | 11.32 % |
| Length of intensive care stay (days) | 9.81 |
| Total hospital stay (days) | 17.09 |
Discussions
The modern surgical treatment of aortic root pathology has evolved significantly over the past decades, beginning with the classic Bentall–De Bono procedure, which involves complete replacement of the aortic root and valve followed by reimplantation of the coronary ostia into a composite valved conduit [1]. Subsequently, techniques designed to preserve the native valve were developed, such as Robicsek aortoplasty, the Yacoub procedure (aortic root remodeling), and the David procedure (valve reimplantation into a tubular graft) [13]. In 2007, Hetzer proposed another technique – aortic valve relocation – further expanding the therapeutic armamentarium of the cardiovascular surgeon [14].
The choice of the most appropriate surgical technique in the setting of acute aortic root dissection has long been controversial. In this regard, Tirone David emphasized that dissections should be managed similarly to elective cases, advocating that aortic valves with normal or repairable cusps should be preserved, regardless of the degree of sinus involvement [14].
Over time, several variants of the David procedure have been developed, adapted to the patient’s anatomic and clinical context. Its main advantage lies in the surgical flexibility it provides, allowing for a personalized approach in each case. In a retrospective analysis from the University of Michigan (Ann Arbor), comparing 307 David procedures with 184 Bentall procedures, both techniques showed good short- and long-term results, without significant differences in mortality or reintervention rates [15]. The authors emphasized that aortic root replacement should be reserved for cases with intimal tear at the root, aneurysm ≥ 45 mm, irreparable aortic valve disease, or connective tissue disorders [15]. Although the use of the David procedure in the emergency setting was initially controversial, data published by Beckmann et al. demonstrated that while immediate postoperative mortality is higher in acute dissection patients, long-term survival is comparable to that of electively operated patients [16]. Furthermore, freedom from valve reintervention at 1, 5, 10, and 15 years was excellent: 97%, 93%, 88%, and 85%, respectively [16].
Recent meta-analyses show equivalent survival between the Tirone David and Bentall procedures, with a higher risk of reintervention after Tirone David – a risk dependent on patient selection, aortic geometry, and the quality of reconstruction [17]. Contemporary series suggest excellent durability with a standardized and meticulous technique. Similarly, a comparative study from Leipzig concluded that, in the hands of experienced surgeons, the David procedure provides survival equivalent to Bentall when selectively applied according to patient-specific factors [18].
Patient subgroups
Young patients and those with connective tissue disorders – The Tirone David procedure is recommended when cusps are morphologically normal or repairable [2]. Avoidance of lifelong anticoagulation, preservation of physiologic root hemodynamics, and complete resection of diseased aortic wall are strong arguments for valve preservation, particularly in Marfan or Loeys–Dietz patients with intact cusps [11]. Modern studies show that, in emergency settings, the David procedure may be chosen as a first-line strategy in carefully selected patients with stable preoperative status; consecutive series report mortality comparable to alternative techniques and stable mid-term valve function, despite longer CPB times [11, 15]. Standardized cerebral protection and cannulation strategies (e.g., right axillary cannulation with selective antegrade cerebral perfusion) support extended approaches in young patients, reducing the neurological burden of more complex procedures. In our series, valve preservation was chosen in 73% of cases (84% in the past 4 years), especially in young patients and those with connective tissue disorders, provided that intraoperative evaluation confirmed repairable cusps and a sino-tubular junction that could be reliably reconstructed with a stable prosthetic graft.
Bicuspid aortic valve – The David procedure is feasible in bicuspid aortic valves if near-180° commissural symmetry and an effective cusp height of ~9-10 mm can be achieved, with targeted prolapse correction (central plication) as needed [19-21]. The literature highlights that success in bicuspid valves depends on reconstructed geometry (commissural angle, restoration of the base and sino-tubular junction). Once these are secured, residual insufficiency is reduced and durability is acceptable [21]. Conversely, extensive calcification, thickened cusps, or uncorrectable commissural ratios direct the choice toward Bentall, where a standardized approach can be more easily applied [8]. For cases with fragile or dissected coronary buttons, modern reimplantation techniques and interposition options (Cabrol/Piehler) can prevent tension and stabilize root reconstruction when the David procedure is not indicated [22, 23]. In our practice, bicuspid patients were candidates only when intraoperative evaluation demonstrated proper commissural symmetry and cusp coaptation without regurgitation; otherwise, we favored Bentall to avoid early reintervention.
Hemodynamically unstable patients or those with malperfusion – In the presence of hemodynamic shock, preoperative resuscitation, tamponade with imminent collapse, or severe visceral/neurological malperfusion, the priority is rapid and secure proximal control using a standardized technique with predictable hemostasis. In these circumstances, Bentall (or, in strictly selected cases, Wheat) provides a shorter option, with robust proximal annular sutures and complete resection of dissected tissue, reducing the risk of proximal reintervention compared with partial root repairs [2]. Contemporary algorithms for acute type A dissection explicitly include “non-David bailout” strategies when critical status and/or complex distal anatomy jeopardize safety. In such situations, axillary cannulation (sometimes combined) and selective cerebral perfusion remain key to controlling neurological risk during circulatory arrest [24]. In our series, where right axillary cannulation was standard (65%), the same criterion was applied: David only for stabilized patients with repairable cusps; Bentall/Wheat when every minute saved and proximal hemostasis were paramount.
Profile of our series. The profile of our cohort (mean age 55.8 years; 69% male; presentation frequently within the first 6-12 hours; 48% severe aortic insufficiency; 73% David procedure; overall mortality 13.7% with a downward trend) is consistent with the literature, which demonstrates that careful selection allows extension of the David procedure to acute type A dissection without compromising safety, at the cost of a learning curve and longer cross-clamp/CPB times. In cases where the valve and/or root cannot be reconstructed within acceptable geometric parameters, systematic application of the Bentall technique (secure proximal hemostatic construction, appropriate graft/valve choice, tension-free coronary button reimplantation, interposition options) ensures robust outcomes and a reliable platform for high-risk emergencies.
Table 4. Major outcomes of the Tirone David procedure in acute type A aortic dissection | |||||
Study | Design/Center | n | Early mortality | Reintervention | Reference |
Tanaka 2018, EJCTS | Observational | 24 Tirone David | 0% | 7–10% | Tanaka H, et al. Outcomes of VSRR in acute Type A dissection. Eur J Cardiothorac Surg. 2018;53:1021–1026. doi:10.1093/ejcts/ezx463 |
Beckmann 2023, AnnalsCTS | Review | 133 | 12.8% | Not specified | Beckmann E, Kaufeld T, Martens A, Rudolph L, Shrestha M, Krueger H, Haverich A, Shrestha ML. Aortic valve-sparing root replacement (David-I) for acute aortic dissection type A. Ann Cardiothorac Surg. 2023;12(3):276–278. doi:10.21037/acs-2022-avs1-168 |
Sá 2023, Int J Cardiol (meta) | Meta-analysis (7 studies) | 367 Tirone David vs 491 Bentall | Similar between David vs Bentall | Higher risk after David vs Bentall | Sá MP, et al. Long-term outcomes of VSRR vs composite valve graft in ATAAD: meta-analysis. Int J Cardiol. 2023;382:12–19. doi:10.1016/j.ijcard.2023.03.062 |
Aubin/Kamiya 2019, Front Surg | Review | 28 | 17.9% | 0% | Aubin H, Kamiya H, et al. Valve-Sparing Aortic Root Replacement as First-Choice Strategy in ATAAD. Front Surg. 2019;6:1-9 |
Conclusions
In acute type A aortic dissection, the Tirone David procedure represents our operation of choice whenever the aortic cusps are intact or amenable to repair, the aortic root is not excessively fragile and allows for safe reconstruction, and the patient’s clinical status tolerates the additional operative time. Conversely, the Bentall procedure remains the optimal option in the presence of irreparable cusps, markedly fragile tissue, or profound hemodynamic instability. Right axillary cannulation constitutes our institutional standard.
When – The Tirone David procedure is favored when cusp repairability and root reconstructability are feasible; the Bentall operation is selected when the valve is irreparable, tissue integrity is compromised, or rapid operative completion is essential.
How – Strict procedural standardization, including correct commissural orientation and accurate prosthesis sizing, is fundamental to ensure long-term durability.
Why – Preservation of physiological hemodynamics and avoidance of lifelong anticoagulation justify the use of the Tirone David procedure in carefully selected patients. In contrast, the Bentall procedure provides greater simplicity and predictability in cases with unfavorable anatomy or hemodynamic compromise.
Our patient series supports the feasibility of the Tirone David operation in the setting of acute type A aortic dissection, with an operative mortality of 13.7% and a favorable downward trend over time.
Competing interests
None declared.
Authors’ contributions
GT conceived the study, supervised the project, and critically revised the manuscript. ME contributed to study design, collected clinical data, and drafted parts of the manuscript. AȚ participated in surgical procedures, data acquisition, and interpretation. AB and SS contributed to perioperative data collection, analysis, and manuscript drafting. AB assisted in statistical analysis, data processing, and preparation of figures and tables. All authors reviewed the work critically, approved the final version of the manuscript, and agree to be accountable for all aspects of the work.
Patient consent
Obtained.
Ethics approval
The study was approved by the Research Ethics Committee of Professor Dr. George I.M. Georgescu Institute of Cardiovascular Diseases, Iasi, Romania (approval number 2185 / 2024-07-26).
Acknowledgements and funding
No external funding.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Authors’ ORCID IDs
Grigore Tinică – https://orcid.org/0000-0002-1755-9674
Mihail Enache – https://orcid.org/0000-0003-3133-3900
Andrei Țărus – https://orcid.org/0000-0001-9428-0637
Silviu Stoleriu – https://orcid.org/0009-0003-3905-919X
Alberto Bacușcă – https://orcid.org/0000-0002-8965-4072
References
Bentall H, De Bono A. A technique for complete replacement of the ascending aorta. Thorax. 1968;23(4):338-9. doi: 10.1136/thx.23.4.338.
Czerny M, Grabenwöger M, Berger T, Aboyans V, Della Corte A, Chen EP, et al. EACTS/STS Guidelines for diagnosing and treating acute and chronic syndromes of the aortic organ. Ann Thorac Surg. 2024;118(1):5-115. doi: 10.1016/j.athoracsur.2024.01.021.
David TE. Aortic valve sparing operations. Ann Thorac Surg. 2002;73(4):1029-30. doi: 10.1016/s0003-4975(02)03487-2.
Shi W, Keefe M, Matalanis G. Valve-sparing aortic root replacement and aortic valve repair [Internet]. In: Motomura N, ed. Aortic valve surgery. London: InTech; 2011 [cited 2025 Jun 14]. Available from: http://dx.doi.org/10.5772/21219.
David TE. Aortic valve sparing operations: a review. J Chest Surg. 2012;45(4):205-12. doi: 10.5090/kjtcs.2012.45.4.205.
Tian D, Rahnavardi M, Yan TD. Aortic valve sparing operations in aortic root aneurysms: remodeling or reimplantation? Ann Cardiothorac Surg. 2013;2(1):44-52. doi: 10.3978/j.issn.2225-319X.2013.01.14.
Pape LA, Awais M, Woznicki EM, Suzuki T, Trimarchi S, Evangelista A, et al. Presentation, diagnosis, and outcomes of acute aortic dissection: 17-year trends from the International Registry of Acute Aortic Dissection. J Am Coll Cardiol. 2015;66(4):350-8. doi: 10.1016/j.jacc.2015.05.029.
Ohira S, Cameron DE, Lansman SL, Spielvogel D. Complex Bentall operation: clinical pearls to standardize the procedure. Ann Thorac Surg. 2025;119(4):744-54. doi: 10.1016/j.athoracsur.2024.09.013.
Angelos P, Taylor LJ, Roggin K, Schwarze ML, Vaughan LM, Wightman SC, et al. Decision-making in surgery. Ann Thorac Surg. 2024;117(6):1087-94. doi: 10.1016/j.athoracsur.2024.01.001.
Isselbacher EM, Preventza O, Hamilton Black J, 3rd, Augoustides JG, Beck AW, Bolen MA, et al. 2022 ACC/AHA Guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022;146(24):e334-e482. doi: 10.1161/cir.0000000000001106.
Aubin H, Akhyari P, Rellecke P, Pawlitza C, Petrov G, Lichtenberg A, et al. Valve-sparing aortic root replacement as first-choice strategy in acute type A aortic dissection. Front Surg. 2019;6:46. doi: 10.3389/fsurg.2019.00046.
Ahmed EM, Chen E. Valve sparing aortic root replacement for aortic valve insufficiency in type A aortic dissection. In: Sellke FW, et al., editors. Aortic dissection and acute aortic syndromes. Cham: Springer; 2021. p. 269-282. doi: 10.1007/978-3-030-66668-2_19.
Yacoub MH, Gehle P, Chandrasekaran V, Birks EJ, Child A, Radley-Smith R. Late results of a valve-preserving operation in patients with aneurysms of the ascending aorta and root. J Thorac Cardiovasc Surg. 1998;115(5):1080-90. doi: 10.1016/s0022-5223(98)70408-8.
David T. Reimplantation valve-sparing aortic root replacement is the most durable approach to facilitate aortic valve repair. JTCVS Techniques. 2021;7:72-8. doi: 10.1016/j.xjtc.2020.12.042.
Yang B, Norton EL, Hobbs R, Farhat L, Wu X, Hornsby WE, et al. Short- and long-term outcomes of aortic root repair and replacement in patients undergoing acute type A aortic dissection repair: twenty-year experience. J Thorac Cardiovasc Surg. 2019;157(6):2125-36. doi: 10.1016/j.jtcvs.2018.09.129.
Beckmann E, Kaufeld T, Martens A, Rudolph L, Shrestha M, Krueger H, et al. Aortic valve-sparing root replacement (David-I) for acute aortic dissection type A. Ann Cardiothorac Surg. 2023;12(3):276-8. doi: 10.21037/acs-2022-avs1-168.
Sá MP, Tasoudis P, Jacquemyn X, Van den Eynde J, Rad AA, Weymann A, et al. Long-term outcomes of valve-sparing root versus composite valve graft replacement for acute type A aortic dissection: meta-analysis of reconstructed time-to-event data. Int J Cardiol. 2023;382:12-9. doi: 10.1016/j.ijcard.2023.03.062.
Subramanian S, Leontyev S, Borger MA, Trommer C, Misfeld M, Mohr FW. Valve-sparing root reconstruction does not compromise survival in acute type A aortic dissection. Ann Thorac Surg. 2012;94(4):1230-4. doi: 10.1016/j.athoracsur.2012.04.094.
Jahanyar J, de Kerchove L, El Khoury G. Bicuspid aortic valve repair: the 180°-reimplantation technique. Ann Cardiothorac Surg. 2022;11(4):473-81. doi: 10.21037/acs-2022-bav-18.
Schäfers HJ, Bierbach B, Aicher D. A new approach to the assessment of aortic cusp geometry. J Thorac Cardiovasc Surg. 2006;132(2):436-8. doi: 10.1016/j.jtcvs.2006.04.032.
Bierbach BO, Aicher D, Issa OA, Bomberg H, Gräber S, Glombitza P, et al. Aortic root and cusp configuration determine aortic valve function. Eur J Cardiothorac Surg. 2010;38(4):400-6. doi: 10.1016/j.ejcts.2010.01.060.
Aphram G, Tamer S, Mastrobuoni S, El Khoury G, de Kerchove L. Valve sparing root replacement: reimplantation of the aortic valve. Ann Cardiothorac Surg. 2019;8(3):415-7. doi: 10.21037/acs.2019.04.05.
Piehler JM, Pluth JR. Replacement of the ascending aorta and aortic valve with a composite graft in patients with nondisplaced coronary ostia. Ann Thorac Surg. 1982;33(4):406-9. doi: 10.1016/s0003-4975(10)63239-0.
Leshnower BG, Myung RJ, Kilgo PD, Vassiliades TA, Vega JD, Thourani VH, et al. Moderate hypothermia and unilateral selective antegrade cerebral perfusion: a contemporary cerebral protection strategy for aortic arch surgery. Ann Thorac Surg. 2010;90(2):547-54. doi: 10.1016/j.athoracsur.2010.03.118.